50y oldmgle complains of dragging sensation in abdomen. Physical examination revealed pallor and massive spleenomegaly. There is no lymphadenopathy, Total leucocyte count is 1, 60, 000 cellmm' and platelet comnt is 2 Lakis/mm'.LML a) Whatis the pröbable diagmosis? b) Describe cytogenetiç change in this case? c) Enumerate peripheral blood smear findings?
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Finding Sources
I now have comprehensive, authoritative information to give a complete answer. Here is the full structured response:
Clinical Case Analysis
50-year-old male | Dragging abdominal sensation | Pallor | Massive splenomegaly | No lymphadenopathy | TLC = 1,60,000 cells/mm³ | Platelets = 2 lakhs/mm³
a) Probable Diagnosis: Chronic Myeloid Leukemia (CML)
The clinical triad of massive splenomegaly + marked leukocytosis (1,60,000 cells/mm³) + absence of lymphadenopathy in a middle-aged male is the hallmark presentation of CML. As Robbins & Kumar directly states:
"Sometimes the first symptom is a dragging sensation in the abdomen caused by splenomegaly or the acute onset of left upper quadrant pain due to splenic infarction."
Key supportive features in this case:
- Age: CML peak incidence is in the 5th-6th decade of life
- Massive splenomegaly due to extensive extramedullary haematopoiesis
- TLC of 1,60,000 cells/mm³ - leukocytosis often exceeding 1,00,000 cells/µL is characteristic
- Pallor - reflects mild-to-moderate anaemia from marrow infiltration
- No lymphadenopathy - distinguishes CML from lymphoid malignancies (CLL, lymphoma)
- Platelets 2 lakhs/mm³ - platelets are often normal or elevated in CML chronic phase
This is CML in chronic phase (blasts < 10%).
b) Cytogenetic Change: The Philadelphia (Ph) Chromosome
Primary Cytogenetic Abnormality
t(9;22)(q34;q11) - The Philadelphia Chromosome
In >90% of CML cases, a reciprocal translocation between chromosomes 9 and 22 produces the Philadelphia chromosome:
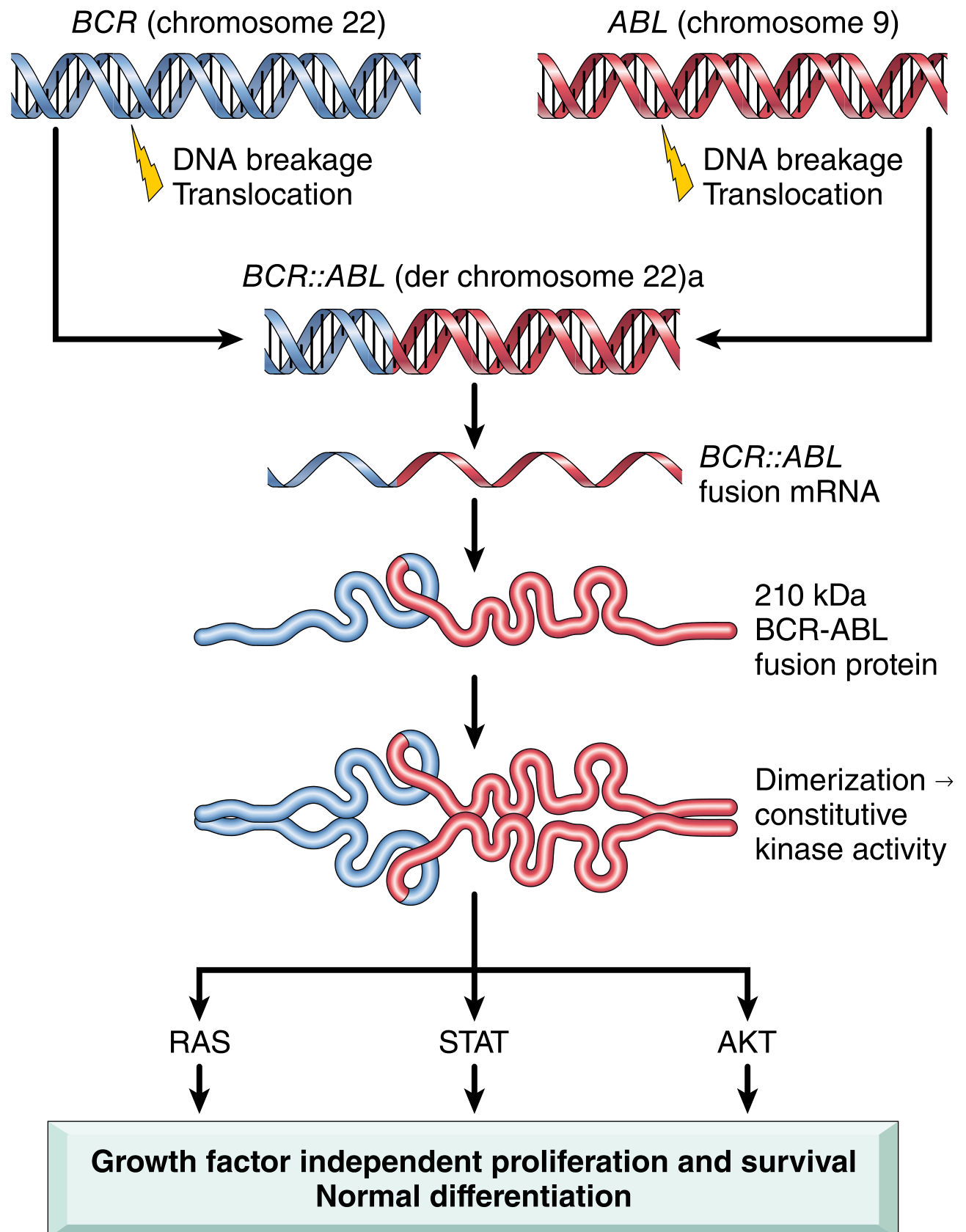
Fig: Pathogenesis of CML - BCR::ABL fusion gene formation and downstream signaling (Robbins & Kumar, Pathologic Basis of Disease)
| Feature | Detail |
|---|---|
| Translocation | t(9;22)(q34;q11) |
| Result on Chr 22 | Shortened chromosome 22 = Philadelphia (Ph) chromosome |
| Result on Chr 9 | Elongated chromosome 9 (der 9) |
| Fusion gene | BCR::ABL chimeric gene on der(22) |
| Fusion protein | 210 kDa BCR-ABL constitutively active tyrosine kinase |
