Give a example case of medical errorr
Reading File
Finding Sources
Reading File
Reading File
Here is a well-documented example case of a medical error, drawn from authoritative medical textbooks:
Example Case: Medication Error — Vancomycin Overdose Leading to Kidney Injury
Clinical Scenario:
A hospitalized patient is diagnosed with a serious methicillin-resistant Staphylococcus aureus (MRSA) infection and is appropriately prescribed vancomycin. The antibiotic is initiated correctly with the right dose and indication.
During the hospital stay, the patient is also given other nephrotoxic agents (e.g., aminoglycosides, NSAIDs, or contrast dye) simultaneously — without accounting for their combined effect on kidney function.
The vancomycin serum level becomes supratherapeutic (above safe levels), and the patient develops acute kidney injury (AKI).
Is this a medical error?
Yes. Because the nephrotoxicity was caused by the simultaneous administration of additional nephrotoxic agents — a preventable, human-made lapse in medication management — this is classified as a medical error, not merely an adverse event.
"If the serum level of antibiotic was supratherapeutic because the patient had simultaneously been given other nephrotoxic agents, then a medical error would have occurred." — Goldman-Cecil Medicine
Key Concepts This Case Illustrates
| Concept | Explanation |
|---|---|
| Medical Error | An act or omission leading to an unanticipated, undesirable outcome |
| Adverse Event vs. Error | Adverse events can occur even with perfect care (e.g., expected drug side effects). Errors are preventable |
| Medication Error | One of the most common types — affects 770,000+ patients/year in the U.S. (FDA data) |
| Swiss Cheese Model | Errors penetrate multiple layers of defense; no single failure alone usually causes harm |
Contributing Factors (Common in Real Cases)
- Polypharmacy — multiple drugs prescribed without checking interactions
- Poor handoff communication — one study found 50% of patients had at least one medication error at discharge
- Fatigue and work overload — longer shifts and more handoffs increase error rates
- Lack of electronic safety checks — absent or overridden drug interaction alerts in EMR systems
How It Should Have Been Prevented
- Medication reconciliation — reviewing all active drugs before adding nephrotoxic agents
- Electronic prescribing with drug-interaction alerts
- Regular monitoring of vancomycin serum levels and renal function
- Checklists and standardized protocols for high-risk medications
"Modern thinking emphasizes efforts to design and implement systems to prevent or catch errors... checklists, read-backs, and standardized safety procedures." — Goldman-Cecil Medicine
Sources: Goldman-Cecil Medicine; Kaplan & Sadock's Comprehensive Textbook of Psychiatry
Give me a easy one
Here is a simple, easy-to-understand example of a medical error:
Case: Wrong Medication Dose for a Child
What happened:
A 5-year-old child (20 kg) is brought to the hospital with a fever. The doctor prescribes paracetamol (acetaminophen).
The correct dose is 15 mg/kg → so the child should receive 300 mg.
The nurse misreads the handwritten prescription and gives 3,000 mg (10× the correct dose).
The child develops liver damage from the overdose.
Why This Is a Medical Error
| Step | What Went Wrong |
|---|---|
| Doctor | Wrote an unclear/illegible prescription |
| Nurse | Misread the dose — did not double-check |
| System | No second nurse verification for high-risk patients |
How It Could Have Been Prevented
- Clear, printed or electronic prescriptions (no handwriting)
- Double-checking doses by a second nurse before giving medication
- Weight-based dose calculators built into hospital systems
- Asking the patient/parent to confirm the medication before giving it
Bottom line: This is a classic medication error — the right drug, but the wrong dose. It was 100% preventable with basic safety checks.
For adult
Here is a simple, easy-to-understand medical error case for an adult:
Case: Wrong Patient Gets the Wrong Medication
What happened:
Two patients are admitted to the same hospital ward:
- Mr. Ali — diabetic, prescribed insulin
- Mr. Ahmed — recovering from surgery, prescribed warfarin (blood thinner)
The nurse is busy and in a rush. She picks up the medication tray without checking the wristband and gives Mr. Ali the warfarin meant for Mr. Ahmed.
