Diagnostic evaluation of COPD.
Reading File
Finding Sources
Finding Sources
Searching PubMed
"COPD" AND "diagnosis" AND "spirometry"
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
I now have comprehensive content from multiple authoritative sources. Let me compile the full answer.
Diagnostic Evaluation of COPD
1. When to Suspect COPD
Consider COPD in any patient presenting with:
- Chronic cough (with or without sputum production)
- Progressive dyspnea (worsening over time, worse on exertion)
- Chronic sputum production
- History of exposure to risk factors - especially cigarette smoking, biomass fuel smoke, occupational dusts/chemicals
Physical findings such as hyperinflated lungs (barrel chest, low-lying diaphragm, decreased breath sounds, hyperresonant percussion) are highly specific but insensitive - they typically appear only in advanced disease. One clinical sign: a thyroid-to-sternal notch distance < 4 cm in a smoker > 45 years is highly indicative. Clubbing is not a feature of COPD - if present, think bronchiectasis, asbestosis, or lung cancer.
- Fishman's Pulmonary Diseases and Disorders, p. 726
2. Spirometry - The Cornerstone of Diagnosis
Spirometry is the definitive diagnostic test. A post-bronchodilator FEV₁/FVC ratio < 0.70 confirms the presence of airflow obstruction and establishes the diagnosis of COPD.
How it is performed
- The patient exhales forcefully; FEV₁ and FVC are recorded
- 400 µg of albuterol (salbutamol) is administered as the bronchodilator
- Post-bronchodilator values are used (helps distinguish COPD from asthma)
Key spirometric findings in COPD
| Parameter | Finding |
|---|---|
| FEV₁/FVC | < 0.70 (GOLD fixed ratio) or below LLN (ATS/ERS) |
| Flow-volume loop | Concave (scooped) expiratory limb |
| Volume-time curve | Prolonged expiratory time |
| TLC / RV | Elevated (hyperinflation and air trapping) |
Note on fixed ratio vs. LLN: GOLD recommends the fixed ratio of 0.70 for simplicity, but the ATS/ERS recommends the 5th percentile (lower limit of normal). The fixed ratio can overdiagnose COPD in the elderly because FEV₁/FVC normally decreases with age even in healthy non-smokers.
- Murray & Nadel's Textbook of Respiratory Medicine, p. 1471
Flow-Volume Loop in COPD
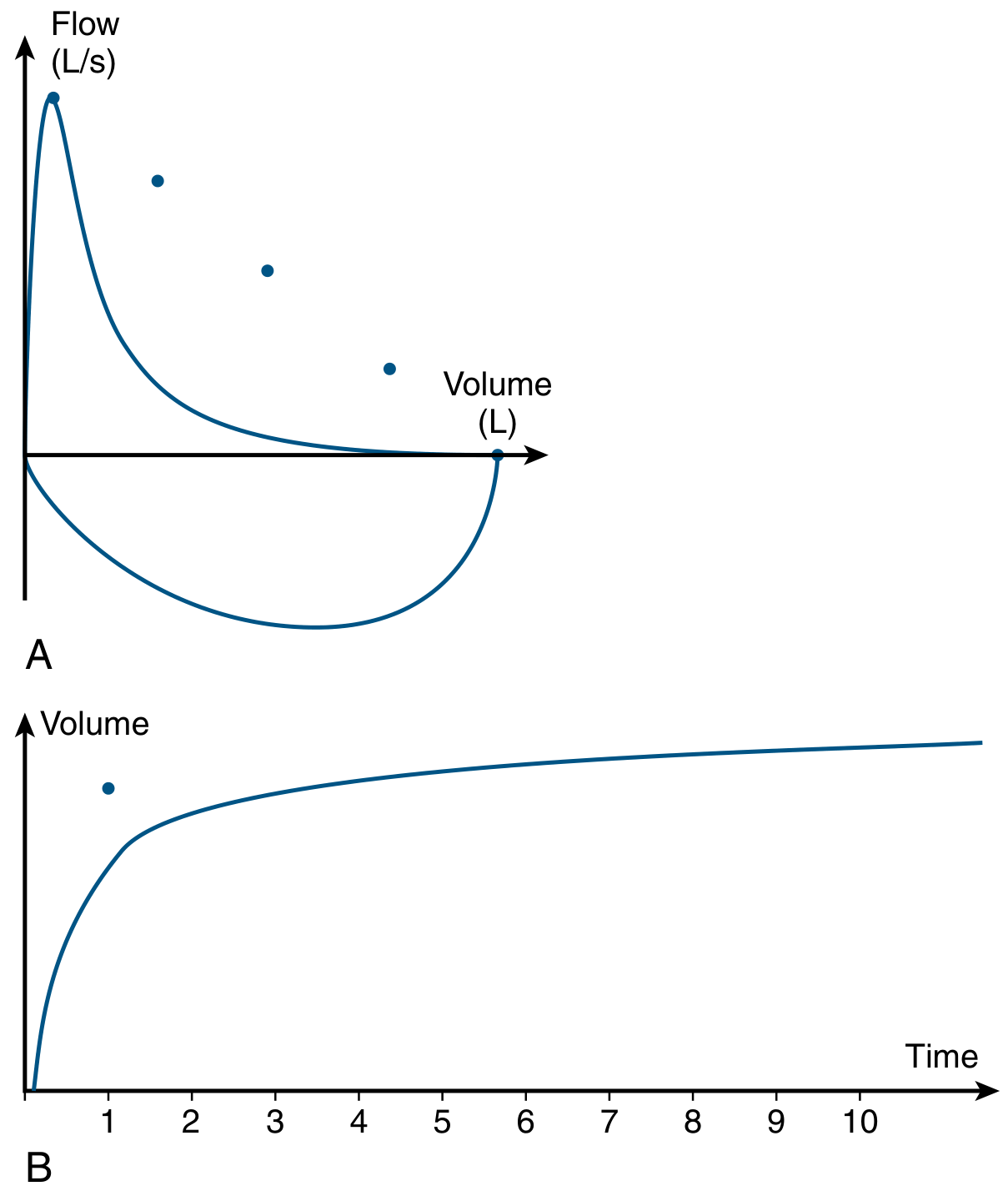
(A) Concave (scooped) expiratory flow-volume loop - flow is reduced at all lung volumes. (B) Volume-time curve showing prolonged expiratory time. The dot indicates predicted FEV₁.
3. GOLD Severity Classification (Post-Bronchodilator FEV₁)
