
PXL_20260505_101642759.jpg
Solve with reason
Reading File
Finding Sources
Reading File
Reading File
Answer: E. Partial Agonism
The correct answer is E — Partial agonism.
The Question
A patient on haloperidol (a typical antipsychotic / full D2 antagonist) develops bradykinesia, tremor, and cogwheel rigidity — classic extrapyramidal side effects (EPS). He is switched to aripiprazole, which causes fewer EPS. Why?
Reasoning
The key lies in aripiprazole's unique receptor pharmacology at the D2 dopamine receptor.
Haloperidol → Full D2 Antagonist
Haloperidol blocks D2 receptors completely (intrinsic activity = 0). In the nigrostriatal pathway, dopamine normally suppresses involuntary movement. Full D2 blockade eliminates this dopaminergic tone → EPS (parkinsonism, tremor, cogwheeling, bradykinesia).
Aripiprazole → Partial D2 Agonist
Aripiprazole has intrinsic activity between 0 and 1 at D2 receptors. It acts as a "dopamine stabilizer":
- Where dopamine is excessive (mesolimbic pathway → psychosis): aripiprazole occupies D2 receptors and transmits less signal than full dopamine → functional antagonism → antipsychotic effect
- Where dopamine is low (nigrostriatal pathway → movement control): aripiprazole still provides some agonist stimulation → preserves nigrostriatal tone → far fewer EPS
"As a partial D2 agonist, aripiprazole offers the putative advantage of stabilizing the dopamine neurotransmitter system by decreasing the amount of signaling when there is excessive ligand... and by increasing the signal when there is reduced activity (by acting as an agonist)." — Kaplan & Sadock's Comprehensive Textbook of Psychiatry
"Overactive dopaminergic pathways tend to be inhibited by aripiprazole, whereas underactive pathways are stimulated. This might explain the ability of aripiprazole to improve symptoms of schizophrenia, with a small risk of causing extrapyramidal adverse effects." — Lippincott Illustrated Reviews: Pharmacology
Why the Other Options Are Wrong
| Option | Why incorrect |
|---|---|
| A. Agonism | Aripiprazole is not a full agonist — full agonism would worsen psychosis |
| B. Antagonism | Simple antagonism (like haloperidol) is what causes EPS — not what reduces it |
| C. Inverse agonism | Inverse agonists produce below-baseline receptor activity, which would worsen movement side effects |
| D. Irreversible antagonism | Irreversible blockade would cause permanent full D2 blockade — worse EPS, not less |
| F. Reversible antagonism | Still full antagonism at D2 → still causes EPS (haloperidol itself is a reversible competitive antagonist) |
Summary
Aripiprazole's partial agonist activity at D2 receptors means it provides just enough nigrostriatal dopaminergic tone to avoid the parkinsonian EPS that full antagonists like haloperidol produce, while still blocking excessive mesolimbic dopamine activity responsible for psychosis. This "dopamine system stabilizer" property is the mechanistic basis for its reduced EPS profile.
Also explain the discussed topic
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Drug-Receptor Interactions: The Full Topic Explained
The question tests your understanding of drug-receptor pharmacodynamics — specifically the spectrum of receptor interactions. Here is a complete explanation.
1. Core Concepts: Affinity vs. Intrinsic Activity
Every drug that acts at a receptor has two independent properties:
| Property | Definition |
|---|---|
| Affinity | How tightly the drug binds to the receptor |
| Intrinsic activity (efficacy) | How much the drug activates the receptor after binding (0 = none, 1 = full) |
Affinity gets you to the receptor. Intrinsic activity determines what happens next.