Mr. Ali has no surgical wound, but warfarin thins his blood unnecessarily. He later develops internal bleeding.
Why This Is a Medical Error
| What went wrong | Detail |
|---|---|
| Nurse skipped ID check | Did not verify patient wristband |
| No second verification | High-risk drug given without double-check |
| Rushed environment | Workload led to shortcuts |
How It Could Have Been Prevented
- Always check 5 Rights before giving any drug:
- Right Patient
- Right Drug
- Right Dose
- Right Route
- Right Time
- Scan the patient's wristband barcode before giving medication
- Never skip ID verification, even when busy
Bottom line: A simple wristband check would have prevented serious harm. This is one of the most common — and most preventable — errors in hospitals.
Another example to make a skit
Here is a medical error example written as a short skit you can perform:
🎭 Skit: "The Rushed Nurse"
Topic: Wrong medication given due to poor communication
Setting: Hospital ward, morning medication round
Characters:
- Nurse Sara — busy, rushing through rounds
- Patient Mr. Hassan — 55 years old, admitted for high blood pressure
- Nurse Layla — senior nurse
Scene 1 — The Mistake
Nurse Sara walks quickly down the ward, holding two medication cups. She stops at Bed 4.
Sara: (not looking up from her clipboard) Good morning, here's your morning medication.
Mr. Hassan: Okay, thank you nurse.
Sara places the cup down and rushes off. Mr. Hassan takes the pills.
A few minutes later, Nurse Layla walks by and checks the medication chart.
Layla: (alarmed) Sara! Wait — Mr. Hassan in Bed 4 is supposed to get amlodipine for blood pressure. Did you give him the metformin from Bed 5 by mistake?
Sara: (stops, goes pale) I... I didn't check his wristband. I thought Bed 4 was the diabetic patient.
Layla: The diabetic patient moved to Bed 5 this morning during the shift change. Nobody told you?
Sara: No one updated the board...
Scene 2 — The Consequences
Both nurses go to Mr. Hassan.
Layla: Mr. Hassan, what did you just take?
Mr. Hassan: The white tablets the nurse gave me. Is something wrong?
Layla: (calmly) Don't worry, we are going to take care of you. (turns to Sara quietly) He received metformin. He's not diabetic — his blood sugar could drop. Call the doctor now and document this immediately.
Sara: (guilty) I should have checked. I was rushing and I assumed...
Layla: In nursing, we never assume.
Scene 3 — The Lesson
Doctor arrives, assesses Mr. Hassan, and he is monitored safely. Later, Sara and Layla debrief.
Layla: Sara, what should you have done before giving any medication?
Sara: Check the 5 Rights — right patient, right drug, right dose, right route, right time. And scan his wristband.
Layla: And what else failed today?
Sara: The handover. Nobody told me the patient in Bed 5 had changed. Communication broke down during the shift change.
Layla: Exactly. The error was not just yours. The system failed too. That is why we report it — not to punish, but to fix the system.
Sara: I will report it and make sure this never happens again.
💡 Key Messages (can be said directly to the audience at the end)
- Always verify patient identity before giving medication
- Clear handover communication between shifts saves lives
- Blame the system, not just the person — errors are often multi-factorial
- Reporting errors is not shameful — it protects future patients
Running time: ~5–7 minutes. Can be adapted for nursing students, hospital training, or patient safety workshops.
Stroke vs vertigo
Finding Sources
Reading File
Reading File
Reading File
Reading File
Here is a clear comparison of Stroke vs. Vertigo — two conditions that are commonly confused in clinical practice:
Stroke vs. Vertigo — Key Differences
The Core Challenge
Both can present with dizziness and unsteadiness. The critical task is distinguishing a dangerous central cause (stroke) from a benign peripheral cause (e.g., BPPV, vestibular neuritis).
