Discuss premalignant lesions of the gastrointestinal tract
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
I now have comprehensive material from the textbooks. Let me compile the full response.
Premalignant Lesions of the Gastrointestinal Tract
Premalignant (or precancerous) lesions of the GI tract are conditions that carry a statistically elevated risk of progression to malignancy. They span the full length of the alimentary canal and include metaplastic, dysplastic, and neoplastic entities. Understanding them is central to cancer surveillance and prevention.
1. Esophagus
Barrett Esophagus
Barrett esophagus is the most important premalignant condition of the esophagus and the dominant risk factor for esophageal adenocarcinoma.
Definition and epidemiology: Barrett esophagus is a complication of chronic gastro-esophageal reflux disease (GERD) characterized by intestinal metaplasia of the esophageal squamous mucosa. It is estimated to occur in up to 10% of those with symptomatic GERD and approximately 2% of the general population. It is most common in males of European descent aged 40-60 years. The incidence is rising. - Robbins, Cotran & Kumar Pathologic Basis of Disease
Pathogenesis: Prolonged acid exposure triggers a metaplastic transformation of stratified squamous epithelium to columnar (intestinal-type) mucosa. Genomic sequencing reveals driver mutations also found in esophageal adenocarcinoma, and these mutations are more numerous when dysplasia is present. Risk of progression is linked to prolonged symptoms, longer segment length, older age, and European ethnicity.
Morphology:
- Gross: Tongues of red, velvety mucosa extending upward from the gastroesophageal junction (GEJ), alternating with residual pale squamous mucosa.
- Classified as long-segment (≥3 cm) or short-segment (<3 cm); long-segment disease carries higher malignant risk.
- Microscopy: Goblet cells (with mucus vacuoles staining pale blue, giving a wine-goblet shape to the cytoplasm) are diagnostic. Non-goblet columnar cells (gastric-type foveolar cells) are also present.
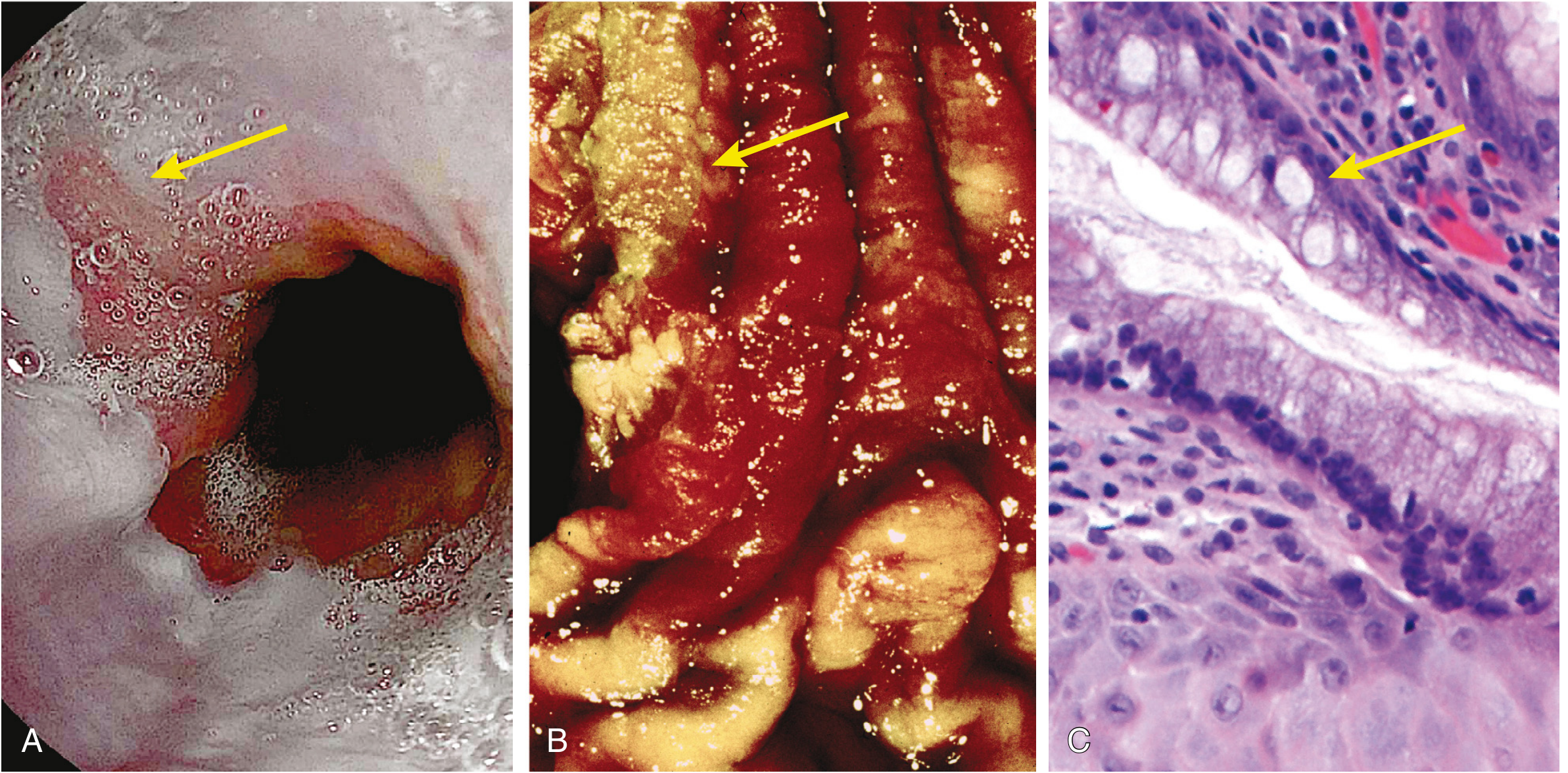
