Cotton ball chest x ray
Reading File
Finding Sources
Searching Images
cotton ball appearance chest x-ray
Finding Sources
Loading Image
Loading Image
Loading Image
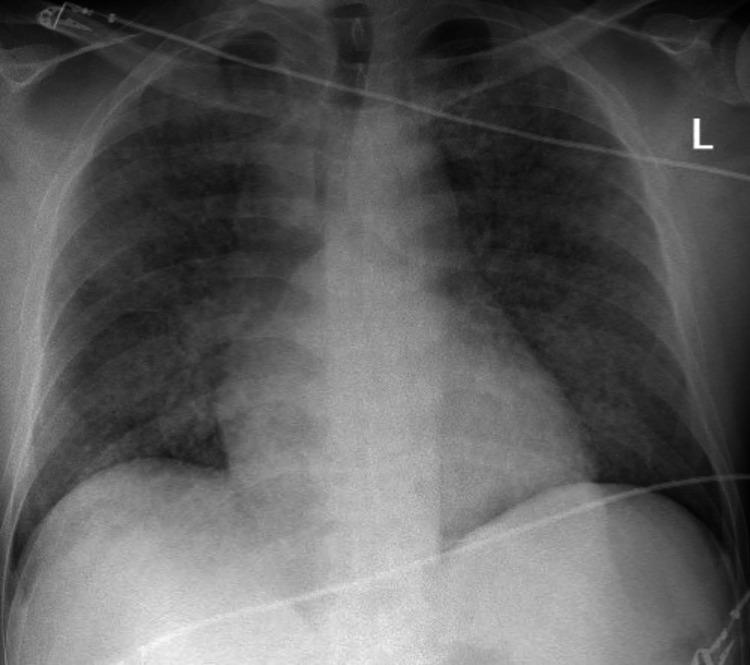
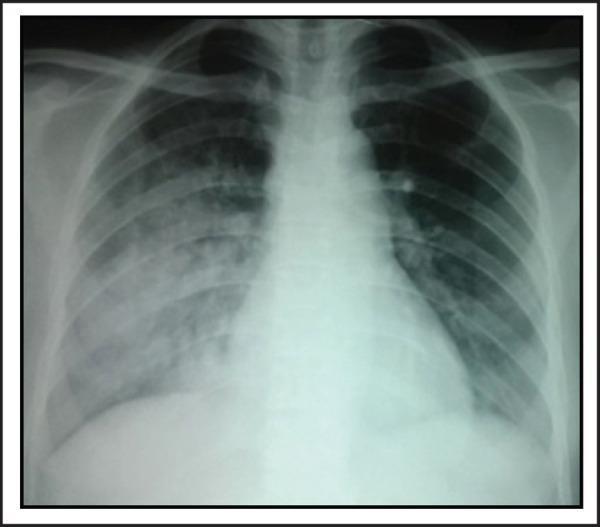
The "cotton ball" (or "cotton-wool") appearance on chest X-ray refers to fluffy, ill-defined, rounded opacities scattered through the lung fields. Here is a comprehensive breakdown:
Cotton-Ball / Cotton-Wool Opacities on Chest X-Ray
What Does It Look Like?
Soft, fluffy, poorly marginated white opacities — resembling clumps of cotton — distributed bilaterally through the lung fields. The borders are hazy rather than sharp.
