Classify cholinergic drugs. Explain the pharmacological actions, therapeutic uses, and adverse effects of Atropine.
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the information needed for a comprehensive, well-structured answer. Let me compile it.
Classification of Cholinergic Drugs
Cholinergic drugs act on receptors activated by acetylcholine (ACh). They are broadly divided into cholinergic agonists (which mimic or enhance ACh) and cholinergic antagonists (which block ACh receptors).
A. Cholinergic Agonists
1. Direct-Acting Agonists
These drugs bind directly to and activate muscarinic or nicotinic receptors.
| Drug | Receptor Selectivity | Key Use |
|---|---|---|
| Acetylcholine | M + N (non-selective) | Intraocular use (miosis) |
| Bethanechol | M (selective) | Urinary retention, gastroparesis |
| Carbachol | M + N | Glaucoma, intraocular miosis |
| Methacholine | M (selective) | Bronchial challenge test |
| Pilocarpine | M (selective) | Glaucoma, xerostomia (Sjogren's) |
| Cevimeline | M1, M3 (selective) | Xerostomia in Sjogren's |
| Nicotine | N (selective) | Smoking cessation |
2. Indirect-Acting Agonists (Cholinesterase Inhibitors)
These drugs inhibit acetylcholinesterase (AChE), thereby increasing endogenous ACh availability.
a) Reversible Inhibitors
| Drug | Key Use |
|---|---|
| Edrophonium | Diagnosis of myasthenia gravis |
| Neostigmine | Reversal of NMB, myasthenia gravis |
| Pyridostigmine | Myasthenia gravis (long-acting) |
| Physostigmine | Anticholinergic toxicity (crosses BBB) |
| Donepezil, Rivastigmine, Galantamine | Alzheimer's disease |
b) Irreversible Inhibitors (Organophosphates)
| Drug | Key Use |
|---|---|
| Echothiophate | Glaucoma (ophthalmic) |
| Malathion, Sarin, Parathion | Insecticides / chemical warfare agents |
c) AChE Reactivator
| Drug | Use |
|---|---|
| Pralidoxime (2-PAM) | Antidote in organophosphate poisoning (must be given before "aging") |
B. Cholinergic Antagonists
1. Antimuscarinic Agents (most clinically important)
Block muscarinic (M) receptors. Examples: Atropine, Scopolamine, Glycopyrrolate, Ipratropium, Tiotropium, Oxybutynin, Benztropine, Tropicamide.
2. Ganglionic Blockers
Block nicotinic receptors at autonomic ganglia. Examples: Trimethaphan, Hexamethonium. Clinically obsolete.
3. Neuromuscular Blocking Agents (NMBAs)
Block nicotinic receptors at the neuromuscular junction.
- Depolarizing: Succinylcholine
- Non-depolarizing: Rocuronium, Vecuronium, Atracurium, Pancuronium
Atropine - Detailed Pharmacology
Source: Naturally occurring tertiary amine alkaloid derived from Atropa belladonna (deadly nightshade) and Datura stramonium.
Chemical nature: Racemic mixture of d- and l-hyoscyamine; the l-isomer (l-hyoscyamine) is the pharmacologically active form.
Mechanism of Action
Atropine is a competitive antagonist at muscarinic receptors. It blocks binding of ACh to all five muscarinic receptor subtypes (M1-M5), preventing receptor activation and inhibiting downstream second-messenger effects. It has essentially no effect on nicotinic receptors at normal clinical doses.