Fig. 17.9 Barrett esophagus. (A) Endoscopic view showing the irregular Z-line; a tongue of salmon-colored columnar mucosa extends upward (arrow). (B) Gross specimen with residual pale squamous mucosa (arrow) within reddish metaplastic mucosa. (C) Histology showing intestinal-type Barrett metaplasia with goblet cells (arrow). - Robbins, Cotran & Kumar Pathologic Basis of Disease
Dysplasia in Barrett esophagus: Dysplasia is the recognized preinvasive precursor step and is graded as:
- Low-grade dysplasia (LGD): Nuclear hyperchromasia, elongation, and stratification; cells fail to mature at the mucosal surface.
- High-grade dysplasia (HGD): More severe cytologic and architectural changes - atypical mitoses, irregularly clumped chromatin, increased nuclear-to-cytoplasmic ratio, glandular budding, and crowding. HGD can progress to intramucosal carcinoma when dysplastic cells invade the lamina propria.
Management:
- Diagnosis requires endoscopy + biopsy with a standardized protocol; chromoendoscopy/narrow-band imaging increase yield.
- LGD: conservative surveillance or radiofrequency ablation (RFA)/endoscopic mucosal resection (EMR).
- HGD or intramucosal carcinoma: RFA, EMR, or surgical esophagectomy (endoscopic mucosectomy is an increasingly viable option for superficial lesions). - Robbins, Cotran & Kumar Pathologic Basis of Disease
Esophageal Squamous Dysplasia
While Barrett esophagus is the precursor for adenocarcinoma, esophageal squamous dysplasia precedes squamous cell carcinoma (SCC). SCC is more common globally, particularly in parts of Asia, Africa, and South America. Risk factors include tobacco, alcohol, achalasia, caustic injury, and nutritional deficiencies. Squamous dysplasia identified on surveillance biopsy represents the preinvasive stage of SCC. - Harrison's Principles of Internal Medicine 22E
2. Stomach
Chronic Atrophic Gastritis and Intestinal Metaplasia
The Correa cascade describes the sequential progression from normal mucosa to adenocarcinoma:
Normal gastric mucosa → Chronic gastritis → Atrophic gastritis → Intestinal metaplasia → Dysplasia → Carcinoma
This sequence is now well established. Chronic atrophic gastritis is by far the most common precursor of gastric cancer, particularly the intestinal subtype.