Key Causes (Differential Diagnosis)
| Cause | Context / Clues |
|---|---|
| Pulmonary edema | Perihilar ("bat-wing") distribution, cardiomegaly, Kerley B lines, pleural effusions |
| Diffuse alveolar hemorrhage (DAH) | Hemoptysis, anemia, rapidly worsening CXR; seen in SLE, Goodpasture's, vasculitis, anti-GBM disease |
| Meconium aspiration syndrome (MAS) | Neonate, coarse asymmetric opacities, hyperinflation, flat diaphragms |
| Pneumocystis jirovecii pneumonia (PCP) | HIV/immunocompromised patient, bilateral perihilar ground-glass or fluffy opacities |
| Alveolar proteinosis | "Crazy-paving" pattern, bat-wing distribution |
| ARDS | Diffuse bilateral opacities following a precipitant (sepsis, trauma, aspiration) |
| Multifocal/atypical pneumonia | Patchy bilateral consolidation, systemic symptoms |
| Sarcoidosis | Upper/mid-zone nodules, hilar lymphadenopathy |
| Metastatic malignancy | Multiple discrete nodules (cannonball if large and round) |
Distinguishing Features by Pattern
Pulmonary edema
- Perihilar ("bat-wing") distribution
- Rapid change with diuresis
- Associated cardiomegaly, pleural effusions
Diffuse alveolar hemorrhage (DAH) in SLE
- Widespread, bilateral fluffy opacities
- No cardiomegaly
- Rapid onset
Meconium aspiration syndrome (neonate)
- Coarse, asymmetric patchy opacities
- Overinflated chest (horizontal ribs, flat diaphragms)
- Air trapping

Clinical Approach
- Is the patient a neonate? → Think MAS
- Is the patient immunocompromised (HIV, transplant)? → Think PCP, fungal
- Is there cardiomegaly / elevated JVP? → Think pulmonary edema
- Is there hemoptysis + anemia + autoimmune history? → Think DAH (SLE, Goodpasture's, ANCA vasculitis)
- Is there an acute precipitant (sepsis, trauma)? → Think ARDS
