Left anterior fascicular block note
Reading File
Finding Sources
Finding Sources
Searching Images
left anterior fascicular block ECG
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Loading Image
Here is a comprehensive note on Left Anterior Fascicular Block (LAFB).
Left Anterior Fascicular Block (LAFB)
Anatomy & Mechanism
The left bundle branch divides into two fascicles:
- Anterior (superior) fascicle — thin, long, supplied mainly by the LAD; conducts to the anterolateral LV
- Posterior (inferior) fascicle — thicker, shorter, dual blood supply (LAD + RCA); more resistant to block
Block of the anterior fascicle forces depolarization to proceed first through the posterior fascicle (inferiorly and rightward), then swings superiorly and leftward — producing the characteristic marked left axis deviation. Because the block is within the fascicle (not the bundle itself), it does not significantly widen the QRS.
ECG Criteria
| Parameter | Finding |
|---|---|
| QRS duration | < 120 ms (normal) |
| Frontal axis | −45° to −90° (marked left axis deviation) |
| Lead I, aVL | qR pattern (small q, tall R) |
| Leads II, III, aVF | rS pattern (small r, deep S) |
| Precordial | Delayed R-wave transition (late transition) |
| ST-T waves | Normal |
Axis threshold: Most authorities use more negative than −45° as the cutoff. Harrison's states it is "probably the most common cause of marked left axis deviation in adults."
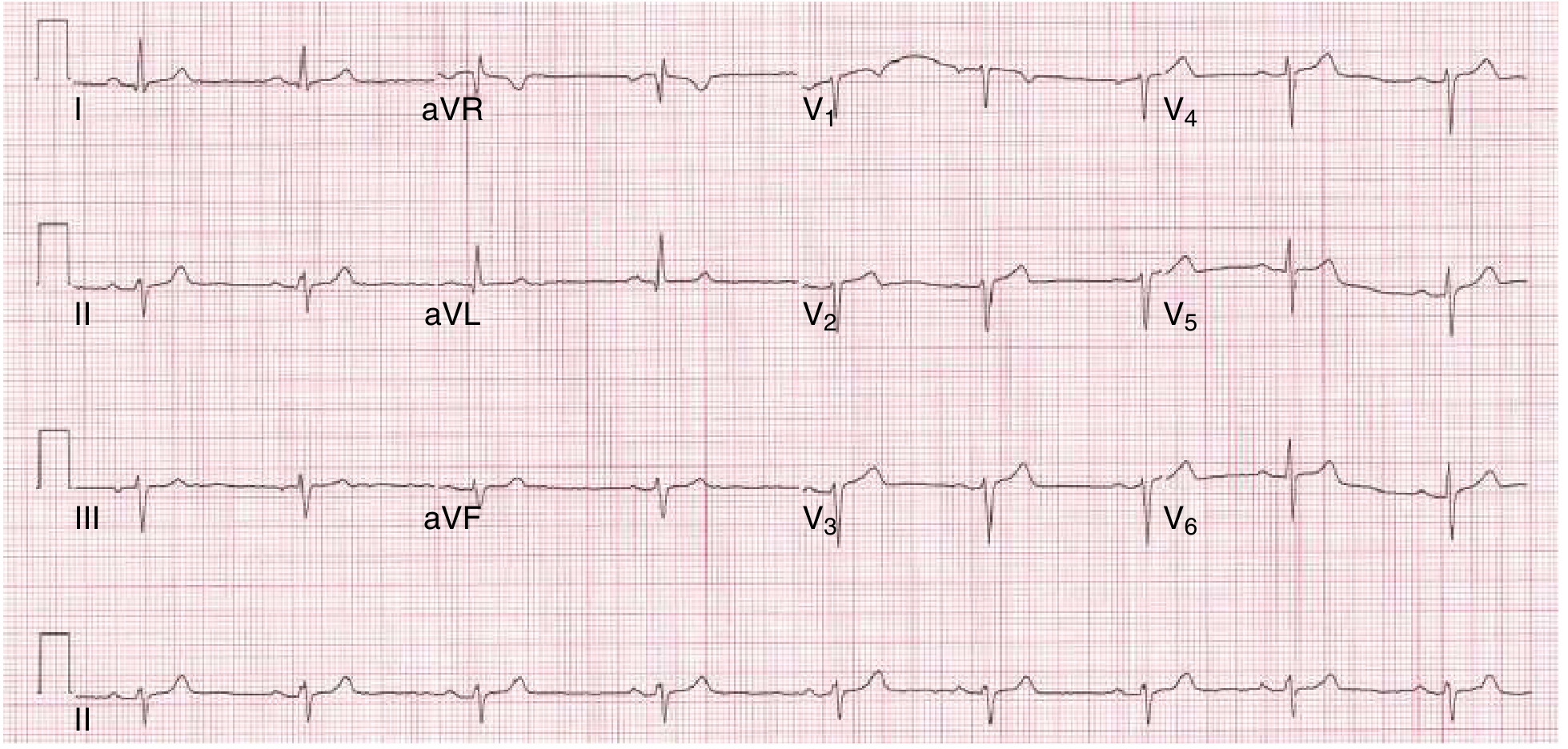
Below is the ECG from Goldman-Cecil Medicine (Fig. 42-5A) showing classic LAFB — left axis deviation ~−60°, normal QRS duration, qR in I/aVL, rS in inferior leads:
Epidemiology & Causes
- Found in ~1% of otherwise healthy adults
- Prevalence of any bundle branch block rises from ~1% at age 50 to ~17% at age 80
- Common causes:
- Degenerative/fibrotic disease of the conduction system (most common)
- Coronary artery disease / ischemic heart disease
- Hypertensive heart disease
- Cardiomyopathy
- Aortic valve disease (including post-TAVR)
- Chagas disease
- Infiltrative disease (amyloid, sarcoid)
- Myocarditis
Clinical Features
- Typically asymptomatic — LAFB itself causes no hemodynamic compromise
- No significant ventricular dyssynchrony (unlike LBBB)
- Clinical importance lies in what it accompanies or progresses to
Combinations & Clinical Significance
LAFB + RBBB = Bifascicular Block
