different types of bandages Deep answer
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Now I have rich textbook content. Let me compile a comprehensive, well-organized answer on types of bandages drawing from all the gathered material plus foundational medical knowledge.
Types of Bandages — A Comprehensive Guide
Bandages serve as the outer retaining layer of a dressing system, or may themselves be the primary wound interface. They are classified by material/construction, function, and application technique.
1. Classification by Material & Construction
A. Gauze (Cotton/Cellulose) Bandages
The most widely used type. Basic cotton gauze is frequently composed of cotton plus cellulose acetate for increased absorbency. They are inexpensive and easy to use but have limited moisture-retentive capacity and may adhere to the wound bed. Can be:
- Plain gauze — used for packing, padding, or as secondary layers
- Impregnated gauze — infused with petrolatum (e.g. Vaseline® gauze, Adaptic™), soft paraffin wax, or antimicrobials (povidone-iodine, silver sulfadiazine, chlorhexidine). These are less adherent, can be molded into wound depressions, and are less painful on removal. Disadvantage: risk of maceration if left on too long.
— Dermatology 2-Volume Set 5e, p. 2961
B. Roller Bandages
Long strips of material wound into a roll. Applied in overlapping turns around a body part. Subtypes by material:
- Cotton crepe — conforming, slightly elastic, used for retention and light compression
- Elasticated (stretch) bandages — conform well to body contours, used for compression and support
- Cohesive/self-adherent (e.g. Coban™) — sticks to itself without adhesive, used for securing dressings, particularly over joints or digits; can cause skin tears if directly applied to intact skin
C. Tubular Bandages
Seamless tubes of cotton or elastic material applied over a limb or digit. Used as:
- Retention bandages post-dressing
- Digit protection (e.g. tubular gauze for finger wounds)
Warning: Tubular gauze over a finger wound should not be applied in more than two layers or twisted between layers — this can produce a tight bandage causing ischemic damage to the digit. — Tintinalli's Emergency Medicine, p. 335
D. Triangular Bandages
Large triangular cloth pieces. Used as slings (arm support), head bandages, or folded into broad/narrow-fold bandages for splint padding and immobilization.
E. Adhesive Bandages (Plasters)
Consist of a small absorbent pad attached to an adhesive strip. Used for minor wounds and abrasions. Repeated use over intact skin with plastic/paper tapes can cause skin tears and blistering.
2. Classification by Function
A. Retention/Securing Bandages
Hold dressings in place. Examples: gauze roller, tubular gauze, elastic adhesive bandage. Key principle — wrap loosely to allow adequate circulation, especially over extremities.
B. Compression Bandages
The most clinically significant category for chronic wound and vascular management. Three main types of graduated compression:
- Long-stretch (elastic) bandages — provide resting and working pressure; maintain compression both at rest and during movement. Examples: elastic crepe, four-layer bandage system.
- Short-stretch (inelastic) bandages — provide high working pressure during muscle contraction but low resting pressure. Examples: Unna's boot. Preferred for arterial or mixed venous/arterial disease due to lower resting pressure risk.
- Multi-layer compression bandage systems — combine several layers (e.g. wool, crepe, elastic, cohesive) to achieve sustained, graduated pressure. The four-layer bandage is the gold standard for venous ulcer management.
— Dermatology 2-Volume Set 5e; Mulholland & Greenfield's Surgery 7e
Compression Classes (by pressure at ankle):
| Class | Ankle Pressure | Clinical Use |
|---|---|---|
| Class I | 14–17 mmHg | Mild varicosities |
| Class II | 18–24 mmHg | Moderate venous insufficiency |
| Class III | 25–35 mmHg | Severe venous disease, venous ulcers |
| Class IV | >35 mmHg | Lymphedema |
C. Immobilization Bandages
Limit movement at a joint or fracture site:
- Sling-and-swathe — used after shoulder dislocation reduction, humeral fractures, and elbow injuries. A sling supports the arm; a swathe (binder) wraps around the body to immobilize it against the chest.
- Velpeau bandage — a specific sling-swathe configuration holding the arm in adduction and internal rotation.
- Figure-of-eight bandage — traditionally used for clavicle fractures; no longer recommended as it is uncomfortable and provides no additional benefit over a simple sling.
— Rosen's Emergency Medicine; Rockwood & Green's Fractures in Adults 10e
D. Pressure Bandages
Applied directly over wounds (e.g. post-biopsy, penetrating trauma, snakebite) to limit hemorrhage or venom spread. A pressure bandage with immobilization is a first-aid technique for snake envenomation.
