Conjunctivitis
Reading File
Finding Sources
Searching Images
conjunctivitis types bacterial viral allergic clinical appearance
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Conjunctivitis
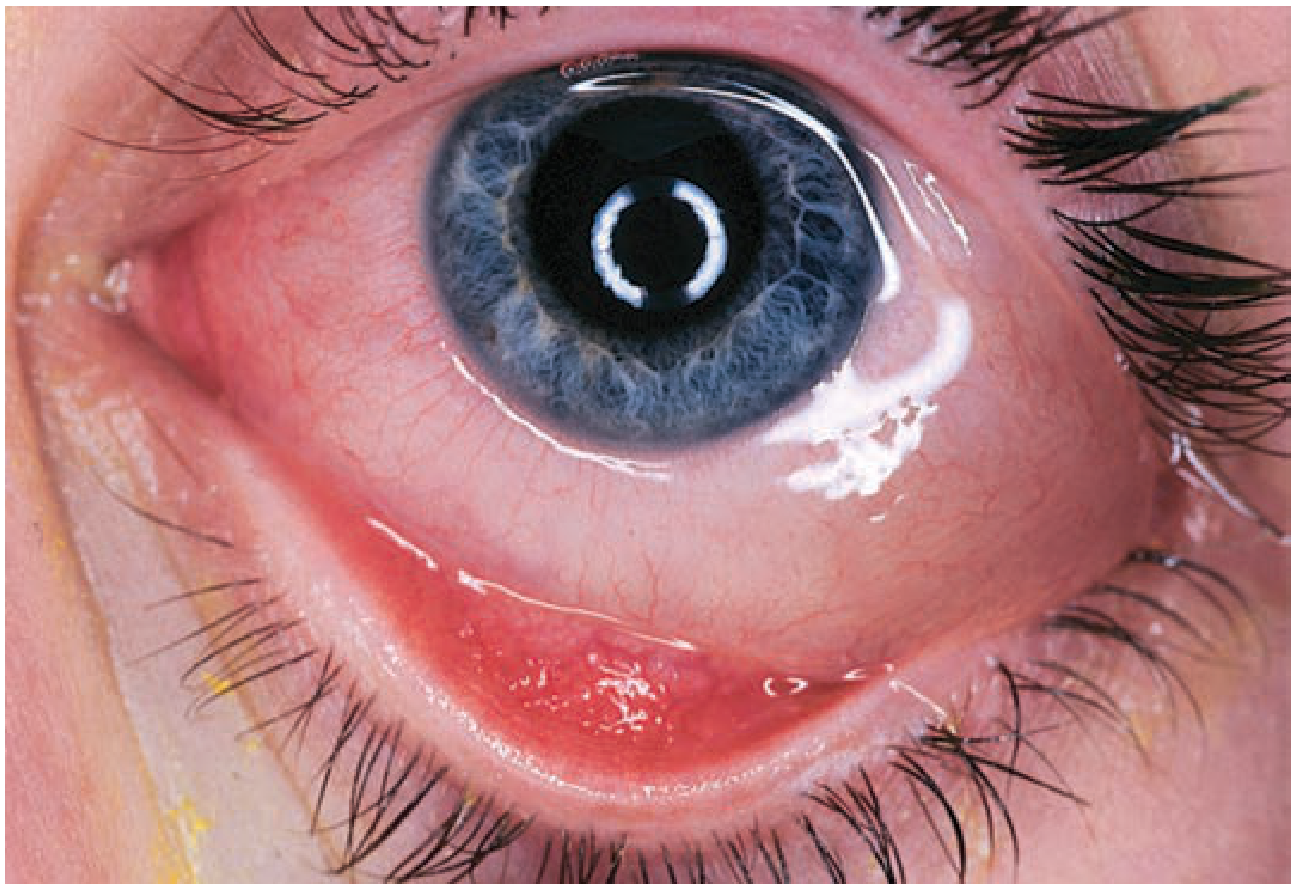
Conjunctivitis is inflammation of the conjunctiva and is one of the most common causes of the red eye. Most cases are viral and self-limited; the clinical challenge is identifying the occasional serious bacterial infection or herpetic corneal involvement that requires aggressive treatment.