- Is it perihilar with hilar lymphadenopathy? → Think sarcoidosis
The "Cannonball" Variant
When the opacities are large, discrete, and sharply marginated (not fluffy), the term cannonball metastases is used — classically seen with renal cell carcinoma, choriocarcinoma, and testicular tumors. This is distinct from cotton-ball/cotton-wool opacities.
Summary: "Cotton ball" on CXR = alveolar-filling process. The key is correlating with clinical context — patient age, immune status, acuity of onset, and associated findings on the film.
Aspergillosis does it present
Finding Sources
Finding Sources
Reading File
Reading File
Searching Images
aspergillosis chest CT halo sign crescent sign fungal ball
Loading Image
Loading Image
Loading Image
Aspergillosis — Chest X-Ray / CT Presentations
Aspergillosis does not typically produce a cotton-ball pattern. Its radiological appearance depends on the form of disease. There are four distinct forms, each with a characteristic imaging pattern.
1. Invasive Pulmonary Aspergillosis (IPA)
Who: Severely immunocompromised — neutropenia, haematologic malignancy, post-transplant, high-dose steroids
Key imaging signs:
a) Halo Sign (early)
A nodule or mass surrounded by a rim of ground-glass opacity. The halo represents haemorrhagic infarction around an infarcted core — Aspergillus hyphae invade and occlude pulmonary arterioles, causing necrosis.
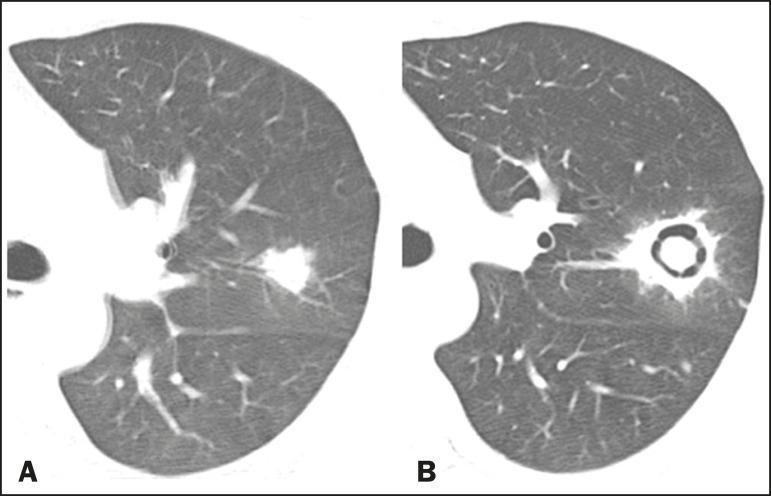
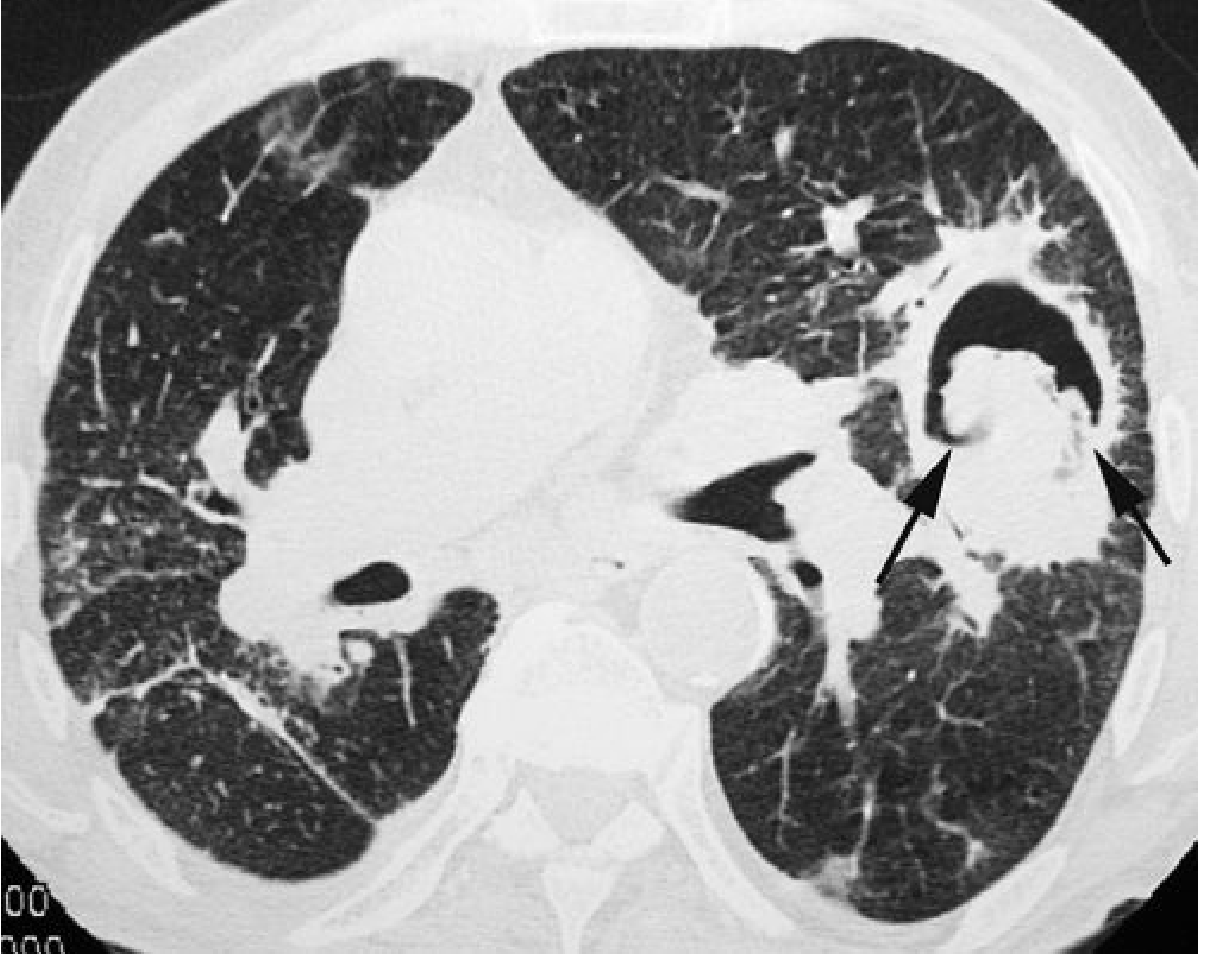
b) Air Crescent Sign (late)
A crescent of air appears between the cavity wall and the central necrotic fungal mass. This develops as the immune system recovers (typically neutrophil reconstitution) and the necrotic core retracts. It is a late sign and signals immune recovery.