E. Protective/Non-adherent Dressings
Placed directly on the wound bed:
- Low-adherent dressings (e.g. Melolin, Telfa) — reduce pain on removal
- Semi-permeable film dressings (e.g. Tegaderm, Op-Site) — transparent, allow oxygen exchange, maintain moist environment, used on superficial/incisional wounds
3. Advanced/Specialty Bandages (Wound Dressing Categories)
As wound care has evolved, the term "dressing" encompasses sophisticated materials that may also function as bandages:
| Type | Mechanism | Best Used For |
|---|---|---|
| Hydrocolloid (e.g. DuoDERM) | Absorbs exudate, maintains moist environment, forms gel | Partial/full-thickness wounds, pressure ulcers |
| Hydrogel | Donates moisture to dry wounds | Necrotic/dry wounds, burns |
| Foam dressings | High absorbency, non-adherent | Moderate–heavy exudate, malignant wounds |
| Alginate dressings | Derived from seaweed; gel-forming, hemostatic | Heavy exudate, full-thickness wounds |
| Negative Pressure (V.A.C.) | Subatmospheric pressure promotes granulation | Complex/deep wounds, surgical dehiscence |
| Activated charcoal (e.g. Actisorb Plus) | Absorbs odor | Malignant/malodorous wounds |
| Silver-containing dressings | Broad-spectrum antimicrobial (incl. MRSA, VRE) | Infected or critically colonized wounds |
— Pfenninger & Fowler's Procedures for Primary Care, 3e, p. 312
4. Bandage Selection by Wound Type
| Wound Type | Objective | Recommended Bandage/Dressing |
|---|---|---|
| Incisional/surgical | Protect, immobilize edges, compress | Steri-Strips, low-adherent, semi-permeable film |
| Skin tears | Protect, immobilize edges | Antibacterial ointment + low-adherent |
| Partial-thickness (burns, donor sites) | Epithelialization, absorb exudate | Low-adherent foam/gauze, hydrocolloid |
| Full-thickness (pressure ulcers, dehiscence) | Maintain moisture, absorb, debride | Hydrogels, alginates, foam, V.A.C. |
| Heavily necrotic | Debridement | V.A.C., larval therapy dressing |
| Malignant wound | Odor control, moisture | Foam, metronidazole gel, activated charcoal |
| Venous ulcers | Graduated compression | Multi-layer (4-layer) compression system |
— Pfenninger & Fowler's Procedures for Primary Care, 3e, Table 44-5
5. Key Principles in Bandage Application
- Never apply too tightly: Circulatory compromise and compartment syndrome are serious risks — especially with circumferential casts and tubular gauze on digits.
- Protect intact skin: Adhesives cause maceration; use skin protectants (zinc oxide, A&E ointment) on skin chronically exposed to moisture or tape.
- Match dressing to wound stage: Wound character evolves — what is appropriate in the inflammatory phase differs from the granulation and epithelialization phases.
- Elevation: After dressing, elevate the injured extremity above heart level for the first 24 hours to reduce edema.
- Bandage contact lenses: A specialized application — soft therapeutic lenses used as bandages for corneal abrasions, providing pain relief and promoting epithelial healing.
— Roberts & Hedges' Clinical Procedures in Emergency Medicine; Tintinalli's Emergency Medicine
Quick Reference Summary
| Category | Examples |
|---|---|
| By material | Gauze, elastic, tubular, triangular, adhesive, cohesive |
| By function | Retention, compression (elastic/inelastic/multi-layer), immobilization, pressure, non-adherent |
| By construction | Impregnated, plain, self-adherent, film, foam, hydrocolloid, hydrogel, alginate |
| Specialty | V.A.C. (negative pressure), silver-containing, activated charcoal, bandage contact lens |
Short way in understanding content types of bandage in medical
Types of Bandages — Quick Reference
🔵 1. By MATERIAL
| Bandage | Key Point |
|---|---|
| Gauze | Most common, cheap, may stick to wound |
| Crepe | Elastic, conforms to body shape |
| Triangular | Cloth triangle → sling or head bandage |
| Tubular | Seamless sleeve for fingers/limbs |
| Adhesive (plaster) | Small pad + sticky strip, minor wounds |
| Cohesive (Coban) | Sticks to itself, not skin |
🟢 2. By FUNCTION
| Bandage | Does What? |
|---|---|
| Retention | Holds dressing in place |
| Compression | Squeezes to reduce swelling/venous disease |
| Immobilization | Limits movement (sling, figure-of-8) |
| Pressure | Stops bleeding |
| Non-adherent | Sits on wound without sticking |
🟡 3. Compression — The 3 Types
| Type | How it works | Used for |
|---|---|---|
| Elastic (long-stretch) | Pressure at rest + activity | Varicose veins |
| Inelastic (short-stretch) | Pressure only during movement | Arterial/mixed disease |
| Multi-layer (4-layer) | Multiple layers combined | Venous ulcers (gold standard) |
🔴 4. Advanced Wound Dressings
| Type | Think of it as... |
|---|---|
| Hydrocolloid | Absorbs fluid → forms protective gel |
| Hydrogel | Adds moisture to dry wounds |
| Foam | Soaks up heavy leakage |
| Alginate | Seaweed-based, hemostatic, for heavy wounds |
| Silver dressing | Kills bacteria (incl. MRSA) |
| V.A.C. (vacuum) | Suction that pulls wound edges together |
| Charcoal | Absorbs bad odor |
⚡ Memory Trick
"MFW — Material → Function → Wound type" Pick material first → decide its function → match it to the wound
🚨 3 Rules Never to Forget
- Never too tight → causes ischemia
- Moist environment heals faster than dry
- Change dressing type as the wound heals — one size does NOT fit all
8 marks answer
Types of Bandages — 8 Marks Answer
Definition
A bandage is a piece of material used to cover, protect, support, or compress a wound or injured body part to promote healing and prevent contamination.