2. The Agonist Spectrum

A. Full Agonist (Intrinsic activity = 1)
- Binds AND fully activates the receptor
- Produces the same maximum response (Emax) as the endogenous ligand
- Example: Dopamine at D2 receptors; morphine at μ-opioid receptors
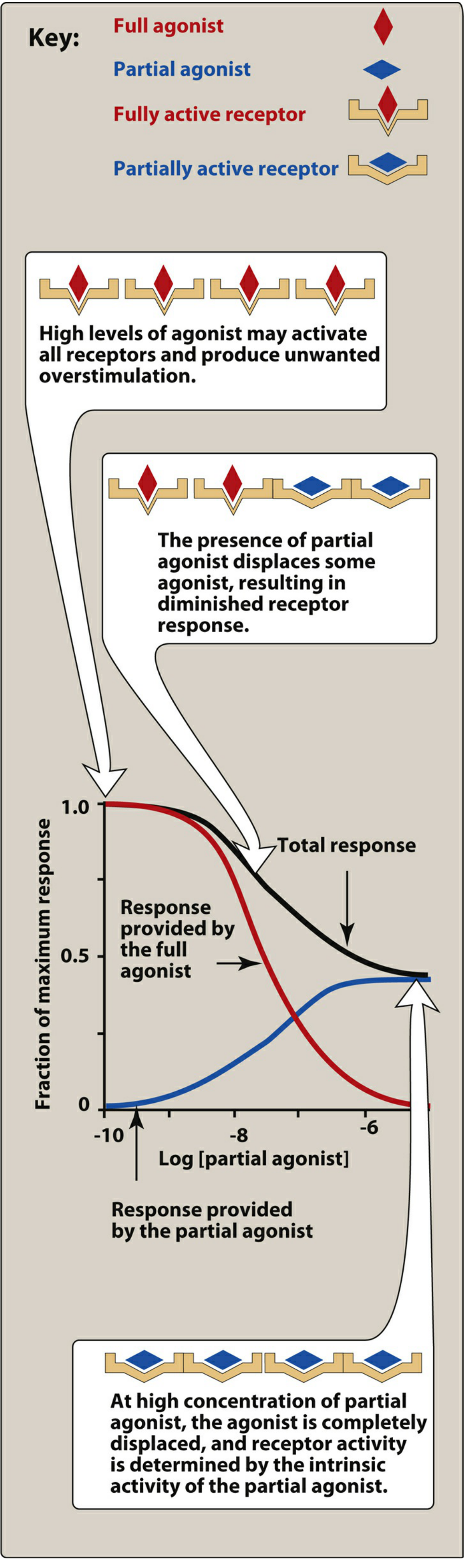
B. Partial Agonist (0 < Intrinsic activity < 1)
- Binds the receptor but produces less than maximal activation, even when all receptors are occupied
- Cannot reach the same Emax as a full agonist, regardless of dose
- Dual character — acts as an agonist OR antagonist depending on context:
"A partial agonist can function both as an agonist or antagonist based on the presence or absence of the endogenous ligand." — Kaplan & Sadock's Comprehensive Textbook of Psychiatry
- In the absence of endogenous ligand → acts as an agonist (provides some signal)
- In the presence of excess endogenous ligand → acts as a functional antagonist (displaces it and delivers less signal)
Example: Aripiprazole at D2 receptors; buprenorphine at μ-opioid receptors
C. Inverse Agonist (Intrinsic activity < 0)
- Some receptors have constitutive (baseline) activity even without any drug
- Inverse agonists bind and suppress receptor activity below baseline — they stabilize the inactive receptor conformation
- Opposite pharmacological effect to agonists
- Example: certain antihistamines at H1 receptors
D. Silent Antagonist (Intrinsic activity = 0)
- Binds with high affinity but produces zero activation
- Does not affect receptor activity alone, but blocks agonists from binding
- Two subtypes:
- Competitive (reversible): Can be overcome by increasing agonist concentration; shifts dose-response curve rightward (↑EC50), Emax preserved. Example: haloperidol, naloxone
- Irreversible: Binds covalently or with very high affinity; cannot be overcome; permanently reduces Emax
3. Partial Agonism in Detail: The Two-Face Mechanism
This is the key insight:
- At low dopamine states → partial agonist provides some stimulation → agonist behavior
- At high dopamine states → partial agonist competes with and displaces dopamine, transmitting less signal → functional antagonist behavior
This context-dependent behavior is what makes partial agonists so clinically valuable as "stabilizers."
4. Receptor Conformation: The Molecular Basis
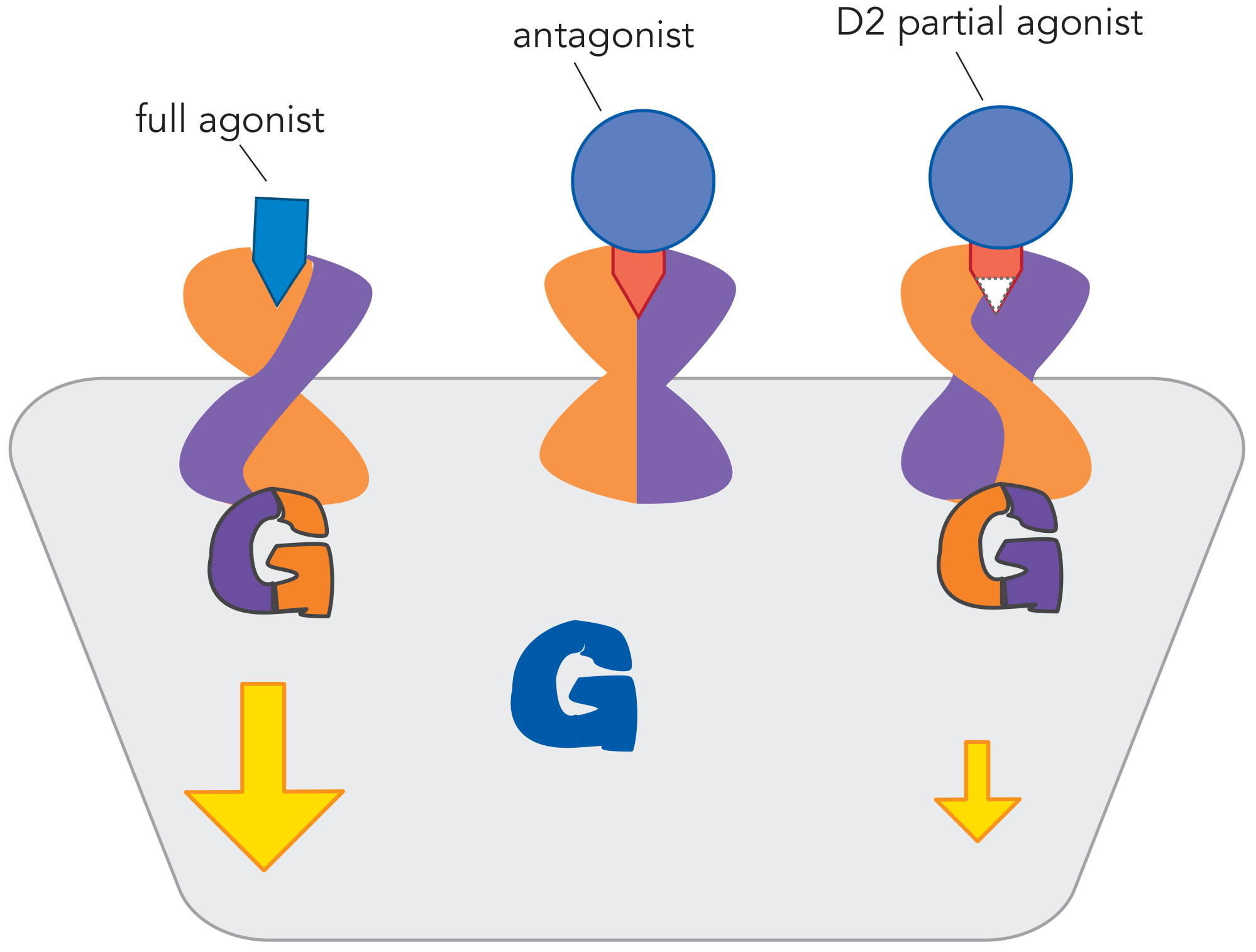
Each drug stabilizes a different receptor conformation:
- Full agonist → fully open conformation → maximum G-protein coupling → maximum intracellular signal
- Antagonist → closed/locked conformation → no G-protein coupling → no signal