Once airflow obstruction is confirmed (FEV₁/FVC < 0.70), severity is graded by FEV₁:
| GOLD Grade | Severity | Post-BD FEV₁ (% predicted) |
|---|---|---|
| GOLD 1 | Mild | ≥ 80% |
| GOLD 2 | Moderate | 50 - 79% |
| GOLD 3 | Severe | 30 - 49% |
| GOLD 4 | Very Severe | < 30% (or < 50% with PaO₂ < 60 mmHg) |
- Washington Manual of Medical Therapeutics, p. 313; Fishman's, p. 726
4. GOLD ABCD Assessment (Symptom + Exacerbation Risk)
Beyond spirometry, COPD is categorized combining symptoms and exacerbation history:
- Symptoms assessed with:
- CAT (COPD Assessment Test) - score 0-40; ≥ 10 = more symptoms
- mMRC Dyspnea Scale - grades 0-4 (see below)
- Exacerbation risk: ≥ 2 moderate exacerbations/year OR ≥ 1 hospitalization = high risk
mMRC Dyspnea Scale
| Grade | Description |
|---|---|
| 0 | Breathless only with strenuous exercise |
| 1 | Breathless hurrying on the level or up a slight hill |
| 2 | Walks slower than peers due to breathlessness, or stops when walking at own pace |
| 3 | Stops for breath after ~100 yards or after a few minutes on the level |
| 4 | Too breathless to leave the house, or breathless when dressing |
- Fishman's Pulmonary Diseases and Disorders, p. 726
5. Additional Pulmonary Function Tests
| Test | Finding in COPD | Clinical Use |
|---|---|---|
| Lung volumes (TLC, FRC, RV) | Elevated (hyperinflation, air trapping) | Exclude restrictive disease |
| DLCO (diffusing capacity for CO) | Reduced (in emphysema) | Indicator of emphysema; independent predictor of mortality |
| 6-Minute Walk Test (6MWT) | Distance < 450 m (abnormal) | Submaximal exercise test; component of multidimensional mortality scores; unmasks exercise-induced hypoxemia |
- Washington Manual of Medical Therapeutics, p. 313
6. Laboratory Studies
| Test | Indication |
|---|---|
| Arterial Blood Gas (ABG) | Recommended in severe COPD (GOLD 3-4); assesses hypoxemia and hypercapnia |
| Serum bicarbonate (elevated) | Suggests chronic hypercapnia (compensated respiratory acidosis) |
| Complete blood count | Polycythemia may reflect chronic hypoxemia |
| Peripheral eosinophils | > 300 cells/µL supports initial use of inhaled corticosteroid (ICS) |
| Alpha-1 antitrypsin (A1AT) level | All COPD patients should be screened at least once - unique comorbidities (liver disease) and replacement therapy available for severe deficiency |
Conditions that should prompt A1AT testing:
-
Early-onset emphysema (age < 45 years)
-
Emphysema in a non-smoker
-
Basilar-predominant emphysema (panacinar pattern)
-