"Approximately 4% of ED visits are from dizziness, and strokes are the underlying cause in approximately 5% of those visits." — Rosen's Emergency Medicine
Side-by-Side Comparison
| Feature | Peripheral Vertigo (e.g., BPPV, Vestibular Neuritis) | Central Vertigo / Stroke |
|---|---|---|
| Onset | Gradual or triggered by head movement | Sudden ("thunderclap") |
| Type of dizziness | Spinning sensation (room spinning) | Vague unsteadiness, off-balance |
| Duration | Seconds (BPPV) to days (neuritis) | Constant, persistent |
| Nausea/Vomiting | Common | May be present |
| Hearing loss/Tinnitus | Possible (Ménière's, labyrinthitis) | Uncommon |
| Neurological signs | Usually absent | Present — slurred speech, weakness, double vision, numbness |
| Gait | Can walk, veers toward lesion side | Often cannot stand without support |
| Nystagmus direction | Fixed direction, horizontal | Direction-changing, vertical, or downbeating |
| Head Impulse Test | Positive (corrective saccade) → peripheral/benign | Negative → central/worrying |
| Risk factors | Viral illness, head position change | Hypertension, diabetes, atrial fibrillation, prior stroke, older age |
| Imaging (MRI) | Normal | Abnormal — infarct or hemorrhage |
Red Flags That Suggest Stroke, Not Benign Vertigo
🚨 Any ONE of these should raise concern:
- Sudden onset with no positional trigger
- Cannot stand or walk at all
- Direction-changing nystagmus on gaze
- Vertical or downbeating nystagmus
- Skew deviation (one eye higher than the other)
- Other neurological symptoms — facial droop, arm weakness, speech difficulty
- Negative head impulse test in a patient with constant vertigo
- Vascular risk factors (HTN, diabetes, AF, age >60)
The HINTS Exam (Bedside Test)
Used in patients with acute, constant vertigo to differentiate stroke from vestibular neuritis:
| Component | Finding | Interpretation |
|---|---|---|
| Head Impulse Test | Positive (corrective saccade seen) | Peripheral (benign) |
| Negative (no saccade) | Central (stroke possible) | |
| Nystagmus | Unidirectional | Peripheral |
| Direction-changing | Central (stroke) | |
| Test of Skew | No vertical misalignment | Peripheral |
| Skew deviation present | Central (brainstem stroke) |
"Direction-changing nystagmus when the patient looks to the left or right may indicate a stroke in a patient with acute vestibular syndrome." — Rosen's Emergency Medicine
⚠️ Note: HINTS should only be performed by experienced clinicians and is not reliable in isolation — always combine with clinical judgment and imaging when uncertain.
Simple Memory Aid
"BENIGN vertigo = spins with head movement, you can still walk, nystagmus goes one way." "STROKE vertigo = sudden, can't walk, direction-changing nystagmus, + other neuro signs."