Two of three fascicles are blocked. The ECG shows:
- Wide QRS (≥120 ms) with RBBB morphology (rsR′ in V1, wide S in I/V5-6)
- Left axis deviation (−45° to −90°)
- High risk for progression to complete heart block, especially in acute MI
Bifascicular Block + PR Prolongation = Trifascicular Block
Implies disease in all three fascicles. Very high risk for complete AV block — pacemaker often placed prophylactically, especially with acute MI.
Evaluation
- Compare to prior ECGs — determine if new or chronic
- Echocardiography — assess LV function, structural disease
- Stress test (echo or nuclear) — rule out ischemic heart disease
- Cardiac MRI — if infiltrative cardiomyopathy suspected
- Rhythm monitoring — if associated with prolonged PR, alternating blocks, or symptoms of syncope/presyncope
Management & Treatment
- Isolated LAFB, asymptomatic: No specific treatment; treat underlying cause; follow-up
- LAFB + symptoms (syncope/presyncope): Evaluate for higher-degree block; consider EP study
- Bifascicular block + syncope: Pacemaker implantation preferred over implantable cardiac monitor, regardless of block morphology or PR interval
- Bifascicular block + new PR prolongation: Prophylactic pacemaker often placed due to high risk of progression to complete heart block
- In acute MI with new bifascicular block: Pacemaker often placed prophylactically
Prognosis
- Isolated LAFB in a structurally normal heart: prognosis is benign; risk not significantly elevated above baseline
- With underlying heart disease: increased mortality risk
- LAFB + RBBB (bifascicular): portends higher long-term risk of requiring a permanent pacemaker, but prophylactic pacing is not indicated without symptoms such as syncope
Summary Table — LAFB vs. Other Fascicular Blocks
| Block | Axis | QRS Width | Key Morphology |
|---|---|---|---|
| LAFB | −45° to −90° | Normal (<120 ms) | qR in I/aVL; rS in II, III, aVF |
| LPFB | +90° to +180° | Normal (<120 ms) | rS in I/aVL; qR in III, aVF |
| RBBB | Normal | Wide (≥120 ms) | rsR′ in V1; wide S in I/V6 |
| RBBB + LAFB | −45° to −90° | Wide (≥120 ms) | RBBB + left axis |
| LBBB | Variable/left | Wide (≥120 ms) | Broad notched R in I/V5-6; no septal q |
Sources: Goldman-Cecil Medicine, 26th Ed. (Ch. 42); Harrison's Principles of Internal Medicine, 22nd Ed. (Ch. 247); Fuster & Hurst's The Heart, 15th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.