Intestinal metaplasia (IM): Gastric carcinoma frequently arises in areas of IM, and cancer risk is proportional to the extent of metaplastic change. IM is recognized by the presence of goblet cells in the gastric mucosa and is strongly associated with development of gastric adenocarcinoma. The accompanying achlorhydria of mucosal atrophy permits bacterial overgrowth, leading to production of carcinogenic nitrosamines. - Schwartz's Principles of Surgery 11th Ed.
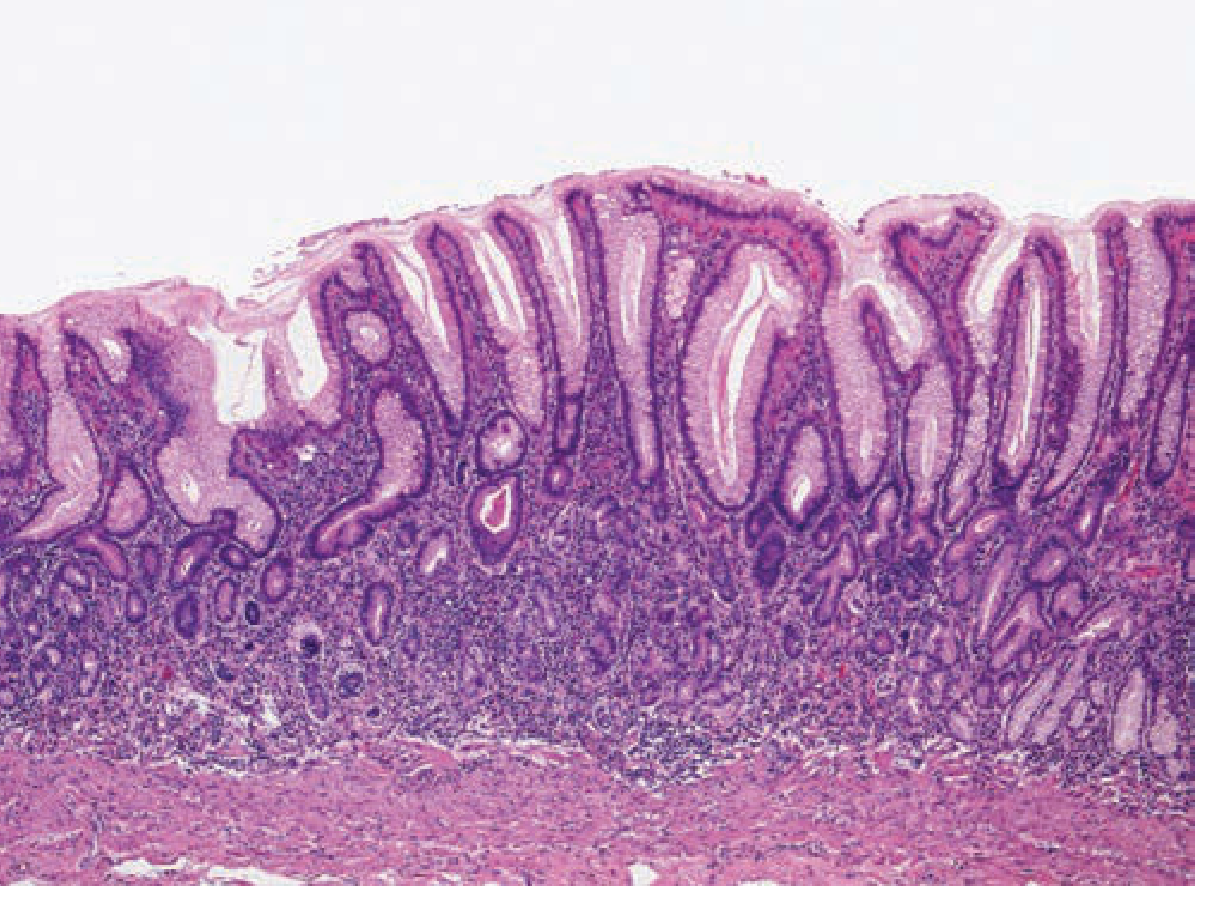
Chronic atrophic gastritis - note the loss of glandular architecture and the dense inflammatory infiltrate. - Schwartz's Principles of Surgery 11e
Types of intestinal metaplasia:
- Complete (Type I): Glands lined with goblet cells and intestinal absorptive cells - histologically indistinguishable from small bowel.