Source: Rosen's Emergency Medicine — Concepts and Clinical Practice
Give pharmacological class n mechanism of action of warfarin
Finding Sources
Reading File
Reading File
Loading Image
Warfarin — Pharmacological Class & Mechanism of Action
Pharmacological Class
| Class | Oral Anticoagulant |
| Subclass | Vitamin K Antagonist (VKA) |
| Chemical type | Coumarin derivative |
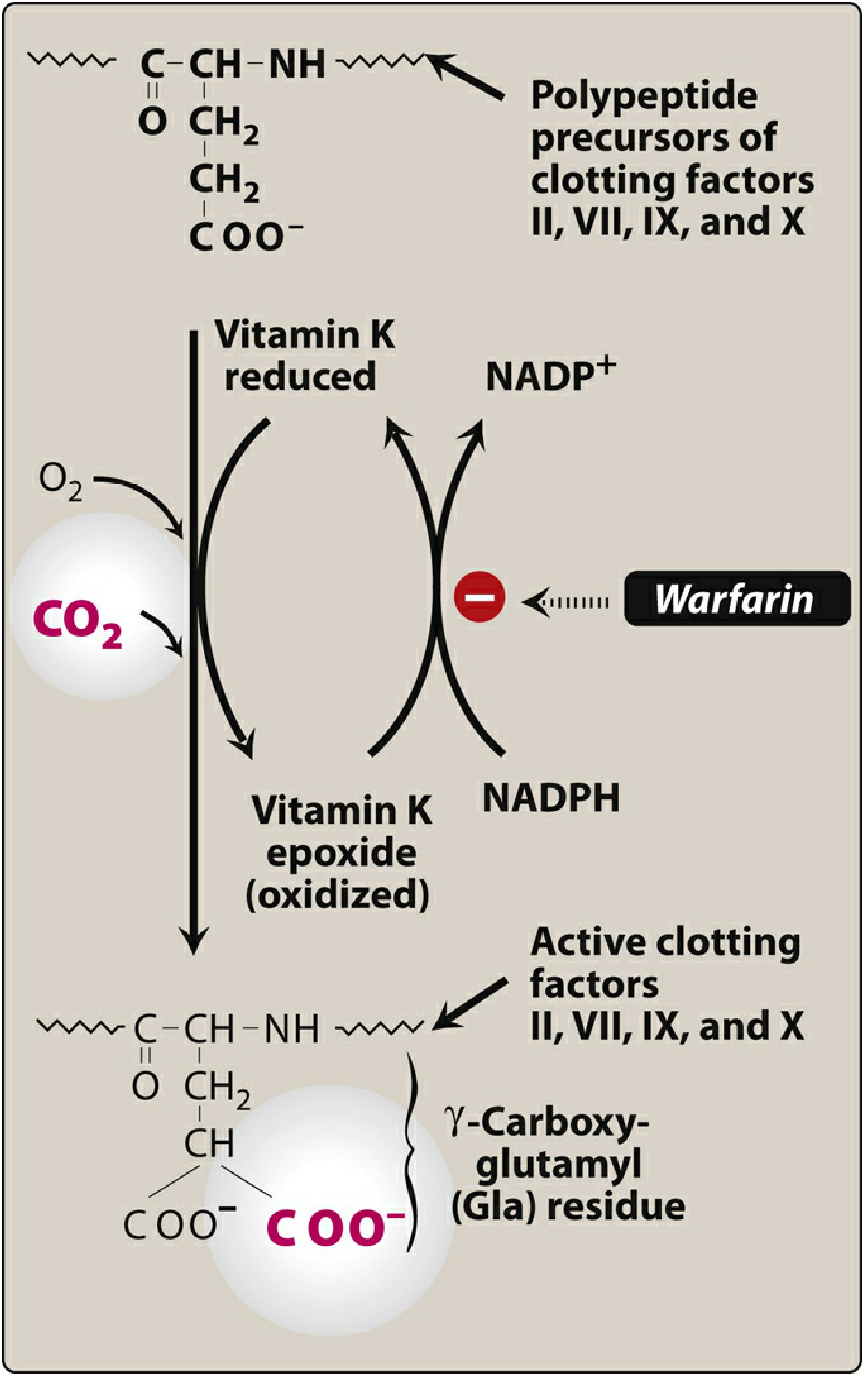
Mechanism of Action
Warfarin works by blocking the Vitamin K cycle, which is essential for producing active clotting factors.
