Sheehan's syndrome
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Searching Images
Sheehan syndrome pituitary infarction MRI empty sella
Reading File
Reading File
Now I have comprehensive information. Let me compile the answer with the MRI image.
Sheehan Syndrome
Definition & Pathophysiology
Sheehan syndrome is ischemic necrosis of the anterior pituitary gland caused by severe peripartum hemorrhage and/or hypotension during or after delivery. First described in 1937, the mechanism hinges on the fact that the pituitary gland is physiologically enlarged during pregnancy (due to estrogen-driven lactotroph hyperplasia), making it especially vulnerable to ischemia when hypotension or significant blood loss compromises its blood supply.
Key pathophysiologic points:
- There is no strict correlation between the severity of hemorrhage and the occurrence of the syndrome
- A large portion of the pituitary must be destroyed before symptoms become evident
- The result is panhypopituitarism (total) or partial hypopituitarism, depending on the extent of necrosis
— Creasy & Resnik's Maternal-Fetal Medicine
Epidemiology
- Now uncommon in high-resource settings due to improved obstetric care and hemorrhage resuscitation
- Remains a significant problem in developing countries
- Diagnostic delay is common — mean delay of 19.7 years in one large Turkish series of 114 patients
Clinical Features
Classically presents with postpartum failure of lactation (agalactia) and failure to resume menstruation (amenorrhea) — these are often the first and most recognizable features.
Presentation may be:
| Timing | Features |
|---|---|
| Acute (within 6 weeks postpartum) | Hyponatremia (adrenal insufficiency), severe headache, persistent hypotension/tachycardia |
| Chronic (years later) | Nonspecific fatigue, features of deficient hormones below |
Hormonal deficiencies (in rough order of frequency):
- GH deficiency — fatigue, altered body composition
- Gonadotropin (LH/FSH) deficiency — amenorrhea, loss of axillary/pubic hair, sexual dysfunction
- TSH deficiency (secondary hypothyroidism) — low T4 with low/normal TSH
- ACTH deficiency (secondary adrenal insufficiency) — hyponatremia, hypotension, hypoglycemia (most dangerous)
- Prolactin deficiency — failure of lactation (hallmark, and often the first sign)
- ADH deficiency — diabetes insipidus (less common)
Over 50% of patients in large series are fully panhypopituitary; the rest are partially hypopituitary.
Diagnosis
Laboratory findings:
- Low cortisol with low/normal ACTH
- Low free T4 with low/normal TSH (secondary hypothyroidism)
- Low estrogen with low FSH/LH
- Low IGF-1 (growth hormone deficiency)
- Hyponatremia (adrenal insufficiency)
- Hyperkalemia may also occur
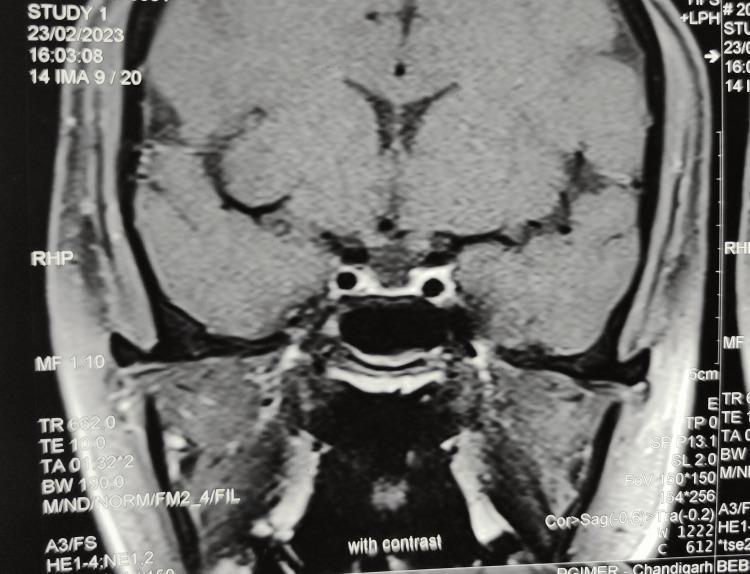
Imaging (MRI):
- Early findings: abnormal lack of pituitary enhancement, enlarged pituitary gland, intrasellar mass
- Later findings: empty sella turcica — the sella fills with CSF as the infarcted pituitary involutes
The classic late MRI appearance of Sheehan syndrome — an empty sella with a thin flattened pituitary rim:
Radiological progression (postpartum day 15 vs. 6 months later):
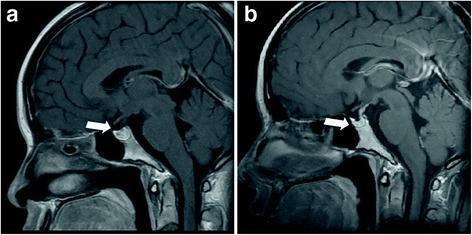
(Image a: normal pituitary at day 15 postpartum. Image b: marked pituitary atrophy at 6 months — characteristic of Sheehan syndrome.)