- Incomplete (Types II/III): Contains columnar mucous cells with sulfomucins (especially Type III); considered higher risk for cancer development.
H. pylori is the primary driver of atrophic gastritis and metaplasia. There is evidence that H. pylori eradication may cause IM to regress, though whether this reduces cancer risk is not fully established. Autoimmune metaplastic atrophic gastritis (involving parietal cell destruction) carries the greatest risk of adenocarcinoma. - Robbins & Kumar Basic Pathology
Gastric Dysplasia
Gastric dysplasia is considered the universal immediate precursor to gastric adenocarcinoma. The morphologic hallmarks are:
- Variations in epithelial cell size, shape, and orientation
- Coarse chromatin texture, hyperchromasia, and nuclear enlargement
- Increased proliferative activity (mitotic figures)
- Importantly: dysplastic cells fail to mature as they reach the mucosal surface (a key distinction from reactive/regenerative changes, in which surface maturation is preserved)
Grading and management:
- Mild (low-grade) dysplasia: Endoscopic surveillance with H. pylori eradication
- Severe (high-grade) dysplasia: Gastric resection if widespread/multifocal; EMR if localized - Schwartz's Principles of Surgery
Gastric Polyps
| Polyp Type | Malignant Potential | Notes |
|---|---|---|
| Hyperplastic polyp | Low (but increases with size >1.5-2 cm) | Most common gastric polyp (up to 75%); regresses with H. pylori eradication; large lesions may harbor dysplasia/carcinoma in situ |
| Gastric adenoma | High (premalignant) | Dysplastic by definition; FAP patients have ~50% prevalence and 10x increased gastric adenocarcinoma risk |
| Fundic gland polyp (sporadic) | Very low | Common with PPI use; almost never malignant in sporadic form |
| Fundic gland polyp (FAP-associated) | Moderate | May show dysplasia; rare malignant transformation |
| Inflammatory/hamartomatous | Negligible | Little to no malignant potential |
- Schwartz's Principles of Surgery 11e; Robbins & Kumar Basic Pathology
Gastric Remnant Cancer
Gastric cancer can develop in the gastric remnant following subtotal gastrectomy, usually more than 10 years post-operatively. Tumors arise in an area of chronic gastritis, metaplasia, and dysplasia near the anastomosis. Billroth II gastroenterostomy carries the highest risk due to obligatory bile/pancreatic secretion reflux. Stage-for-stage prognosis is similar to other proximal gastric cancers. - Schwartz's Principles of Surgery
Hereditary Diffuse Gastric Cancer (HDGC) / CDH1 Mutations
Mutations in the CDH1 (E-cadherin) gene cause HDGC, an autosomal dominant disorder with a lifetime gastric cancer risk of 70% (men) and 56% (women). Median age of diagnosis is 38 years. Prophylactic total gastrectomy is recommended for mutation carriers; multifocal intramucosal carcinoma is frequently found even without a pre-operative cancer diagnosis. Mutation-carrying women also face elevated lobular breast cancer risk. - Schwartz's Principles of Surgery
Ménétrier's Disease
The mucous cell hyperplasia of Ménétrier's disease is generally considered to carry a 5-10% risk of adenocarcinoma.