Step-by-step:
- Clotting factors II, VII, IX, and X require Vitamin K as a cofactor to become active in the liver
- During activation, these factors undergo γ-carboxylation — a process that adds a carboxyl group to glutamic acid residues, converting them into γ-carboxyglutamic acid (Gla) residues
- This Gla modification allows clotting factors to bind calcium and attach to platelet membranes — essential for clot formation
- During this process, Vitamin K is oxidized → becomes Vitamin K epoxide
- Normally, Vitamin K epoxide reductase (VKOR) converts it back to active (reduced) Vitamin K to be reused
- Warfarin inhibits VKOR → Vitamin K is NOT recycled → reduced Vitamin K is depleted
- Without sufficient reduced Vitamin K, clotting factors II, VII, IX, X (and Proteins C & S) are produced with little to no biological activity
- Result: Reduced clot formation = anticoagulation
Key Points to Remember
| Feature | Detail |
|---|---|
| Target enzyme | Vitamin K epoxide reductase (VKOR / VKORC1) |
| Affected factors | II, VII, IX, X (+ Proteins C & S) |
| Active enantiomer | S-warfarin (more potent than R-warfarin) |
| Onset of action | Delayed — 72 to 96 hours (time needed to deplete existing clotting factors) |
| Metabolism | CYP2C9 (liver) |
| Antidote | Vitamin K (reversal takes ~24 hours) |
| Route | Oral only |
| Monitoring | INR (International Normalized Ratio) |
Why is the onset delayed?
Because warfarin does not inactivate existing clotting factors — it only prevents new ones from being made. You have to wait until the already-circulating active factors are used up (depleted). That's why in urgent situations, heparin is given alongside warfarin as a "bridge."
"Peak effects may be delayed for 72 to 96 hours, which is the time required to deplete the pool of circulating clotting factors." — Lippincott Illustrated Reviews: Pharmacology
Sources: Lippincott Illustrated Reviews: Pharmacology; Harrison's Principles of Internal Medicine 22E
what happens if you proscribed antidiabetic drug to a hypertensive patient
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
This is essentially a medication error scenario — prescribing an antidiabetic drug to a patient who does not have diabetes. Here is a full clinical breakdown:
What Happens When an Antidiabetic Drug is Given to a Hypertensive (Non-Diabetic) Patient?
The Core Problem
A hypertensive patient has normal blood glucose regulation. Their pancreas already produces sufficient insulin and their glucose levels are controlled. Adding an antidiabetic drug disrupts this balance.
The outcome depends heavily on which drug was given:
By Drug Class
1. Insulin or Sulfonylureas (e.g., glibenclamide, glipizide)
Most dangerous — cause significant hypoglycemia
These drugs force blood glucose down regardless of the patient's actual glucose level.
What happens:
| Stage | Blood Glucose | Symptoms |
|---|---|---|
| Early | ~60–70 mg/dL | Sweating, trembling, palpitations, anxiety, hunger |
| Moderate | ~50 mg/dL | Confusion, dizziness, difficulty speaking, blurred vision |
| Severe | <40 mg/dL | Seizures, loss of consciousness, coma |
| Critical | Untreated | Brain damage, cardiac arrhythmia, death |
"The signs and symptoms of hypoglycemia include dizziness, confusion, sweating, palpitations, and tachycardia; if hypoglycemia persists, loss of consciousness may occur." — Robbins & Kumar Basic Pathology
Extra danger in hypertensive patients: Beta-blockers (commonly used for hypertension) mask the warning signs of hypoglycemia (especially tachycardia and tremor), so the patient may not realize they are becoming dangerously hypoglycemic.
