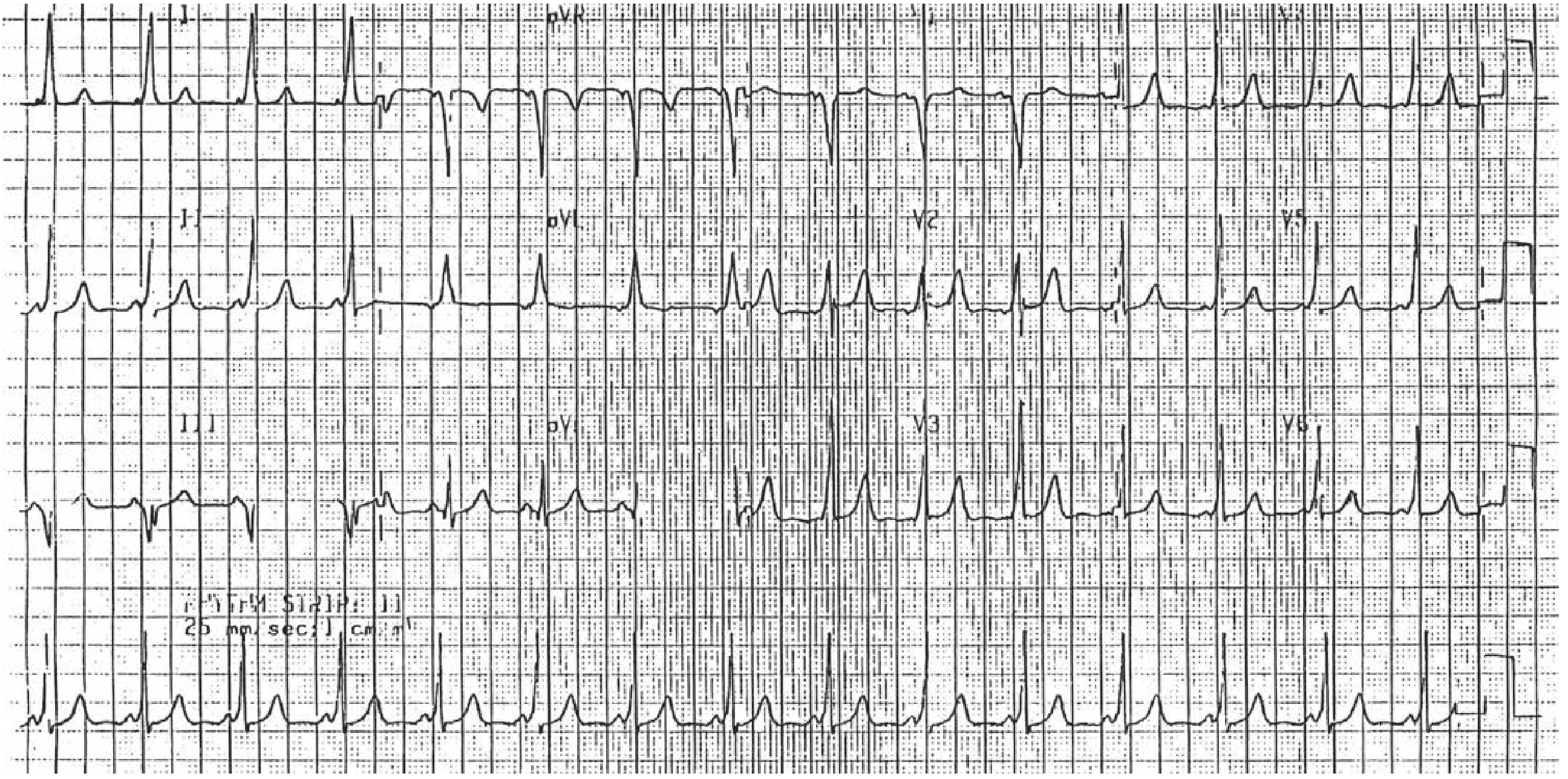
35-year-old female with sinus rhythm, short PR interval. PR interval is 108 milliseconds, QRS duration 82 milliseconds, QT or QTc interval is 472. bar 400 milliseconds. ST junctional depression seen.