3. Colon and Rectum
Colorectal Adenomas (Adenomatous Polyps)
Colorectal adenomas are the most clinically important premalignant GI lesions. They are precursors to the vast majority of colorectal adenocarcinomas. Present in nearly 50% of adults in the Western world over 50 years of age (rising frequency in Asia in parallel with westernized diets).
Morphology:
- Range from 0.3 to 10 cm; can be pedunculated (on a stalk) or sessile
- Velvety surface texture due to abnormal epithelial growth
- Microscopic hallmark: Epithelial dysplasia - nuclear hyperchromasia, elongation, stratification, failure of surface maturation
Architectural subtypes:
| Type | Architecture | Size tendency | Morphology |
|---|---|---|---|
| Tubular adenoma | Small, rounded/tubular glands | Usually small, pedunculated | Smooth surface, rounded glands |
| Villous adenoma | Slender, finger-like villi | Often large, sessile | Resembles small-intestinal villi |
| Tubulovillous adenoma | Mixed tubular + villous elements | Intermediate | Mixture of both |
Note: While foci of invasion are more frequent in villous adenomas, cancer risk is primarily driven by size, not architecture alone.
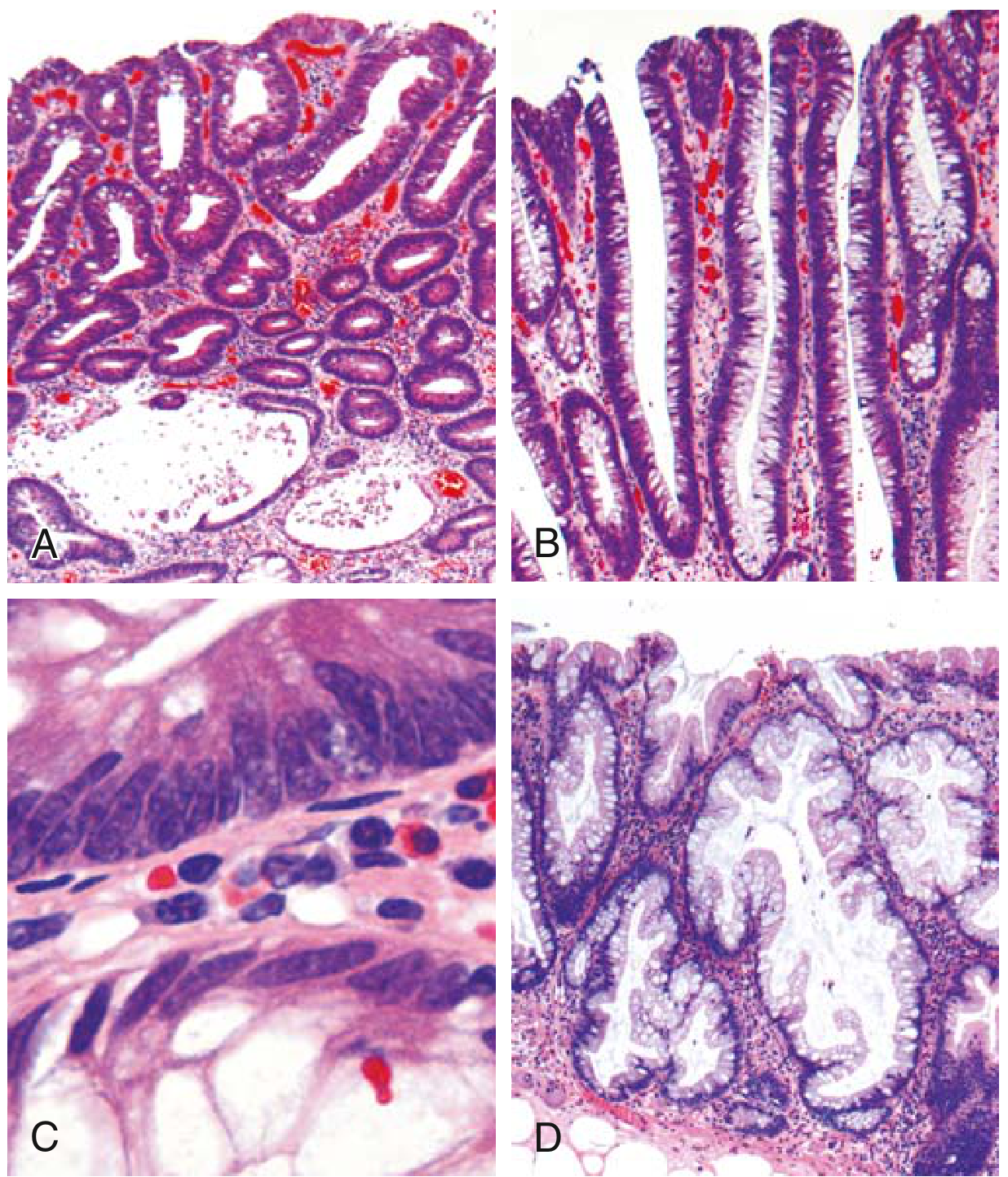
Fig. 13.34 Histologic appearance of colonic adenomas. (A) Tubular adenoma. (B) Villous adenoma. (C) Dysplastic epithelium (top) vs. normal (bottom). (D) Sessile serrated adenoma - distinguished from hyperplastic polyp by full-crypt serration and crypt base involvement. - Robbins & Kumar Basic Pathology
Risk of malignancy:
- Adenomas <1 cm: extremely rare to contain cancer
- Adenomas >4 cm: nearly 40% harbor foci of invasive cancer
- High-grade dysplasia is a secondary (less important) risk factor
- Current US recommendation: colonoscopy screening beginning at 45 years of age - Robbins & Kumar Basic Pathology
Sessile Serrated Adenoma (SSA)
SSAs are a distinct and increasingly recognized entity. Their histologic features overlap with hyperplastic polyps, and they typically lack overt cytologic dysplasia. However, they carry malignant potential similar to conventional adenomas (via the BRAF/CpG island methylator phenotype - CIMP pathway to microsatellite-unstable cancers). The key distinguishing feature from hyperplastic polyps is serrated architecture throughout the full length of the glands including the crypt base, with crypt dilation and lateral (horizontal) growth. - Robbins & Kumar Basic Pathology
Familial Adenomatous Polyposis (FAP)