Management
Hormone replacement therapy targeting deficient axes:
| Deficiency | Replacement |
|---|---|
| Adrenal insufficiency (ACTH) | Hydrocortisone (highest priority — life-threatening if missed) |
| Hypothyroidism (TSH) | Levothyroxine (start after glucocorticoid replacement to avoid precipitating adrenal crisis) |
| Hypogonadism (LH/FSH) | Estrogen/progesterone (pre-menopausal) or testosterone (males) |
| GH deficiency | GH replacement (if symptomatic) |
| Diabetes insipidus | Desmopressin (DDAVP) |
Emergency management: If acute presentation with hypotension/hyponatremia — IV hydrocortisone, fluid resuscitation, urgent endocrinology consultation.
Subsequent pregnancy does not exclude Sheehan syndrome — the condition should be considered in any woman with a history of postpartum hemorrhage and suggestive symptoms.
Differential Diagnosis
- Lymphocytic hypophysitis (especially in peripartum period; may be self-limiting)
- Pituitary apoplexy
- Empty sella syndrome (primary)
- Other causes of hypopituitarism (tumors, irradiation, infiltrative disease)
— Creasy & Resnik's Maternal-Fetal Medicine; Rosen's Emergency Medicine; Goldman-Cecil Medicine
Postpartum hemorrhage
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Searching Images
postpartum hemorrhage uterine atony bimanual compression management
Reading File
Finding Sources
Reading File
Reading File
Excellent. I now have comprehensive information across multiple authoritative sources. Here is the full synthesis:
Postpartum Hemorrhage (PPH)
Definition
Traditional definition:
-
500 mL blood loss after vaginal delivery
-
1000 mL after cesarean delivery
Clinical/practical definition (now preferred):
Any bleeding that results in — or would result if untreated in — signs and symptoms of hemodynamic instability.
Primary PPH: within 24 hours of delivery
Secondary (late) PPH: 24 hours to 6 weeks postpartum
Physiologic Context
Pregnancy increases plasma volume by ~40% and red blood cell volume by ~25% by the end of the third trimester. This hemodilution masks hemorrhage — up to 30% of total blood volume may be lost before blood pressure drops. The first sign may be only a mild tachycardia.
Causes — The "4 T's"
| T | Cause | Frequency |
|---|---|---|
| Tone | Uterine atony | ~70–80% (most common) |
| Tissue | Retained placental fragments, placenta accreta | ~10% |
| Trauma | Lacerations (cervical, vaginal, perineal), uterine rupture, uterine inversion | ~20% |
| Thrombin | Coagulopathy (DIC, hereditary coagulopathy) | <1% |
Risk factors for uterine atony:
- Uterine overdistension: polyhydramnios, multiple gestation, macrosomia
- Multiparity, prolonged or rapid labor
- Oxytocin/tocolytic use
- Intraamniotic infection (chorioamnionitis)
Secondary PPH causes: subinvolution of the placental site, retained tissue, infection, hereditary coagulopathy
Initial Assessment & Resuscitation
- Monitor vitals frequently; recognize that hypotension is a late sign
- IV access — large-bore, ≥2 lines
- Fluid resuscitation — IV lactated Ringer's; prepare for blood transfusion
- Labs — CBC, platelets, fibrinogen, PT/aPTT, fibrin split products, type and crossmatch
- Supplemental oxygen to maximize oxygen delivery
- Ultrasound — helpful to identify retained placenta or intrauterine blood clots
Activate massive transfusion protocol early in severe cases. Transfusion should be guided by clinical assessment, not waiting for lab results. Cryoprecipitate or fibrinogen concentrate should be considered early, as fibrinogen is likely to be depleted.