c) Other patterns:
- Pleural-based, wedge-shaped consolidations (infarcts)
- Multiple bilateral nodules without halos
- Cavitation
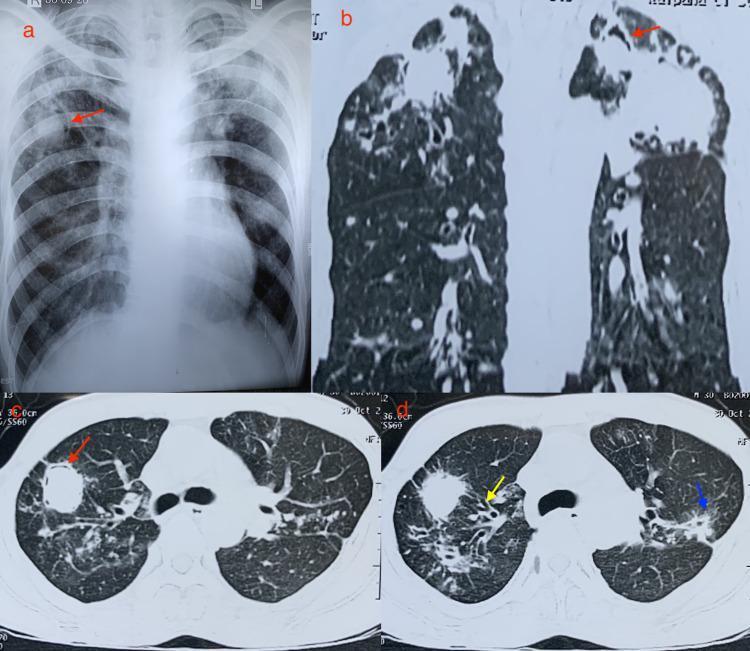
2. Aspergilloma (Fungus Ball)
Who: Pre-existing lung cavity (old TB, sarcoidosis, bronchiectasis)
Imaging: A rounded soft-tissue mass sitting within a cavity, separated from the wall by a crescent of air — the Monod sign (or air crescent sign in this context). The ball moves with position changes on decubitus films.
Symptoms: Haemoptysis (sometimes massive), chronic cough. Many are asymptomatic.
3. Allergic Bronchopulmonary Aspergillosis (ABPA)
Who: Asthma or cystic fibrosis patients with IgE-mediated hypersensitivity
Imaging:
- "Finger-in-glove" sign — branching tubular opacities from mucoid impaction in dilated bronchi (central bronchiectasis)
- Mucus plugs can be hyperdense on CT (up to 20% of cases) — high-attenuation mucus is characteristic
- Upper lobe predominance
- Transient, migratory consolidations
4. Chronic/Semi-Invasive Aspergillosis
Who: Mildly immunocompromised (diabetes, COPD, alcoholism, prolonged steroids)
Imaging:
- One or more poorly marginated upper lobe opacities
- Cavitation developing over weeks to months
- Pleural thickening
- Lesions may eventually resemble aspergilloma with an air crescent
Summary Table
| Form | Key Patients | Classic CXR/CT Sign |
|---|---|---|
| Invasive (IPA) | Neutropenic, transplant | Halo sign → air crescent sign |
| Aspergilloma | Prior TB/cavity | Fungus ball + Monod sign |
| ABPA | Asthma/CF | Finger-in-glove, central bronchiectasis |
| Chronic/semi-invasive | Mild immunocompromise | Upper lobe cavitation, pleural thickening |
To directly answer your question: Aspergillosis does not typically produce cotton-ball opacities. Its hallmark signs are the halo sign and air crescent sign (IPA), the fungus ball with Monod sign (aspergilloma), and the finger-in-glove sign (ABPA). — Murray & Nadel's Textbook of Respiratory Medicine; Grainger & Allison's Diagnostic Radiology
This is a shared conversation. Sign in to Orris to start your own chat.