Ecmo
Reading File
Finding Sources
Searching PubMed
"extracorporeal membrane oxygenation" AND outcomes
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Here is a thorough overview of ECMO drawn from authoritative textbook sources:
Extracorporeal Membrane Oxygenation (ECMO)
What Is ECMO?
ECMO (also called extracorporeal life support) is a form of prolonged cardiopulmonary bypass that oxygenates and removes CO2 from the blood outside the body, providing support when the heart and/or lungs fail. Its origins trace back to Gibbon's extracorporeal circuit first used successfully for open-heart surgery in 1953.
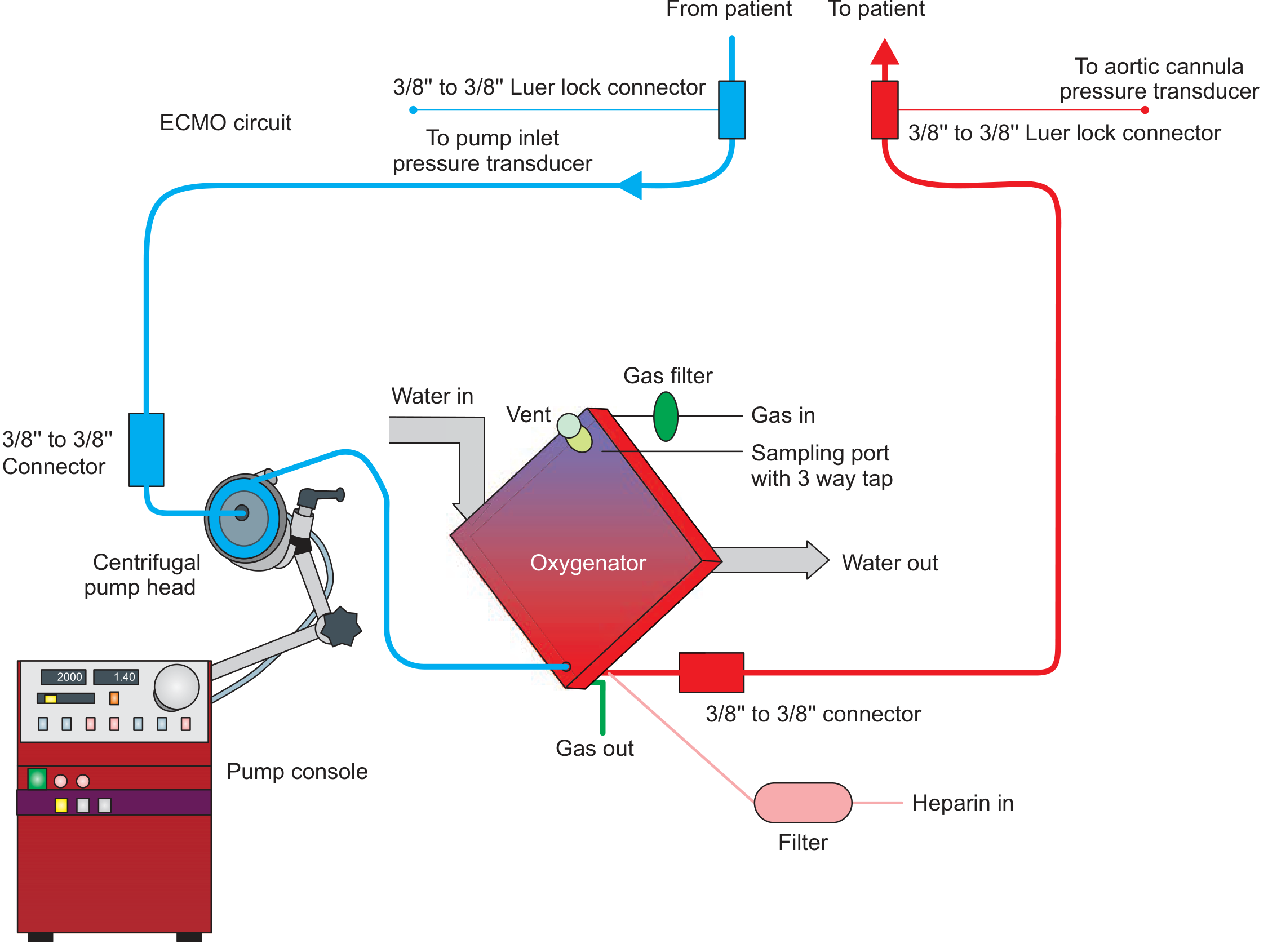
The basic circuit consists of:
- An inflow cannula - drains blood from the patient
- A centrifugal pump - maintains blood flow (magnetically levitated, preload-dependent, afterload-sensitive)
- A membrane oxygenator - gas exchange surface (~2 m² vs. ~143 m² in the human lung)
- An outflow cannula - returns oxygenated blood to the patient
- A heat exchanger - prevents heat loss across the oxygenator
- Continuous heparin infusion to prevent thrombosis
Two Main Types
1. Veno-Venous (VV) ECMO
- Purpose: Lung support only
- Cannulation: Venous drainage and venous return (e.g., femoral vein in, internal jugular vein out via dual-lumen cannula)
- Indication: Severe acute respiratory failure (ARDS, pneumonia, bridging to lung transplant)
- Advantage: Preserves native cardiac output; lower risk of limb ischemia
- Limitation: Does not provide hemodynamic (cardiac) support
2. Veno-Arterial (VA) ECMO
- Purpose: Heart AND lung support
- Cannulation: Venous drainage (femoral/internal jugular), arterial return (femoral artery, or via subclavian graft)
- Indications: Cardiogenic shock, cardiac arrest, refractory hypoxemia, bi-ventricular failure, myocarditis, myocardial stunning
- Key concern: Can cause pulmonary edema and LV fluid overload because it bypasses the LV without unloading it. Often requires additional strategies: inotropes, vasodilators, IABP, or Impella to unload the LV
- Bridges to recovery, VAD placement, or heart transplant
3. Hybrid Configurations
- VAV ECMO and Oxygenated RVAD (Protek Duo): Used when RV failure accompanies respiratory failure (e.g., ARDS with cor pulmonale)
Indications
| Condition | Mode |
|---|---|
| Severe ARDS / acute respiratory failure | VV ECMO |
| Bridge to lung transplant | VV ECMO (awake, ambulatory preferred) |
| Cardiogenic shock | VA ECMO |
| Refractory cardiac arrest (E-CPR) | VA ECMO |
| Myocarditis / myocardial stunning | VA ECMO |
| Biventricular failure + hypoxemia | VA or VAV ECMO |
| RV failure + ARDS | Oxygenated RVAD / VAV ECMO |
Circuit Physiology & Key Parameters
- To achieve adequate O2 delivery (~260 mL O2/min) with post-oxygenator PaO2 >300 mmHg, blood flow of ~4 L/min must be maintained
- CO2 removal is efficient even at low flow rates (<1 L/min with high sweep gas)
- Transmembrane pressure drop should not exceed 30 mmHg (inlet ~250 mmHg, outlet ~220 mmHg)
- Tubing length/surface area matters: activates the inflammatory cascade, consumes clotting factors, and alters pharmacokinetics of antibiotics, opioids, and sedatives
Anticoagulation
Anticoagulation is required continuously to prevent circuit thrombosis:
| Agent | Notes |
|---|---|
| Unfractionated heparin (UFH) | Most common; easy reversal, familiar monitoring (PTT/ACT); risks: heparin resistance, HIT |
| Bivalirudin | Direct thrombin inhibitor; lower HIT risk; renally cleared; t½ ~25 min; no FDA-approved reversal |