Uterotonic Pharmacotherapy
First-line: Oxytocin
- 20–40 units in 1 L crystalloid, infused at 200–500 mL/hr, titrated to sustain contractions
- Do not give as IV bolus — causes severe hypotension
- IM route (10 units) if no IV access
Second-line agents (if oxytocin fails):
| Drug | Dose | Key Cautions |
|---|---|---|
| Methylergonovine maleate | 0.2 mg IM q2–4h | Contraindicated in hypertension/preeclampsia — causes vasoconstriction and severe HTN |
| Carboprost (15-methyl PGF₂α) | 0.25 mg IM q15 min, max 2 mg (8 doses) | Caution in asthma/cardiovascular disease; use antiemetics/antidiarrheals concurrently |
| Misoprostol (PGE₁ analogue) | 800–1000 μg PR (or PO) | May cause tachycardia; useful when other agents unavailable |
Tranexamic acid (antifibrinolytic):
- Lysine analogue that inhibits plasmin-mediated fibrin degradation
- WOMAN trial (20,060 patients): reduced death due to bleeding when given within 3 hours of PPH diagnosis (RR 0.69; 95% CI 0.52–0.91)
- ACOG recommends when initial medical therapy fails
- Administer after cord clamping (crosses placenta)
- Not recommended prophylactically — a large RCT (n=4,079) showed no benefit over oxytocin alone
Non-Pharmacologic & Surgical Escalation
Step 1 — Bimanual uterine compression/massage:
One fist in the anterior vaginal fornix, the other compressing the fundus suprapubically. Avoid vigorous downward massage (risk of uterine inversion or broad ligament vessel injury).
Step 2 — Uterine tamponade:
- Bakri balloon (specifically designed for PPH)
- Foley catheter (for low placental implantation site)
- Intrauterine gauze packing (retrospective evidence supports use)
Step 3 — Interventional radiology:
- Selective pelvic vessel embolization (~85–90% success when feasible)
Step 4 — Surgical (laparotomy):
- B-Lynch compression sutures — mechanical hemostasis of atonic uterus
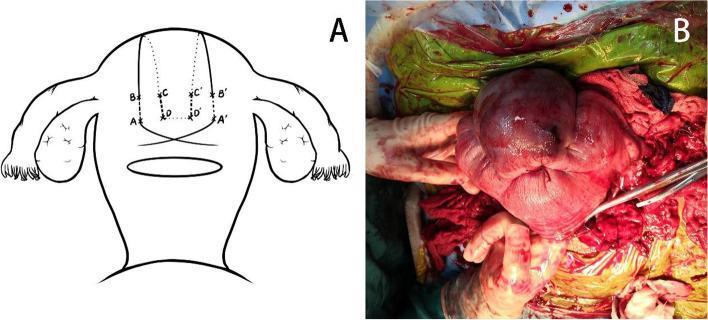
- Uterine/internal iliac artery ligation
- Peripartum hysterectomy — definitive; indicated for refractory atony, placenta accreta, uterine rupture, or failure of all conservative measures
No single invasive option is significantly superior to another; all carry ~85–90% success rates. Hysterectomy follows if these fail.
Cell salvage: Effective in massive obstetric hemorrhage; use leukocyte reduction filter. In Rh-negative patients, give anti-D immunoglobulin and perform Kleihauer-Betke testing.
Special Situations
Uterine inversion:
- Usually from excessive cord traction to deliver placenta
- Diagnosis by vaginal exam or ultrasound
- Treatment: immediate manual replacement of uterus (grasp in palm, push back superiorly); tocolytics (magnesium sulfate 0.25 mg IV) may assist; general anesthesia may be required
Uterine rupture:
- Rare but carries high maternal/fetal mortality
- Primary risk factor: previous cesarean scar
- Requires immediate surgical repair or hysterectomy
Prevention
Active management of the third stage of labor reduces PPH incidence by ~two thirds:
- Early oxytocin administration after delivery of the anterior shoulder
- Early cord clamping
- Controlled cord traction
Adequate IV access should be established prior to delivery in all high-risk patients.
Sources: Creasy & Resnik's Maternal-Fetal Medicine; Tintinalli's Emergency Medicine; Roberts and Hedges' Clinical Procedures in Emergency Medicine; Miller's Anesthesia; Textbook of Family Medicine, 9e; Schwartz's Principles of Surgery
Mastitis
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Searching Images
mastitis breast ultrasound abscess lactational
I now have a comprehensive picture across multiple sources. Here is the full synthesis:
Mastitis
Definition
Mastitis is inflammation or infection of the breast tissue, most commonly occurring during lactation (lactational/puerperal mastitis) but also seen in non-lactating women. It may range from a localized cellulitis to frank abscess formation.