Family history of early-onset emphysema or non-smoking related emphysema
-
Family history of cirrhosis
-
Bronchiectasis without other etiology
-
c-ANCA positive vasculitis (e.g., GPA)
-
Necrotizing panniculitis (Weber-Christian disease)
-
Fishman's Pulmonary Diseases and Disorders, p. 726; Washington Manual, p. 313
7. Imaging
Chest X-Ray (CXR)
- Not sensitive for diagnosing COPD - primarily used to rule out alternative diagnoses and establish baseline
- Signs of hyperinflation in advanced disease:
- Flattening of the diaphragm
- Increased retrosternal / retrocardiac air spaces
- Lung hyperlucency with diminished vascular markings
- Bullae
Chest CT (HRCT)
-
More sensitive than CXR for detecting emphysema
-
Detects: emphysema, airway wall thickening, air trapping, bullae
-
Also screens for lung cancer and atherosclerosis in at-risk smokers
-
Symptomatic smokers with normal spirometry may still have CT abnormalities
-
In severe disease, CT determines candidacy for lung volume reduction surgery (LVRS)
-
Quantitative HRCT analysis allows early emphysema detection but is not yet widely available clinically
-
Washington Manual of Medical Therapeutics, p. 313; Fishman's, p. 726
8. Summary Diagnostic Algorithm
Symptoms (chronic cough, dyspnea, sputum) + Risk factors (smoking, occupational exposure)
↓
Spirometry (post-bronchodilator)
↓
FEV₁/FVC < 0.70 → COPD CONFIRMED
↓
Grade severity by FEV₁ (GOLD 1-4)
Assess symptoms (CAT / mMRC) + Exacerbation risk
→ GOLD ABCD Group Assignment
↓
Supplementary tests:
• Lung volumes + DLCO
• ABG (if severe)
• A1AT level (all patients)
• Peripheral eosinophils
• CXR (baseline + exclude alternatives)
• CT chest (if indicated: severe, LVRS candidacy, suspected cancer)
Recent Evidence Note
A 2026 systematic review (Watson et al., PMID 41813011) highlights evolving definitions of "early COPD" and predictors for disease progression - emphasizing that radiographic and symptomatic abnormalities in at-risk smokers with normal spirometry may carry prognostic significance even before meeting traditional spirometric criteria. Current guidelines still require post-bronchodilator spirometry for diagnosis, but this area is under active investigation.
A 2025 meta-analysis (Robertson et al., PMID 39742912) examined Preserved Ratio Impaired Spirometry (PRISm) - a pattern where FEV₁/FVC is normal but FEV₁ is reduced - as an intermediate phenotype carrying independent cardiovascular and mortality risk, distinct from classical COPD.
This is a shared conversation. Sign in to Orris to start your own chat.