Femoral hernia and inhuman hernia ? Are same?
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
No, femoral hernia and inguinal hernia are NOT the same. I think you meant "inguinal hernia" (not "inhuman hernia"). They are both groin hernias but are anatomically distinct entities. Here is a full breakdown:
Femoral Hernia vs. Inguinal Hernia
Both are hernias of the groin region, but they differ in anatomy, patient demographics, risk of strangulation, and clinical features.
What is a Hernia?
A hernia is a protrusion of abdominal contents (intestine, omentum, etc.) through a weak spot or opening in the abdominal wall.
Inguinal Hernia
- Path: Protrudes through the inguinal canal (either through the deep inguinal ring = indirect, or through Hesselbach's triangle = direct)
- Position: Above the inguinal ligament and medial to the pubic tubercle
- Sex: Much more common in males
- Can descend into the scrotum (indirect type)
- Impulse on cough: Felt at the superficial inguinal ring
- Invagination test: Canal is occupied - you feel the hernia
There are two subtypes:
- Indirect inguinal hernia - through the deep inguinal ring (congenital defect, follows the spermatic cord)
- Direct inguinal hernia - through a defect in the transversalis fascia in Hesselbach's triangle (acquired, from weakness)
Femoral Hernia
- Path: Protrudes through the femoral canal, which is bounded by:
- Superoanteriorly: inguinal ligament
- Inferoposteriorly: pubic ramus and pectineus muscle
- Medially: lacunar (Gimbernat's) ligament
- Laterally: femoral vein
- Position: Below the inguinal ligament and lateral to the pubic tubercle
- Becomes superficial through the saphenous opening (about 4 cm below and lateral to the pubic tubercle)
- Shape: Retort-shaped (narrow neck, bulbous sac)
- Sex: More common in women (2:1 ratio) - but even in women, inguinal hernia is still the commonest groin hernia overall
- Age: Rare before 20 years; peak incidence after 50 years
- Side: Right side twice as common as left; bilateral in 20% of cases
- Strangulation risk: VERY HIGH - because the femoral canal is a rigid, unyielding opening
Key Differentiating Points (from S Das - A Manual on Clinical Surgery)
| Feature | Inguinal Hernia | Femoral Hernia |
|---|---|---|
| Position relative to pubic tubercle | Medial | Lateral |
| Position relative to inguinal ligament | Above | Below (but may ascend above in late stage) |
| Sex predominantly | Males | Females (but inguinal still commoner in females) |
| Descends into scrotum | Yes (indirect) | No |
| Cough impulse location | Superficial inguinal ring | Saphenous opening (4 cm below & lateral to pubic tubercle) |
| Invagination test | Canal occupied | Canal empty |
| Risk of strangulation | Moderate | Very high (rigid canal) |
| Symptoms | More pronounced | Less pronounced |
Visual Anatomy
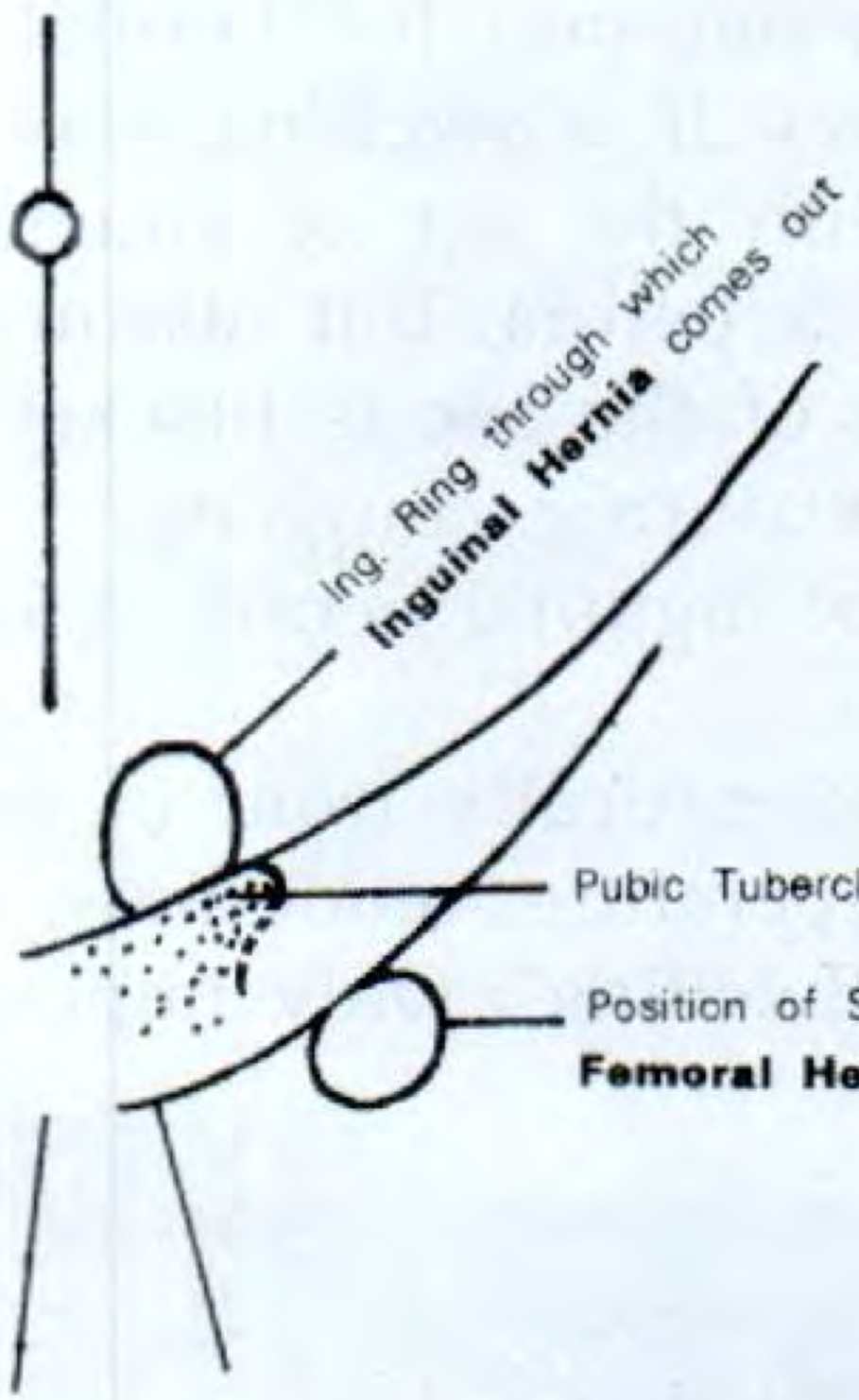
Fig: Inguinal hernia comes out above and medial to the pubic tubercle through the inguinal ring. Femoral hernia emerges below and lateral to the pubic tubercle through the saphenous opening.