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Now I have enough information to provide a thorough ECG interpretation. Let me synthesize the findings.
ECG Interpretation
Patient: 35-year-old female
Rhythm: Sinus rhythm
Key Measurements & Findings
| Parameter | Value | Normal | Interpretation |
|---|---|---|---|
| PR interval | 108 ms | 120–200 ms | SHORT (< 120 ms) |
| QRS duration | 82 ms | < 100 ms | Normal |
| QTc | 472 ms | < 440–450 ms (female) | Borderline prolonged |
| RR interval | 400 ms | — | Heart rate ~150 bpm |
| ST changes | Junctional depression | — | Abnormal |
Primary Diagnosis: Lown-Ganong-Levine (LGL) Syndrome Pattern
The combination of a short PR interval (108 ms) with a normal QRS duration (82 ms) and no delta wave is the hallmark of LGL syndrome, not classic WPW.
- In WPW: short PR + wide QRS + delta wave (slurred QRS upstroke)
- In LGL: short PR + normal QRS + no delta wave
This distinction is critical. In WPW, the bundle of Kent bypasses the AV node and inserts directly into ventricular myocardium, producing pre-excitation (delta wave). In LGL, the aberrant bundle (James fibers) bypasses the AV node but connects into the His-Purkinje system distal to the node — so ventricular conduction proceeds normally, giving a narrow QRS without a delta wave. — Ganong's Review of Medical Physiology, 26th Ed.
"Attacks of paroxysmal supraventricular tachycardia, usually nodal tachycardia, are seen in individuals with short PR intervals and normal QRS complexes (Lown-Ganong-Levine syndrome). In this condition, depolarization presumably passes from the atria to the ventricles via an aberrant bundle that bypasses the AV node but enters the intraventricular conducting system distal to the node." — Ganong's Review of Medical Physiology
Additional ECG Features
1. Borderline Prolonged QTc (472 ms)
- Normal QTc for females is < 460–470 ms; values > 460 ms are considered borderline prolonged in women
- At a rate of ~150 bpm (RR = 400 ms), the Bazett correction may overcorrect — QTc should be interpreted with caution at fast rates
- Warrants monitoring; consider checking electrolytes (K⁺, Mg²⁺, Ca²⁺) and reviewing any QT-prolonging medications
2. ST Junctional Depression
- "Junctional" (J-point) ST depression at a rate of ~150 bpm can be a normal rate-related repolarisation change
- However, in the context of a pre-excitation syndrome or SVT, it may reflect:
- Secondary repolarization changes due to altered ventricular activation
- Demand ischemia if the rate is truly ~150 bpm
- If this ECG was captured during tachycardia, the ST changes are likely rate-related
Clinical Implications
| Risk | Detail |
|---|---|
| SVT susceptibility | LGL pathways predispose to AVRT and PSVT; orthodromic re-entry is most common |
| AF risk | Atrial fibrillation can occur with rapid accessory pathway conduction |
| Drugs to avoid if SVT occurs | Verapamil and digoxin are contraindicated in accessory pathway syndromes — may precipitate lethal dysrhythmias — Tintinalli's Emergency Medicine |
| Definitive treatment | Electrophysiology study + radiofrequency catheter ablation if symptomatic |
| Adenosine | Indicated for PSVT conversion in LGL — Roberts and Hedges' Clinical Procedures in Emergency Medicine |
Summary
This ECG pattern — short PR (108 ms) + normal narrow QRS (82 ms) + no delta wave — in a 35-year-old female in sinus rhythm represents the LGL pre-excitation pattern. The RR of 400 ms suggests the ventricular rate is ~150 bpm (possibly captured during or just after a tachycardic episode). ST junctional depression is likely rate-related. The borderline QTc requires serial monitoring.