FAP is an autosomal dominant condition caused by germline mutation of the APC tumor-suppressor gene, resulting in hundreds to thousands of colorectal adenomas appearing by the teenage years. Without prophylactic colectomy, 100% of patients develop colorectal adenocarcinoma, often before age 30.
Variants:
- Gardner syndrome: FAP + osteomas (mandible, skull, long bones), epidermal cysts, desmoid tumors, dental abnormalities
- Turcot syndrome: FAP + CNS tumors (medulloblastoma in APC mutation carriers; glioblastoma in mismatch repair mutation carriers)
Management: Prophylactic colectomy; post-colectomy patients remain at risk for duodenal/periampullary adenomas and desmoids. - Robbins & Kumar Basic Pathology
Lynch Syndrome (Hereditary Non-Polyposis Colorectal Cancer - HNPCC)
Lynch syndrome is caused by germline mutations in DNA mismatch repair (MMR) genes (MLH1, MSH2, MSH6, PMS2), leading to microsatellite instability. It accounts for approximately 2-4% of all colorectal cancers. Associated cancers include colorectal (right-sided predominance), endometrial, gastric, ovarian, small bowel, and urinary tract cancers. Individuals with Lynch syndrome also carry an elevated ~10% risk of gastric cancer, predominantly intestinal subtype. - Schwartz's Principles of Surgery
Inflammatory Bowel Disease-Associated Dysplasia (Colitis-Associated Cancer)
Patients with long-standing ulcerative colitis (UC) are at significantly elevated risk of colorectal cancer. Cancer is most commonly associated with dysplastic changes in the mucosa, often at multiple sites. Risk correlates with:
- Duration of disease (risk increases markedly after 8-10 years)
- Extent of colitis (pancolitis > left-sided > proctitis)
- Presence and grade of dysplasia
Surveillance: Current guidelines recommend colonoscopy with chromoendoscopy or narrow-band imaging with targeted biopsies beginning 8 years after onset of disease, repeated every 1-2 years. If dysplasia is found without a discrete polypoid lesion with well-defined borders, colectomy is recommended. The risk in Crohn colitis is equivalent to UC of similar extent; surveillance colonoscopy is also recommended. - Goldman-Cecil Medicine; Robbins & Kumar
4. Small Intestine
Small intestinal premalignant conditions are less common:
- Celiac disease: Longstanding untreated celiac disease increases the risk of enteropathy-associated T-cell lymphoma (EATL) and small bowel adenocarcinoma. Dietary compliance may reduce this risk.