2. Metformin
Lower immediate risk, but still harmful
Metformin has a low risk of causing hypoglycemia on its own, but in a non-diabetic patient it can still cause:
- Nausea, vomiting, diarrhea, abdominal pain
- Loss of appetite and unintended weight loss
- Lactic acidosis (rare but serious — especially if the patient has kidney or heart problems, which are common in hypertensives)
- Vitamin B12 deficiency with long-term use
3. SGLT2 Inhibitors (e.g., empagliflozin, dapagliflozin)
- Force glucose excretion through urine
- Can cause urinary tract infections, genital infections, and dehydration
- Dehydration worsens in hypertensive patients already on diuretics
- Risk of hypotension (dangerously low blood pressure)
4. GLP-1 Agonists (e.g., semaglutide, liraglutide)
- Cause significant nausea, vomiting, weight loss
- Low hypoglycemia risk alone, but unpleasant side effects
- Can cause dehydration and low blood pressure
Summary Table
| Drug Class | Risk Level | Main Danger |
|---|---|---|
| Insulin | 🔴 Very High | Severe hypoglycemia → coma |
| Sulfonylureas | 🔴 High | Hypoglycemia → seizures |
| Metformin | 🟡 Moderate | Lactic acidosis, GI symptoms |
| SGLT2 Inhibitors | 🟡 Moderate | Dehydration, UTI, hypotension |
| GLP-1 Agonists | 🟢 Lower | Nausea, weight loss, dehydration |
In the Context of Medical Error
This is a classic wrong-drug medication error. Contributing factors:
- Similar-looking patient names on charts
- Poor handover communication
- Failure to verify the patient's diagnosis before prescribing
- No pharmacist review or medication reconciliation
Prevention:
- Always confirm the indication before prescribing any drug
- Pharmacist double-check on all prescriptions
- Electronic prescribing systems that flag drugs against the patient's diagnosis
Sources: Robbins & Kumar Basic Pathology; Braunwald's Heart Disease; Tintinalli's Emergency Medicine
Narrate to wrong medication wrong skit
Here is a full narrated skit based on the wrong medication given to the wrong patient — specifically, an antidiabetic drug given to a hypertensive patient:
🎭 Skit: "One Mistake Too Many"
Topic: Wrong drug given to wrong patient (antidiabetic drug → hypertensive patient)
Setting: General medical ward, morning medication round
Characters:
- Narrator
- Nurse Amir — junior nurse, first week on the ward
- Patient Mr. Rajan — 58 years old, admitted for high blood pressure
- Patient Mr. Gopal — 60 years old, in the next bed, admitted for Type 2 diabetes
- Dr. Priya — ward doctor
- Nurse Head Farah — senior charge nurse
🎙️ NARRATOR:
It is 8:00 in the morning. The ward is busy. Nurses are rushing through medication rounds before the doctor's visit. Nurse Amir has just received his medication trolley and is preparing to distribute the morning drugs. He is new, eager, and unfortunately — moving too fast.
Scene 1 — The Setup
Nurse Amir pushes the trolley down the ward. He picks up two medication cups. One contains amlodipine for Mr. Rajan in Bed 3 — a calcium channel blocker for hypertension. The other contains metformin for Mr. Gopal in Bed 4 — an antidiabetic tablet.
Narrator: Nurse Amir approaches Bed 3. Mr. Rajan is sitting up reading a newspaper. Mr. Gopal in Bed 4 is asleep. Amir glances at the cups, glances at the bed numbers... and hesitates for just a second.
Amir: (quietly to himself) Bed 3... Bed 4... okay.
He places the metformin cup — meant for Bed 4 — on Mr. Rajan's tray.
Amir: Good morning sir, here is your morning tablet.
Mr. Rajan: Thank you nurse. (swallows the tablet without question)
Amir moves to Bed 4 and wakes Mr. Gopal.
Amir: Good morning sir, your medication.
He places the amlodipine — meant for Mr. Rajan — in front of Mr. Gopal.
Mr. Gopal: (groggy) Mm... okay. (takes the tablet)
Narrator: Two patients. Two medications. Both swapped. And Nurse Amir walks away without checking a single wristband.
Scene 2 — The Signs Begin
Thirty minutes later. Mr. Rajan calls out from Bed 3.
Mr. Rajan: (anxious) Nurse... nurse! I feel strange. My stomach is turning. I feel dizzy.
Nurse Farah walks over quickly.
Farah: What is wrong, Mr. Rajan? Tell me exactly how you feel.
Mr. Rajan: I feel nauseous. My head is spinning. I am sweating. And I feel... weak. Very weak.