| Downstream pathways | RAS, STAT, AKT - drive growth factor-independent proliferation |
| Differentiation | Preserved (unlike AML) - hence mature cells in peripheral blood |
| Frequency | Present in 100% of CML cases (cytogenetically or molecularly) |
Mechanism: The BCR moiety contains a dimerization domain that causes self-association of the fusion protein, leading to constitutive activation of ABL tyrosine kinase without the need for growth factor stimulation. This drives unregulated proliferation of a pluripotent haematopoietic stem cell.
Note: In the ~10% of cases where the Ph chromosome is not visible on karyotyping ("Ph-negative CML"), the BCR::ABL fusion gene is still detectable by FISH or PCR - there is no truly BCR-ABL-negative CML.
Additional Cytogenetic Changes in Disease Progression
As CML transforms to accelerated/blast phase, additional clonal abnormalities may appear:
- Trisomy 8
- Isochromosome 17q
- Duplication of the Ph chromosome
c) Peripheral Blood Smear Findings
| Finding | Detail |
|---|---|
| Leukocytosis | Marked, often >1,00,000 cells/µL; predominantly granulocytic |
| Neutrophilia | Mature neutrophils and band forms - the dominant cell type |
| Myelocytes | Prominent - the hallmark "myelocyte bulge" in the differential |
| Metamyelocytes | Present in significant numbers |
| Promyelocytes | Present in small numbers |
| Blasts | Usually <10% in chronic phase |
| Eosinophilia | Absolute eosinophilia - a characteristic feature |
| Basophilia | Absolute basophilia - very characteristic of CML; rising basophils signal accelerated phase |
| Anaemia | Normocytic normochromic anaemia |
| Thrombocytosis | Platelets often elevated (sometimes markedly); thrombocytopenia is uncommon in chronic phase |
| Nucleated RBCs | May be seen due to extramedullary haematopoiesis |
| Low LAP score | Leukocyte Alkaline Phosphatase (LAP) score is characteristically low/absent in CML - distinguishes it from leukemoid reaction |
"Myeloid Spectrum" Pattern
The PBS in CML shows a full spectrum of myeloid maturation - from blasts to mature neutrophils - as if the entire bone marrow has "spilled" into the blood. This is unlike a leukemoid reaction (which shows only mature forms and toxic changes) or AML (which shows a maturation arrest with predominantly blasts).
Source: Robbins, Cotran & Kumar - Pathologic Basis of Disease; Goldman-Cecil Medicine; Robbins & Kumar - Basic Pathology
This is a shared conversation. Sign in to Orris to start your own chat.