Classification
| Type | Context | Key Features |
|---|---|---|
| Lactational (puerperal) | First weeks–months of breastfeeding | Most common; S. aureus dominant |
| Non-lactational (periductal) | Women in 40s, not breastfeeding | Subareolar; duct rupture/leakage; smoking association |
| Granulomatous (idiopathic) | Parous women, often hyperprolactinemia | Noncaseating granulomas; mimics cancer |
| Tuberculous | Rare; immunocompromised/endemic areas | Sinus tract formation |
Lactational Mastitis
Epidemiology & Pathogenesis
Occurs in approximately 5% of lactating women, most commonly in the first month of breastfeeding. It affects ~1 in 3 breastfeeding women in the US by some estimates, and progresses to abscess in up to 10% of cases.
Entry route: Cracks, fissures, and trauma to the nipple allow skin flora to enter the milk ducts during suckling. Milk stasis (blocked ducts, poor latch, overproduction) predisposes to infection by creating a nutrient-rich environment.
Risk factors: Breast trauma, latch difficulties, milk overproduction, blocked ducts, cracked nipples, poor hygiene
Causative organisms:
- Staphylococcus aureus — 40–88% (dominant; can form abscesses)
- Streptococcus species (viridans, group A/B) — spreading cellulitis pattern
- Escherichia coli, Corynebacterium — less common
- Community-acquired MRSA — increasingly important; consider in cases failing standard therapy
Clinical Features
- Prodrome: malaise, flu-like symptoms, fever ≥39°C, chills
- Local signs: erythematous, hot, tender, swollen wedge-shaped area of the breast (corresponding to one lobe)
- Ipsilateral axillary pain/tenderness
- Discolored milk from the infected breast
- Initially one duct system is involved; if untreated, infection spreads to the entire breast
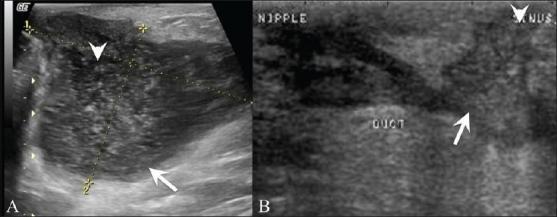
Ultrasound Findings
Mastitis (pre-suppurative):
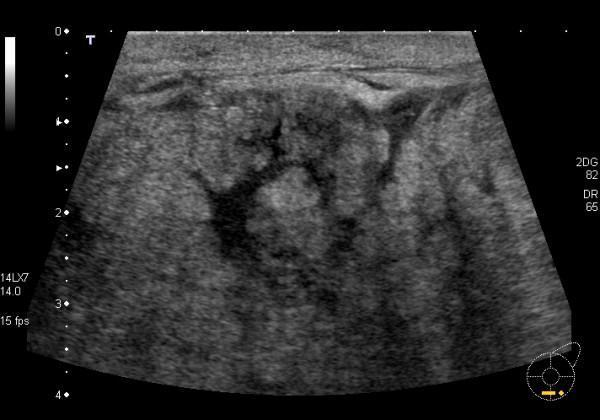
Diffuse heterogeneous parenchymal echogenicity, dilated hypoechoic ducts, skin thickening, and edema — no discrete fluid collection.
Breast abscess:
Hypoechoic, well-defined fluid collection with absent vascular signals; mobile internal echoes may be present. Ultrasound is essential to distinguish mastitis from abscess before deciding management.
Diagnosis
Primarily clinical (history + examination). Routine milk culture is not required.
Cultures are indicated when:
- No response to antibiotics within 48 hours
- Recurrent mastitis
- Hospital-acquired mastitis
- Severe cases or antibiotic allergy
- MRSA suspected (culture midstream milk flow)
Management
1. Continue breastfeeding — do NOT stop.
Continued breast emptying on both breasts is critical. Stopping breastfeeding worsens milk stasis and increases abscess risk.