Etiology
| Category | Examples |
|---|---|
| Viral | Adenovirus (most common), HSV, enterovirus, influenza |
| Bacterial | Staphylococcus, Streptococcus, H. influenzae, N. gonorrhoeae, Chlamydia |
| Allergic | Environmental allergens, contact lens solutions |
| Toxic/Chemical | Chlorine, smoke, medications |
| Parasitic/Fungal | Rare |
Types & Clinical Features
1. Bacterial Conjunctivitis
Key features:
- Painless, mucopurulent discharge — often causes eyelids to adhere on awakening
- Unilateral or bilateral conjunctival injection
- Clear cornea (no fluorescein staining)
- Chemosis (conjunctival edema) is common
- No preauricular lymphadenopathy (except in gonococcal infection)

Typical pathogens: Staphylococcus spp., Streptococcus spp.
Special forms:
- Gonococcal — can cause ophthalmia neonatorum; associated with preauricular lymphadenopathy
- Chlamydial — also a disease of the newborn
Treatment:
- Most cases are self-limited, but antibiotics shorten the course
- Trimethoprim–polymyxin B — effective first-line; avoids sulfa/neomycin allergy risk
- Contact lens wearers: fluoroquinolone (besifloxacin, gatifloxacin, moxifloxacin, ofloxacin) or tobramycin to cover Pseudomonas
- Always perform fluorescein staining of the cornea, especially in infants, to rule out abrasion, ulcer, or herpetic dendrite
2. Viral Conjunctivitis
Key features:
- URI may precede onset
- Watery discharge (not purulent)
- Mild-to-moderate red eye; no pain unless keratitis is present
- One eye involved first, second eye follows within days
- Preauricular lymphadenopathy present
- Slit lamp: follicles (small, regular, translucent bumps) on inferior palpebral conjunctiva
- Highly contagious

Epidemic Keratoconjunctivitis (EKC):
- More severe adenovirus variant; occurs in epidemics
- Prodrome: cough, high fever, malaise, myalgias
- Corneal punctate staining on fluorescein — represents keratitis
- Duration: 1–3 weeks
Treatment:
- Cool compresses
- Ocular decongestants (e.g., Naphcon-A, 1 drop TID PRN)
- Artificial tears 5–6×/day
- Instruct patient: frequent handwashing, separate towels
- Examiner should wear gloves; disinfect slit lamp and furniture after contact
3. Allergic Conjunctivitis
Key features:
- Intense itching — hallmark symptom
- Watery discharge, redness
- Erythematous, swollen eyelids
- Injected, edematous conjunctiva with papillae (irregular mounds of tissue with central vascular tuft) on inferior fornix
- Chemosis (conjunctival edema) may be prominent
Treatment (stepwise by severity):
- Mild: identify/eliminate allergen; cool compresses QID; artificial tears alone
- Moderate: topical antihistamine/decongestant, mast cell stabilizers, or NSAIDs
- Severe: topical steroids (consult ophthalmologist first — occult herpetic infection must be excluded)
Key Differentiating Features
| Feature | Bacterial | Viral | Allergic |
|---|---|---|---|
| Discharge | Mucopurulent | Watery | Watery |
| Itch | Absent/mild | Absent/mild | Prominent |
| Preauricular nodes | Absent (except GC) | Present | Absent |
| Conjunctival findings | Papillae, chemosis | Follicles | Papillae, chemosis |
| Laterality | Uni/bilateral | Starts unilateral | Usually bilateral |
| Associated symptoms | None | URI, fever | Atopy history |
When to Refer / Red Flags
- Decreased visual acuity
- Corneal involvement (fluorescein staining positive) — suspect herpetic dendrite
- Severe pain
- Gonococcal infection (requires systemic antibiotics)
- No improvement after empiric treatment
If bacterial vs. viral is uncertain after assessment, prescribe topical antibiotics pending ophthalmology follow-up.
— Tintinalli's Emergency Medicine: A Comprehensive Study Guide
Treatment
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Here is a comprehensive treatment summary for conjunctivitis, organized by type:
Treatment of Conjunctivitis
1. Bacterial Conjunctivitis
General Principle
About 60% resolve within 5 days without treatment. Antibiotics shorten the course and reduce transmission but are not always mandatory.
Topical Antibiotics (first-line options)
Use QID for up to 1 week. Ointments provide higher concentration and longer contact time but blur vision — reserve for nighttime use.
| Agent | Notes |
|---|---|
| Trimethoprim–polymyxin B | Preferred first-line; avoids sulfa/neomycin allergy risk |
| Erythromycin / Bacitracin ointment | Broad coverage, well tolerated |
| Tobramycin | Good gram-positive and gram-negative coverage |
| Ciprofloxacin / Ofloxacin | Broad-spectrum fluoroquinolones |
| Gatifloxacin / Moxifloxacin / Besifloxacin | Newer fluoroquinolones; better gram-positive penetration |
| Chloramphenicol | Widely used outside USA; some practitioners avoid due to rare aplastic anaemia risk |
| Fusidic acid | Option in some guidelines |
Contact lens wearers: Use a fluoroquinolone or tobramycin to cover Pseudomonas.