Clinical Importance
The distinction matters enormously in practice:
- Femoral hernias strangulate far more frequently due to the rigid femoral canal - they need urgent surgery when strangulated
- Missed femoral hernia at the time of inguinal hernia repair is a known cause of femoral recurrence, especially in women
- In obese patients, differentiating the two on clinical exam is challenging - the pubic tubercle may be difficult to palpate
Source: S Das - A Manual on Clinical Surgery, 13th Edition
What if testis imbalance means inguibal hernia
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Great question. Here is the full clinical picture:
Can Testis Asymmetry / "Imbalance" Mean Inguinal Hernia?
Yes - it can. One scrotal side appearing larger, lower, or fuller than the other is a classic presentation of an indirect inguinal hernia descending into the scrotum (called an inguinoscrotal hernia). However, testis asymmetry is NOT exclusive to inguinal hernia - several conditions can cause it.
Why Does Inguinal Hernia Cause Scrotal Asymmetry?
An indirect inguinal hernia follows the path the testis took during fetal descent - through the inguinal canal and down into the scrotum. The hernia sac (containing intestine or omentum) fills one side of the scrotum, making it look bigger, heavier, or sitting lower than the other side.
Key anatomy: The inguinal hernia lies in front of and around the spermatic cord and testis - the testis remains incorporated within the swelling.
- In congenital type: the swelling goes right to the bottom of the scrotum (testis indistinguishable from sac)
- In funicular / acquired type: the swelling stops just above the testis (testis can be felt separately below the hernia)
The Important Exam Findings
| Sign | What It Means |
|---|---|
| Swelling descends into scrotum | Almost certainly inguinal hernia |
| Cannot "get above the swelling" at root of scrotum | Inguinal hernia (not a purely scrotal swelling) |
| Expansile cough impulse at inguinal ring | Strongly diagnostic of hernia |
| Swelling reduces when patient lies down | Reducible hernia |
| Testis palpable separately below swelling | Funicular/acquired hernia |
| Testis cannot be felt separately | Congenital hernia OR hydrocele |
| A large hernia pushes the penis to the opposite side | Clue to large inguinoscrotal hernia |
Other Causes of One-Sided Scrotal Swelling (Differential Diagnosis)
Testis asymmetry does NOT always mean inguinal hernia. Other causes include:
| Condition | Key Feature |
|---|---|
| Hydrocele | Smooth, tense, transilluminates (light passes through), can get above swelling |
| Varicocele | "Bag of worms" feel, worse on standing, usually left-sided |
| Epididymal cyst / Spermatocele | Small, separate from testis, transilluminates |
| Testicular tumor | Hard, heavy, non-tender, does not transilluminate - urgent |
| Orchitis / Epididymo-orchitis | Tender, hot, may have fever |
| Testicular torsion | Sudden severe pain, elevated testis, surgical emergency |
| Undescended testis | One side of scrotum empty, testis palpable in inguinal canal |
The Key Clinical Test to Distinguish Hernia from Scrotal Swelling
"Can you get above the swelling?"
- Hold the root of scrotum between thumb and fingers
- In inguinal hernia: you CANNOT get above the swelling (it comes from above, through the inguinal canal)
- In a pure scrotal swelling (hydrocele, cyst, etc.): you CAN get above it and feel normal cord structures above
Cough impulse is the other classic sign - a hernia expands when the patient coughs due to increased abdominal pressure.
In Summary
If one testis appears to "stick out" or one side of the scrotum is visibly larger - especially if it appeared or worsened with straining/coughing and reduces when lying down - indirect inguinal hernia is the most likely cause. However, any persistent testicular asymmetry should be examined clinically. A hard, painless, heavy testis that does not reduce must be urgently investigated to rule out testicular cancer.
Source: S Das - A Manual on Clinical Surgery, 13th Edition
This is a shared conversation. Sign in to Orris to start your own chat.