2. Supportive care:
- Analgesia (paracetamol, NSAIDs) — facilitates milk let-down and expression
- Rest, adequate fluids and nutrition
- Heat before feeding (aids let-down); cold after expression (pain relief)
- Bimanual breast massage (therapeutic massage technique)
3. Antibiotics — recommended by most practitioners for 10–14 days (no controlled trial data on optimal duration):
| Drug | Dose | Notes |
|---|---|---|
| Dicloxacillin (sodium) | 500 mg PO four times daily | First-line; excellent anti-staphylococcal coverage |
| Oxacillin | 500 mg PO four times daily | Alternative first-line |
| Cephalexin | 500 mg PO four times daily | For mild penicillin allergy |
| Clindamycin | 300 mg PO every 8 hours | Serious penicillin allergy; active vs MRSA |
| TMP-SMX DS | Twice daily | Active vs MRSA; less expensive, less diarrhea than clindamycin; contraindicated in infants <2 months old |
Mastitis should improve within 24–48 hours of starting antibiotics. Failure to improve mandates ultrasound to exclude abscess and broadening of coverage.
Most common cause of recurrent mastitis: delayed or inadequate initial treatment.
Breast Abscess
Complicates mastitis in ~3–10% of cases.
Management:
- Ultrasound-guided aspiration — first-line; should be documented to resolution sonographically
- Antibiotics — as above; for drug-resistant organisms, oral cephalosporins or clindamycin
- Surgical incision and drainage — last resort in lactating patients (risk of milk fistula)
- IV vancomycin (1 g q12h) — for septic or hospitalized patients; alternatives: linezolid, quinupristin-dalfopristin (reserve for refractory cases due to cost)
- Continue breastfeeding throughout, unless the antibiotic regimen is contraindicated for the infant
Non-Lactational Mastitis
Presents in women typically in their 40s with acute breast pain, erythema, and swelling — predominantly in the nipple-areolar area. Caused by rupture of dilated subareolar ducts and leakage into periductal tissue.
Treatment:
- Empirical antibiotics: cephalexin 250 mg q6h or dicloxacillin 250 mg q6h for 7–10 days
- If no response → ultrasound to exclude abscess → incision and drainage if found
- MRSA coverage if risk factors present: TMP-SMX, clindamycin, or tetracycline
Subareolar abscess in young smokers:
- Caused by squamous metaplasia of lactiferous ducts (Zuska disease)
-
90% of patients are smokers
- Ductal obstruction by keratin → rupture → intense granulomatous inflammation → recurrent abscess and periareolar fistula
- Simple I&D alone leads to recurrence; definitive treatment is en bloc excision of the involved duct and fistula tract
- Smoking cessation is essential
Granulomatous Mastitis
- Inflammatory phlegmon, often tender, with skin ulceration; may mimic cancer
- Occurs in parous women; associated with hyperprolactinemia
- Diagnosis: core needle biopsy — noncaseating granulomas around breast lobules
- Culture to exclude tuberculosis
- Idiopathic granulomatous mastitis (IGM): associated with Corynebacterium species; treat with targeted antibiotics (doxycycline, clindamycin, azithromycin, or levofloxacin) ± systemic steroids
- In many cases, observation alone suffices — the process often resolves spontaneously
Key Differential Diagnosis
Inflammatory breast carcinoma must always be excluded when breast erythema fails to resolve with antibiotics. Biopsy is mandatory in any case not responding to treatment. In non-lactating women, failure to improve is an indication for urgent breast surgery referral.
Prevention (Lactational Mastitis)
- Avoid alcohol-based nipple cleaning products
- Apply lanolin to nipple and areola after nursing
- Ensure effective latch and adequate breast emptying
- Treat nipple fissures promptly
Sources: Creasy & Resnik's Maternal-Fetal Medicine; Goldman-Cecil Medicine; Tintinalli's Emergency Medicine; Berek & Novak's Gynecology; Current Surgical Therapy, 14e; Robbins, Cotran & Kumar Pathologic Basis of Disease; Mulholland & Greenfield's Surgery
Miscarriage and abortion difference
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive material from multiple authoritative sources. Here is the synthesized answer:
Miscarriage vs. Abortion — Medical Terminology Clarified
The Core Distinction
In everyday language, "miscarriage" and "abortion" are often treated as opposites — one natural, one deliberate. In medical terminology, however, "abortion" is the umbrella term for any pregnancy loss before viability (~20 weeks), and miscarriage is simply the lay term for one specific type.