Recommended next steps: 12-lead ECG at rest, electrolytes, Holter monitoring, and cardiology/electrophysiology referral for risk stratification and consideration of EP study.
Symptoms patient can experience
Finding Sources
Finding Sources
Reading File
Finding Sources
Here is a comprehensive overview of symptoms this patient with an LGL/accessory pathway pattern may experience:
Symptoms Associated with This ECG Pattern
May Be Completely Asymptomatic
Many patients with short PR interval accessory pathway patterns are discovered incidentally on routine ECG with no symptoms at all. — Tintinalli's Emergency Medicine
Cardiac Symptoms (When Dysrhythmias Occur)
Dysrhythmias occur in approximately 50% of patients with accessory pathway syndromes. When they do, the patient may experience:
1. Palpitations
- The most common presenting complaint
- Described as a racing, fluttering, or pounding sensation in the chest
- Typically sudden onset and sudden offset ("paroxysmal")
- Can last seconds to hours
2. Dizziness / Lightheadedness
- Due to reduced cardiac output during rapid tachycardia
- May precede syncope
3. Syncope (Fainting)
- Loss of consciousness from hemodynamic compromise during sustained rapid tachycardia
- A high-risk symptom — warrants urgent electrophysiology referral
- Family history of syncope or sudden death should be specifically asked about — Pfenninger and Fowler's Procedures for Primary Care
4. Shortness of Breath / Dyspnoea
- Occurs during tachycardic episodes due to elevated heart rate and impaired ventricular filling
5. Chest Pain / Chest Tightness
- Can occur during fast SVT episodes due to demand ischemia, even in a structurally normal heart
6. Fatigue / Weakness
- During or after a prolonged tachycardic episode
Tachyarrhythmias That Drive These Symptoms
| Arrhythmia | Characteristics | Symptoms |
|---|---|---|
| Orthodromic AVRT (most common) | Narrow QRS, rate 150–250 bpm | Palpitations, dyspnoea, presyncope |
| Atrial fibrillation (up to 30% of patients) | Irregular, can be very fast via accessory pathway | Palpitations, dizziness, syncope |
| Antidromic AVRT (less common) | Wide QRS, very rapid | Severe symptoms, hemodynamic instability |
| Ventricular fibrillation (rare but catastrophic) | Via uncontrolled AF down accessory pathway | Sudden cardiac arrest/death |
Symptoms Related to the Borderline Long QTc (472 ms)
The mildly prolonged QTc adds an additional risk layer:
- Palpitations from triggered premature beats
- Dizziness or syncope — if torsades de pointes (polymorphic VT) is triggered
- Risk is amplified by electrolyte disturbances (hypokalemia, hypomagnesemia) or QT-prolonging drugs (antihistamines, antibiotics, antidepressants, antipsychotics)
Red Flag Symptoms Requiring Urgent Referral
| Symptom | Significance |
|---|---|
| Syncope during exertion | High-risk — may indicate fast conduction during AF |
| Syncope without warning | Possible ventricular arrhythmia |
| Family history of sudden cardiac death | Inherited accessory pathway risk |
| Presyncope with palpitations | Suggests haemodynamically significant tachycardia |
Summary
This 35-year-old woman may be entirely asymptomatic, or may experience episodic palpitations, dizziness, dyspnoea, chest tightness, or syncope — all driven by paroxysmal tachycardias mediated through the accessory pathway. The short PR pattern combined with a borderline QTc means she carries risk from two separate mechanisms (re-entrant tachycardia and potential torsades). Cardiology/electrophysiology referral is warranted for risk stratification regardless of current symptom status. — Tintinalli's Emergency Medicine; Pfenninger and Fowler's Procedures for Primary Care
This is a shared conversation. Sign in to Orris to start your own chat.