- Partial agonist → intermediate conformation → partial G-protein coupling → reduced signal
5. Applied to Schizophrenia: The Four Dopamine Pathways
This is why it all matters clinically:
| Pathway | Dopamine State in Schizophrenia | Effect of Full Antagonist (Haloperidol) | Effect of Partial Agonist (Aripiprazole) |
|---|---|---|---|
| Mesolimbic (reward/psychosis) | ↑↑ Excess | Blocks → treats positive symptoms ✓ | Displaces excess dopamine → functional antagonist → treats positive symptoms ✓ |
| Mesocortical (cognition/negative symptoms) | ↓↓ Deficit | Blocks further → worsens negative/cognitive symptoms ✗ | Provides some agonism → improves negative/cognitive symptoms ✓ |
| Nigrostriatal (movement) | Normal | Full blockade → EPS (tremor, rigidity, bradykinesia) ✗ | Small agonism preserves movement tone → minimal EPS ✓ |
| Tuberoinfundibular (prolactin) | Normal | Full blockade → ↑ prolactin → galactorrhea ✗ | Partial agonism → minimal prolactin elevation ✓ |
"Partial agonists are also proposed to have reduced liability for extrapyramidal symptoms (EPS) and hyperprolactinemia when excessive dopamine receptor blockade occurs in the nigrostriatal and tuberoinfundibular pathways." — Kaplan & Sadock's Comprehensive Textbook of Psychiatry
6. Where Aripiprazole Sits on the Spectrum
A critical nuance from Stahl's Essential Psychopharmacology:
"The D2 partial agonists for the treatment of psychosis are 'almost' antagonists with just a whiff of intrinsic agonist activity."
Aripiprazole sits very close to the antagonist end of the agonist spectrum — just enough agonism to preserve nigrostriatal tone and avoid EPS, but close enough to antagonism to block hyperdopaminergic mesolimbic activity (positive symptoms). This precise positioning is what distinguishes antipsychotic partial agonists from dopamine partial agonists used in Parkinson's disease (which sit near the full-agonist end).
Summary Table
| Drug Type | Intrinsic Activity | In Absence of Ligand | In Excess Ligand | Clinical Use |
|---|---|---|---|---|
| Full agonist | = 1 | Full activation | Full activation | Replace/mimic endogenous ligand |
| Partial agonist | 0 < x < 1 | Partial activation | Functional antagonist | "Stabilizer" — aripiprazole, buprenorphine |
| Silent antagonist | = 0 | No effect | Blocks agonist | Most classic drugs — haloperidol, naloxone |
| Inverse agonist | < 0 | Suppresses baseline | Suppresses further | Reduce constitutive receptor activity |
This is a shared conversation. Sign in to Orris to start your own chat.