| Argatroban | Direct thrombin inhibitor; hepatically cleared; t½ ~45-50 min |
A single-center retrospective study found bivalirudin significantly reduced major bleeding events (11.7% vs. 40.7% with heparin) and decreased circuit thrombosis.
Complications
Hemorrhagic
- Epistaxis, GI bleeding (most common)
- Rare: intracranial hemorrhage, pulmonary hemorrhage
- Mechanism: thrombocytopenia, platelet destruction, clotting factor consumption, anticoagulation
Thrombotic
- Circuit thrombosis (clot in oxygenator or tubing)
- Arterial embolism (especially with VA ECMO)
Hemodynamic (VA ECMO specific)
- LV distension and pulmonary edema (LV cannot eject against the increased afterload from arterial return)
- North-South syndrome (mixing of deoxygenated native LV output with oxygenated ECMO return)
Circuit/Technical
- Pneumothorax and arterial injury during cannulation
- Hemopericardium from guidewire cardiac injury
- Air embolism (especially with awake VV ECMO cannulation)
- Hemolysis (increases exponentially if a second extracorporeal circuit, e.g., CRRT, is added)
- Oxygenator failure (monitor by pressure drop and post-membrane gas values)
Systemic
- Inflammatory cascade activation (cytokine storm)
- Altered drug pharmacokinetics (sequesters antibiotics, sedatives, opioids in tubing)
- Acute kidney injury requiring CRRT (associated with OR 6.5 for in-hospital mortality)
Monitoring & Imaging
- TEE (Transesophageal echocardiography): Before and during cannulation to assess RV/LV function, detect PFO/ASD/VSD, rule out pericardial effusion, guide cannula tip position
- Fluoroscopy: Guides stiff wire and cannula placement
- Ultrasound: Linear surface ultrasound for percutaneous vascular access
- Pre/post-membrane pressure sensors + flow monitoring: Continuous circuit surveillance; transmembrane pressure >30 mmHg signals oxygenator failure
Bridge Strategies
| Goal | Notes |
|---|---|
| Bridge to recovery | Days to weeks; heart/lungs recover; device removed |
| Bridge to VAD | Transition to durable LVAD or BiVAD when no cardiac recovery |
| Bridge to transplant | VV ECMO as bridge to lung transplant (5% of lung transplants as of 2017, rising); awake ambulatory preferred to avoid ventilator-induced injury |
Lung transplant outcomes with VV ECMO bridge: 88% survival to discharge were alive at 1 year; 83% alive at 5 years (Tipograf et al., n=70 successfully transplanted).
Limitations
- VA ECMO does not compensate for severely impaired LV function and may worsen pulmonary congestion
- Not a permanent solution; prone to infection and complications with prolonged use
- Highly institution-dependent: deployment, monitoring, and troubleshooting require dedicated, experienced teams
- Large prime volume causes acute hemodilution at initiation
- Allosensitization risk if blood-primed in pre-transplant patients
Recent Evidence
- ECMO for interstitial lung disease (2024 meta-analysis) - Systematic review in ASAIO J examining outcomes of ECMO in ILD patients [PMID: 38810214]
- Mechanical circulatory support in cardiogenic shock (Lancet 2024) - Individual patient data meta-analysis of temporary MCS (including ECMO) in infarct-related cardiogenic shock at 6-month follow-up [PMID: 39236726]
Sources: Fishman's Pulmonary Diseases and Disorders (Chapter 149, pp. 2641-2660); Fischer's Mastery of Surgery 8th ed. (pp. 345-346)
This is a shared conversation. Sign in to Orris to start your own chat.