Farah checks his vitals. His blood pressure is normal but his blood glucose reading shows — 3.1 mmol/L. Dangerously low.
Farah: (alarmed, checks the chart) Your blood glucose is very low. But Mr. Rajan — you are not diabetic!
She picks up the medication cup still on his tray. She reads the label — METFORMIN 500mg.
Farah: (under her breath) This is not his medication...
She looks at Bed 4. Mr. Gopal is now sitting up, looking fine — because amlodipine, while not his drug, did not cause him immediate harm.
Narrator: Nurse Farah now understands exactly what happened. The medications were swapped. Mr. Rajan — a non-diabetic — received metformin. His blood sugar has dropped. He is experiencing hypoglycemia. This is a medical emergency.
Scene 3 — The Emergency
Farah calls for the doctor immediately.
Farah: Dr. Priya — come to Bed 3 urgently. Possible wrong medication. Patient is hypoglycemic.
Dr. Priya arrives, examines Mr. Rajan.
Dr. Priya: Mr. Rajan, how are you feeling right now?
Mr. Rajan: (pale, sweating) Doctor... I cannot think clearly. My hands are shaking. Am I going to be okay?
Dr. Priya: You will be fine. We are going to give you glucose right now. (to Farah) Give him 25g of oral glucose immediately. Monitor his blood sugar every 15 minutes. And check Mr. Gopal's BP — he may have received amlodipine.
Farah brings glucose drink. Mr. Rajan drinks it slowly. His colour gradually returns.
Narrator: Within 20 minutes, Mr. Rajan's blood glucose returns to normal. He is lucky. The metformin was a single dose. Had it been insulin — he could have lost consciousness. Had this gone unnoticed for longer — the outcome could have been catastrophic.
Scene 4 — The Confrontation
Later. Nurse Head Farah calls Nurse Amir aside.
Farah: Amir. Did you check Mr. Rajan's wristband before giving his medication this morning?
Amir: (looking down) I... I looked at the bed number. I thought—
Farah: Bed numbers change. Patients move. Wristbands do not lie. Did you check it?
Amir: (quietly) No.
Farah: Did you confirm the medication name against his chart?
Amir: No.
Farah: Did you ask him his name before giving the tablet?
Amir: (long pause) No.
Farah: You skipped all three checks. Three opportunities to catch this — and all three were missed. Mr. Rajan is fine now. But what if he was alone, fell unconscious, and nobody found him in time?
Amir is silent.
Farah: This is not about blaming you. You made a mistake and I want you to learn from it — not be destroyed by it. But you must report this in the incident form today. Every error we report protects the next patient.
Scene 5 — The Lesson
Amir sits with Farah. She opens the medication policy.
Farah: What are the 5 Rights of medication administration?
Amir: Right patient... right drug... right dose... right route... right time.
Farah: And how do you confirm the right patient?
Amir: Check the wristband. Ask the patient to state their name. Match it to the medication chart.
Farah: Every. Single. Time. No shortcuts. Not when you are busy. Not when you think you already know. Every time.
Amir: I understand. I am sorry.
Farah: Good. Now write the incident report — honestly and completely. That is how we fix systems, not just people.
🎙️ NARRATOR (closing):
That afternoon, the ward updated its process. A double-check policy was introduced for all medications. Wristband scanning was made mandatory. And Nurse Amir — though shaken — became one of the most careful nurses on the floor. Because he learned the hardest lesson in nursing:
"The moment you assume — you put a patient at risk."
💡 Key Messages for the Audience
- Always check the wristband — never rely on bed numbers
- Ask the patient to state their name before every medication
- Verify the drug against the chart — every time, no exceptions
- Wrong drug in a wrong patient can cause serious harm — even death
- Reporting errors is not punishment — it builds a safer system for everyone
Estimated performance time: 8–12 minutes. Suitable for nursing students, ward training days, and patient safety workshops.
This is a shared conversation. Sign in to Orris to start your own chat.