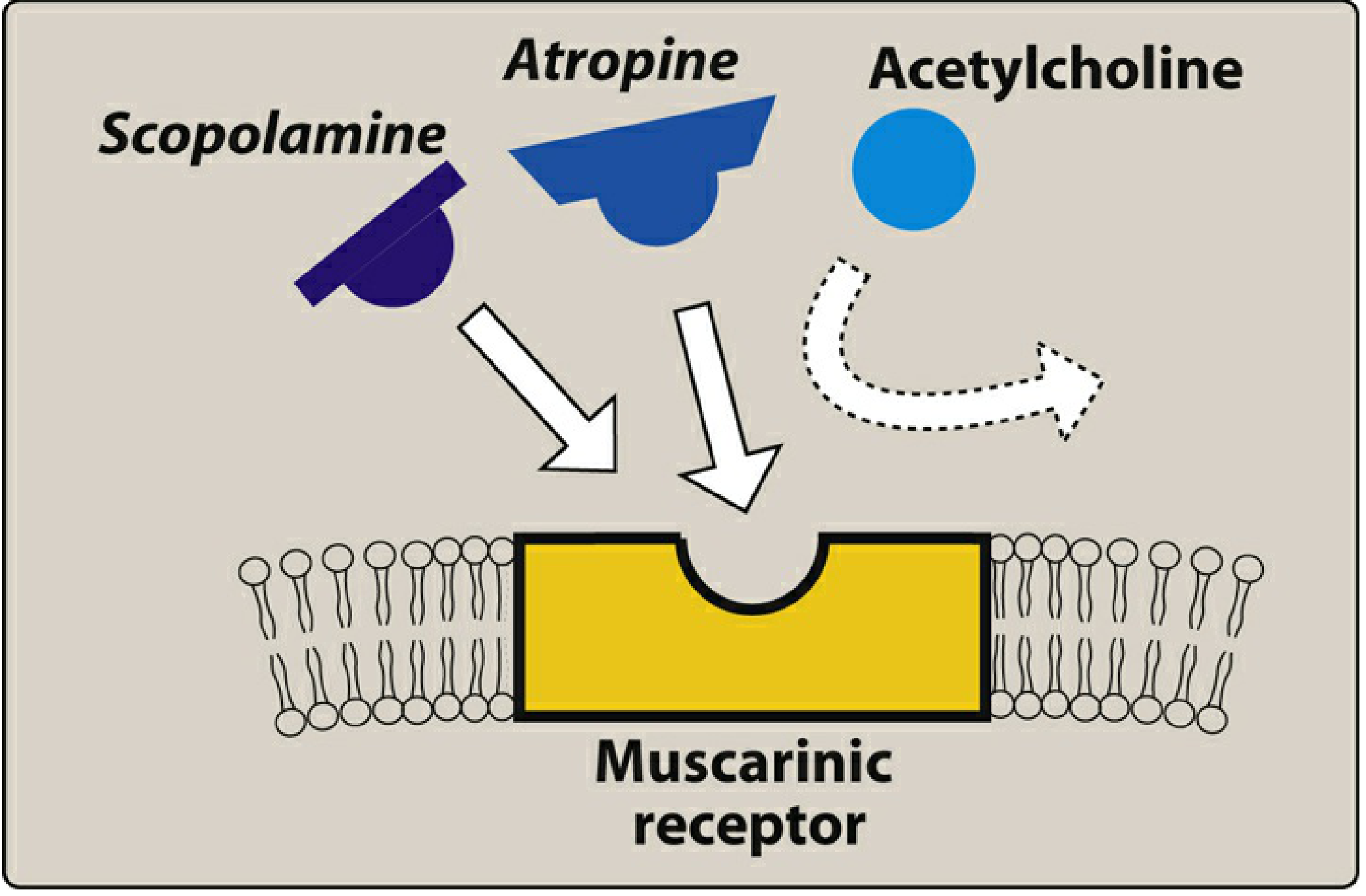
Atropine and scopolamine competing with acetylcholine for the muscarinic receptor - Lippincott Illustrated Reviews: Pharmacology
Receptor subtype distribution:
- M1: CNS, autonomic ganglia, gastric parietal cells
- M2: Cardiac (SA node, AV node) - mediates vagal bradycardia
- M3: Smooth muscle, exocrine glands, eye
Pharmacological Actions
1. Eye (M3 blockade)
- Mydriasis - pupillary dilation (iris sphincter paralysis)
- Cycloplegia - loss of accommodation for near vision (ciliary muscle paralysis)
- Unresponsiveness of pupil to light
- Caution: Can precipitate acute angle-closure glaucoma
2. Cardiovascular (M2 blockade)
- Dose-dependent effects (see diagram below):
- Low doses (0.5 mg): Paradoxical bradycardia due to blockade of M1 receptors on presynaptic inhibitory neurons, allowing more ACh release
- Higher doses (>1 mg): Tachycardia from blockade of M2 receptors at the SA node
- Promotes AV conduction - shortens P-R interval; antagonizes heart block
- Can cause atropine flush (cutaneous vasodilation at high doses)
- Little direct effect on ventricles due to sparse cholinergic innervation
3. Exocrine Glands (M3 blockade)
- Antisialagogue effect - marked reduction in salivation (salivary glands are exquisitely sensitive)
- Reduced lacrimal secretion
- Reduced bronchial secretions
- Reduced gastric secretions (at high doses only)
- Inhibition of sweating (anhidrosis) - can cause hyperthermia ("atropine fever"), especially dangerous in children and the elderly
4. Gastrointestinal (M3 blockade)
- Reduced GI motility and peristalsis
- Antispasmodic effect (one of the most potent antispasmodics)
- Reduces salivation (decreases gastric motility)
- Prolongs gastric emptying time