- Peutz-Jeghers syndrome: An autosomal dominant condition with hamartomatous polyps throughout the GI tract (especially small bowel) caused by STK11/LKB1 mutations. Despite being hamartomas, these polyps carry a risk of GI and extra-GI malignancies (breast, pancreas, ovary, cervix).
- Crohn's disease: Chronic small bowel inflammation can give rise to small bowel adenocarcinoma, particularly in strictured segments.
Summary Table
| Site | Premalignant Lesion | Associated Cancer | Key Risk Factors |
|---|---|---|---|
| Esophagus | Barrett esophagus (intestinal metaplasia/dysplasia) | Adenocarcinoma | GERD, male sex, obesity, European ethnicity |
| Esophagus | Squamous dysplasia | Squamous cell carcinoma | Tobacco, alcohol, achalasia, caustic injury |
| Stomach | Chronic atrophic gastritis + intestinal metaplasia | Intestinal-type adenocarcinoma | H. pylori, autoimmune gastritis, diet |
| Stomach | Gastric dysplasia (low- and high-grade) | Adenocarcinoma | Chronic gastritis, H. pylori |
| Stomach | Gastric adenoma | Adenocarcinoma | H. pylori, FAP |
| Stomach | Large hyperplastic polyp (>1.5-2 cm) | Adenocarcinoma | H. pylori-associated gastritis |
| Stomach | Ménétrier's disease | Adenocarcinoma (5-10% risk) | Unknown |
| Stomach | Gastric remnant (post-gastrectomy) | Adenocarcinoma | Bile reflux, chronic gastritis, Billroth II |
| Colon/Rectum | Adenomatous polyps (tubular, villous, tubulovillous) | Adenocarcinoma | Age, diet, FAP, Lynch syndrome |
| Colon/Rectum | Sessile serrated adenoma | Adenocarcinoma (BRAF/CIMP pathway) | BRAF mutation |
| Colon/Rectum | FAP (APC gene mutation) | Adenocarcinoma (100% if untreated) | Germline APC mutation |
| Colon/Rectum | Lynch syndrome (MMR gene mutations) | Adenocarcinoma + extracolonic cancers | Germline MLH1/MSH2/MSH6/PMS2 mutation |
| Colon/Rectum | IBD-associated dysplasia (UC, Crohn colitis) | Adenocarcinoma | Disease duration, extent, activity |
| Small bowel | Celiac disease (untreated) | EATL, adenocarcinoma | Gluten exposure, non-compliance |
| Small bowel | Peutz-Jeghers polyps | GI + extraintestinal cancers | STK11/LKB1 mutation |
Key conceptual principle: Across all GI sites, the pathway from premalignant change to invasive cancer involves progressive accumulation of genetic alterations - typically driven by chronic inflammation, carcinogenic exposure, or inherited defects in DNA repair or tumor suppressor pathways. The clinical value of recognizing these lesions lies in the opportunity for endoscopic surveillance, early detection, and curative intervention before invasive cancer develops.
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease; Robbins & Kumar Basic Pathology; Schwartz's Principles of Surgery 11e; Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.