"Abortion (Latin: aboriri, to miscarry) is a premature stoppage of development and expulsion of a conceptus from the uterus before it is viable." — The Developing Human: Clinically Oriented Embryology
Definitions Side by Side
| Term | Medical Meaning |
|---|---|
| Spontaneous abortion | Pregnancy loss that occurs naturally, without intervention, before 20 weeks gestation — this is what the public calls a "miscarriage" |
| Induced abortion | Deliberate termination of pregnancy by medical or surgical means before 20 weeks |
| "Miscarriage" | Lay/colloquial term — synonymous with spontaneous abortion only |
| "Abortion" (in medicine) | Covers both spontaneous and induced types — the broader clinical category |
The WHO defines spontaneous abortion as loss of pregnancy before 20 weeks or loss of a fetus weighing <500 grams.
Types of Spontaneous Abortion (Miscarriage)
All of the following refer to vaginal bleeding before 20 weeks of gestation:
| Type | Definition |
|---|---|
| Threatened abortion | Vaginal bleeding through a closed cervical os — pregnancy still potentially viable |
| Inevitable abortion | Bleeding + cervical dilatation (and/or membrane rupture) — cannot be prevented |
| Incomplete abortion | Passage of some but not all products of conception; more common between 6–14 weeks |
| Complete abortion | Passage of all products of conception before 20 weeks |
| Missed abortion | Fetal death at <20 weeks with retention of all products of conception — usually asymptomatic |
| Septic abortion | Any stage of abortion complicated by infection |
| Habitual/Recurrent abortion | Three or more consecutive spontaneous abortions (some societies define as two or more) |
Epidemiology of Spontaneous Abortion
- 25–30% of all recognized pregnancies end in spontaneous abortion
- 75–80% occur before 8–12 weeks (first trimester)
- Using sensitive β-hCG assays, an additional 20% of very early pregnancies terminate spontaneously before the woman is even aware of pregnancy — total rate approaches 50–70% of all conceptions
- The most common single cause is chromosomal abnormality (~50% of early losses)
Causes of Spontaneous Abortion
| Category | Examples |
|---|---|
| Fetal/genetic (most common) | Aneuploidy, polyploidy, translocations; present in ~50% of early losses |
| Maternal endocrine | Luteal phase defect, poorly controlled diabetes, thyroid disorders |
| Uterine structural | Submucosal fibroids, polyps, uterine malformations, Asherman syndrome |
| Systemic vascular | Antiphospholipid antibody syndrome, hypertension, coagulopathies |
| Infectious | Toxoplasma, Mycoplasma, Listeria, syphilis, HIV; ascending infections common in second trimester |
| Immunological | Defective fetal-maternal immune tolerance; regulatory T-cell dysfunction |
| Environmental/behavioral | Tobacco (>30% increased risk, dose-dependent), heavy alcohol, caffeine, certain heavy metals |
| Maternal age | Risk rises sharply at age 35, steeply at 40 — due to oocyte non-disjunction |
Induced Abortion — Subcategories
Induced abortion is the deliberate termination of a pregnancy, and may be:
- Therapeutic — to protect maternal health or life
- Elective — at the patient's request
- Medical (pharmacological) — e.g., mifepristone + misoprostol
- Surgical — dilation and curettage (D&C), dilation and evacuation (D&E), vacuum aspiration
Why the Terminology Matters Clinically
- Documentation accuracy: Patients who have had an induced abortion may report it as a "spontaneous abortion" on history — this can distort risk assessments
- Communication: Using "abortion" medically without clarification can cause distress or confusion for patients expecting the term "miscarriage"
- Legal/ethical context: In many jurisdictions, induced abortion carries legal significance distinct from spontaneous abortion
- Recurrence risk counseling: Each spontaneous abortion increases the risk of a subsequent one; history-taking must distinguish between the two
Summary Table
| Feature | Spontaneous Abortion (Miscarriage) | Induced Abortion |
|---|---|---|
| Initiation | Natural — no intervention | Deliberate — medical or surgical |
| Cause | Chromosomal, structural, maternal disease, etc. | Voluntary or therapeutic decision |
| Gestational limit | <20 weeks / <500 g | Varies by jurisdiction; typically <20–24 weeks |
| Management | Expectant, medical (misoprostol), or surgical (D&C) | Medical or surgical procedure |
| Emotional context | Typically experienced as a loss | Variable |
Sources: The Developing Human (Moore & Persaud); Tintinalli's Emergency Medicine; Robbins, Cotran & Kumar Pathologic Basis of Disease; Swanson's Family Medicine Review; Creasy & Resnik's Maternal-Fetal Medicine
Puerperal infections
Finding Sources
Finding Sources
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
Endometriosis
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.