- Reduces lower esophageal sphincter pressure
- Does NOT significantly reduce HCl production - therefore NOT effective for peptic ulcers
5. Pulmonary (M3 blockade)
- Bronchodilation (relaxes bronchial smooth muscle)
- Reduces respiratory tract secretions (useful during airway procedures)
- Increases anatomic dead space
- More pronounced effect in COPD and asthma
6. Genitourinary (M3 blockade)
- Reduces ureteral and bladder tone (smooth muscle relaxation)
- Can cause urinary retention (especially in men with BPH)
7. CNS (M1, M4, M5 blockade)
- Crosses the blood-brain barrier (being a tertiary amine)
- Low-to-moderate doses: mild stimulation (restlessness, excitability)
- Higher doses: hallucinations, delirium
- Very high doses: coma and respiratory depression
- Less sedation than scopolamine
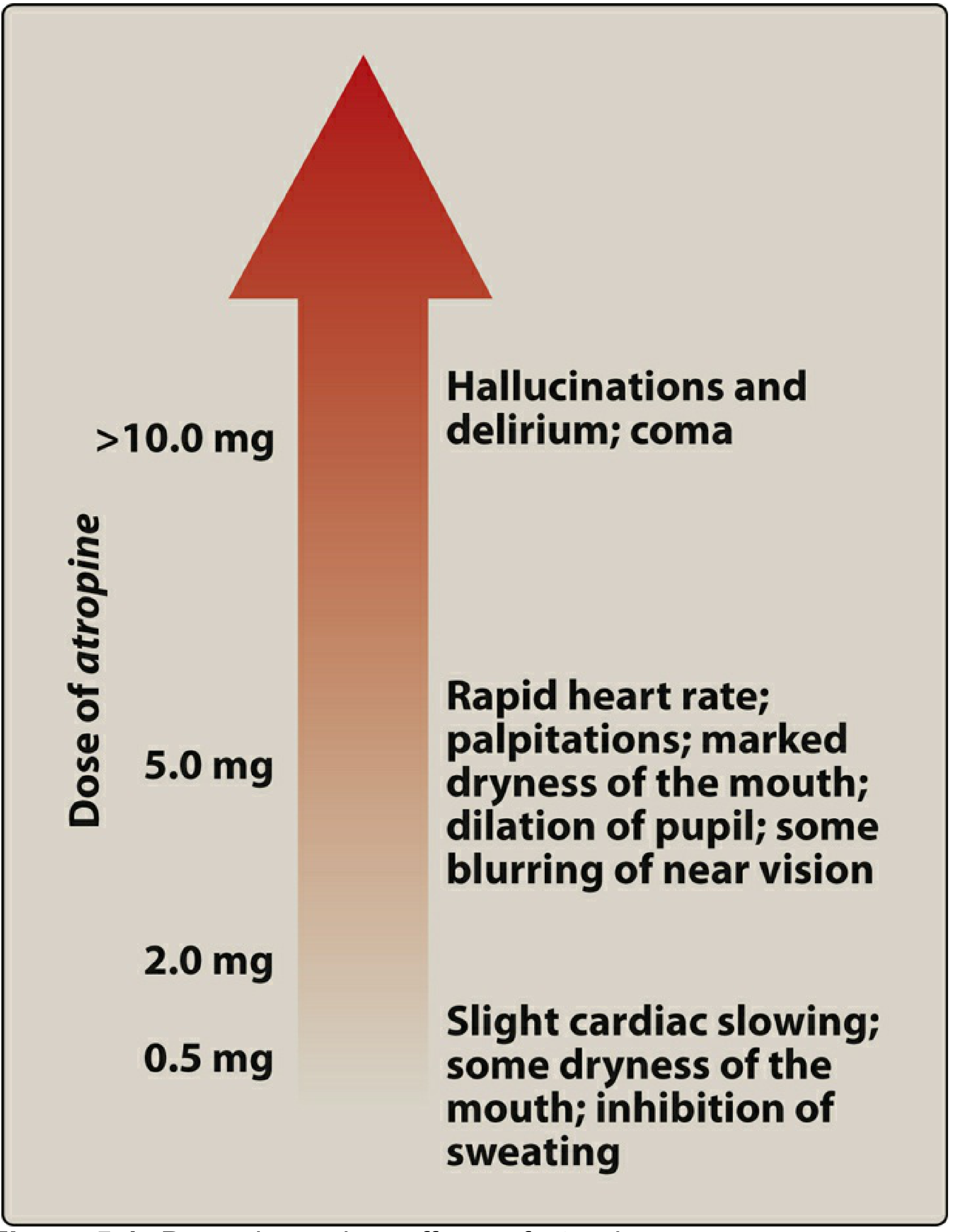
Dose-dependent effects of atropine - Lippincott Illustrated Reviews: Pharmacology
Therapeutic Uses
| System | Indication |
|---|---|
| Ophthalmology | Mydriasis and cycloplegia for fundoscopy and refraction; treatment of anterior uveitis (prevents synechiae) |
| Cardiovascular | Sinus bradycardia; AV block (heart block due to vagal overactivity); bradyarrhythmias during anesthesia |
| Anesthesia (premedication) | Antisialagogue before intubation/airway procedures; prevent vagal bradycardia during laryngoscopy |
| GI | Antispasmodic for intestinal colic, irritable bowel syndrome, biliary/renal colic (combined with analgesics) |
| Organophosphate poisoning | Reverses muscarinic effects (hypersalivation, bronchospasm, bradycardia, lacrimation, miosis) - given in large repeated doses; combined with pralidoxime |
| Mushroom (Amanita muscaria) poisoning | Reverses muscarinic toxidrome |