If no improvement in 2–3 days or worsening, refer to ophthalmologist. Culture discharge in severe cases.
Systemic Antibiotics — Required For:
| Organism | Systemic Treatment |
|---|---|
| N. gonorrhoeae | Ceftriaxone (preferred in adults); quinolones or macrolides are alternatives. Seek genitourinary specialist input |
| H. influenzae | Oral amoxicillin–clavulanic acid (25% risk of otitis/systemic spread in children) |
| N. meningitidis | IM benzylpenicillin, ceftriaxone, or cefotaxime — do not delay; up to 30% develop systemic disease |
| Trachoma | Systemic azithromycin (with specialist consultation) |
Gonococcal/meningococcal: Also give topical antibiotic 1–2 hourly initially (quinolone, gentamicin, chloramphenicol, or bacitracin) in addition to systemic therapy.
Supportive
- Irrigation with normal saline to clear excessive discharge in hyperpurulent cases
- Discontinue contact lenses until 48 hours after complete symptom resolution
2. Viral Conjunctivitis
Largely self-limited (1–3 weeks). No specific antivirals except for herpetic involvement.
| Measure | Details |
|---|---|
| Cool compresses | Several times daily for comfort |
| Artificial tears | 5–6 times/day |
| Topical decongestant | e.g., Naphcon-A 1 drop TID PRN for redness |
| Topical antibiotics | Not routinely indicated; prescribe only if bacterial vs. viral distinction is uncertain pending ophthalmology review |
| Topical steroids | Avoid — prolongs viral infection and risks corneal herpetic penetration |
Herpes keratitis (HSV): Topical acyclovir 5% ointment — requires ophthalmology or infectious disease consultation.
Infection Control (critical)
- Frequent handwashing; separate towels
- Examiner wears gloves; disinfect slit lamp and examination surfaces
- No evidence-based medical reason to exclude from school/daycare, though many institutions mandate antibiotics before return
3. Allergic Conjunctivitis
Non-pharmacological
- Identify and eliminate the allergen
- Cool compresses QID
- Keep windows closed during allergy season; wash face/hair after outdoors; avoid touching eyes
Pharmacological (stepwise)
| Severity | Treatment |
|---|---|
| Mild | Artificial tears alone; oral non-sedating antihistamine |
| Moderate | Topical antihistamine–decongestant (naphazoline–pheniramine [Naphcon-A]) — note: rebound vasodilation can occur with prolonged use |
| Moderate–Severe | Topical mast cell stabilizer: cromolyn sodium 4%, pemirolast (QID during allergy season); dual-action antihistamine + mast cell stabilizer: olopatadine (Patanol), ketotifen, azelastine (Optivar) |
| Moderate | Topical NSAIDs: ketorolac (Acular), lodoxamide (Alomide) |
| Severe | Topical corticosteroids — only with ophthalmology consultation (risk of herpetic infection, glaucoma, cataracts, fungal ulcer) |
| Refractory | Allergy testing and immunotherapy (desensitization shots) |
For concomitant allergic rhinoconjunctivitis: topical cromolyn sodium or topical antihistamines (olopatadine, azelastine, ketotifen, epinastine) are effective.
4. Neonatal Conjunctivitis (Ophthalmia Neonatorum)
| Type | Onset | Treatment |
|---|---|---|
| Chemical (silver nitrate prophylaxis) | Day 1 | None — self-resolves |
| Gonococcal | Days 3–5 | IV/IM cefotaxime 50 mg/kg (preferred over ceftriaxone in neonates — avoids bilirubin displacement and kernicterus); admit + ophthalmology consult; irrigate with NS; topical alone is inadequate |
| Chlamydial | End of week 1 – 1 month | Oral erythromycin 50 mg/kg/day ÷ QID × 14 days; treat mother and partners; topical unnecessary |
| HSV | Variable | Full sepsis evaluation; IV acyclovir 20 mg/kg/dose TID |
Key Contraindication
Topical corticosteroids should not be used for conjunctivitis outside ophthalmologist supervision due to risk of:
- Herpetic corneal perforation
- Steroid-induced open-angle glaucoma
- Cataracts
- Fungal corneal ulcer
— Kanski's Clinical Ophthalmology, Tintinalli's Emergency Medicine, Textbook of Family Medicine 9e, Rosen's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.