| ACLS | Historically used for asystole/PEA (no longer first-line per current guidelines) |
| Reversal of NMB | Given with neostigmine to prevent bradycardia from neostigmine-induced muscarinic stimulation |
Adverse Effects
The adverse effects of atropine follow directly from its pharmacological actions and are summarized by the mnemonic "Hot as a hare, blind as a bat, dry as a bone, red as a beet, mad as a hatter":
| Adverse Effect | Mechanism |
|---|---|
| Dry mouth (xerostomia) | Salivary gland M3 blockade |
| Urinary retention | Bladder smooth muscle relaxation; especially in BPH |
| Constipation | Reduced GI motility |
| Tachycardia / palpitations | M2 blockade at SA node |
| Mydriasis / blurred near vision | M3 blockade in eye |
| Acute angle-closure glaucoma | Mydriasis increases aqueous drainage resistance |
| Hyperthermia / flushing (atropine fever) | Inhibition of sweat glands + cutaneous vasodilation |
| CNS effects | Restlessness, confusion, hallucinations, delirium (at high doses) |
| Coma / respiratory depression | Toxic doses (>10 mg) |
| Atropine flush | Cutaneous vasodilation from large doses |
Contraindications
- Angle-closure glaucoma (absolute)
- Benign prostatic hyperplasia (relative - risk of urinary retention)
- Tachyarrhythmias (avoid in paroxysmal tachycardia)
- Paralytic ileus / pyloric stenosis
- Myasthenia gravis
Antidote for Atropine Toxicity
Physostigmine (a cholinesterase inhibitor that crosses the BBB) is the specific antidote for atropine-induced central and peripheral toxicity.
Sources:
- Lippincott Illustrated Reviews: Pharmacology, Ch. 4-5
- Morgan and Mikhail's Clinical Anesthesiology, 7e, Ch. 13
- Goodman & Gilman's The Pharmacological Basis of Therapeutics, Ch. 10
This is a shared conversation. Sign in to Orris to start your own chat.