Types of Bandages
1. Gauze Bandage
- Made of cotton + cellulose acetate
- Inexpensive, widely available
- Disadvantage: May adhere to wound; limited moisture retention
- Used as: retention layer, wound packing
- Can be impregnated with petrolatum (Vaseline gauze) or antimicrobials (povidone-iodine, silver) to reduce adherence
2. Roller Bandage
- Long strip wound into a roll
- Applied in overlapping turns around body part
- Subtypes:
- Cotton crepe — light compression, retention
- Elastic/stretch — conforms to body contours
- Cohesive (Coban) — self-adherent, no adhesive to skin
3. Triangular Bandage
- Large triangular cloth
- Used as arm sling, head bandage, or folded for splint padding
- Versatile, especially in first aid and emergency settings
4. Tubular Bandage
- Seamless tube applied over limbs or digits
- Used for retention and digit protection
- ⚠️ Must not exceed two layers on a finger — risk of ischemic injury
5. Adhesive Bandage (Plaster)
- Small absorbent pad on adhesive strip
- Used for minor wounds and abrasions
- Repeated use may cause skin tears or maceration
6. Compression Bandage
Most important type in vascular and wound management:
| Type | Pressure | Used For |
|---|---|---|
| Elastic (long-stretch) | At rest + during activity | Varicose veins |
| Inelastic (short-stretch) | Only during movement | Arterial/mixed disease |
| Multi-layer (4-layer) | Sustained, graduated | Venous ulcers (gold standard) |
7. Immobilization Bandage
- Sling-and-swathe — shoulder dislocation, humeral fractures
- Velpeau bandage — arm held in adduction + internal rotation
- Figure-of-eight — historically for clavicle fractures (no longer recommended)
8. Advanced/Specialty Dressings
| Type | Function |
|---|---|
| Hydrocolloid | Absorbs exudate, maintains moist healing |
| Hydrogel | Adds moisture to dry/necrotic wounds |
| Foam dressing | Heavy exudate absorption |
| Alginate | Seaweed-based, hemostatic, heavy wounds |
| Silver dressing | Broad-spectrum antibacterial (incl. MRSA) |
| V.A.C. dressing | Negative pressure — promotes granulation |
| Activated charcoal | Odor control in malignant wounds |
Dressing Selection by Wound Type
| Wound | Recommended Bandage |
|---|---|
| Surgical/incisional | Semi-permeable film, low-adherent |
| Partial thickness/burns | Foam + gauze, hydrocolloid |
| Full thickness/pressure ulcer | Hydrogel, alginate, V.A.C. |
| Infected wound | Silver dressing |
| Venous ulcer | 4-layer compression |
| Malignant/odorous | Charcoal dressing |
Key Principles (Important for Marks)
- Moist wound environment heals 30% faster than dry (George Winter, 1962)
- Never apply too tightly → risk of ischemia and compartment syndrome
- Change dressing type as wound progresses through healing stages
- Protect intact skin from adhesives → use zinc oxide or skin protectants
- Elevate limb for first 24 hours to reduce edema post-dressing
Conclusion
Bandages are classified by material, function, and wound type. Selecting the correct bandage requires assessment of wound depth, exudate level, infection status, and stage of healing. No single bandage suits all wounds — appropriate selection is essential for optimal healing outcomes.
surgical needle & needle holders, deep answer
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Now I have rich, authoritative content from multiple surgical textbooks plus excellent diagrams. Let me compile the deep answer.
Surgical Needles & Needle Holders — Deep Answer
PART 1: SURGICAL NEEDLES
Definition
A surgical needle is a stainless steel instrument used to carry suture material through tissue, enabling wound closure. It must be strong, sharp, and resistant to bending without being brittle.
"Inappropriate needle selection can damage the tissues, causing poor results and delayed healing." — Pfenninger & Fowler's Procedures for Primary Care, 3e
Anatomy of a Surgical Needle
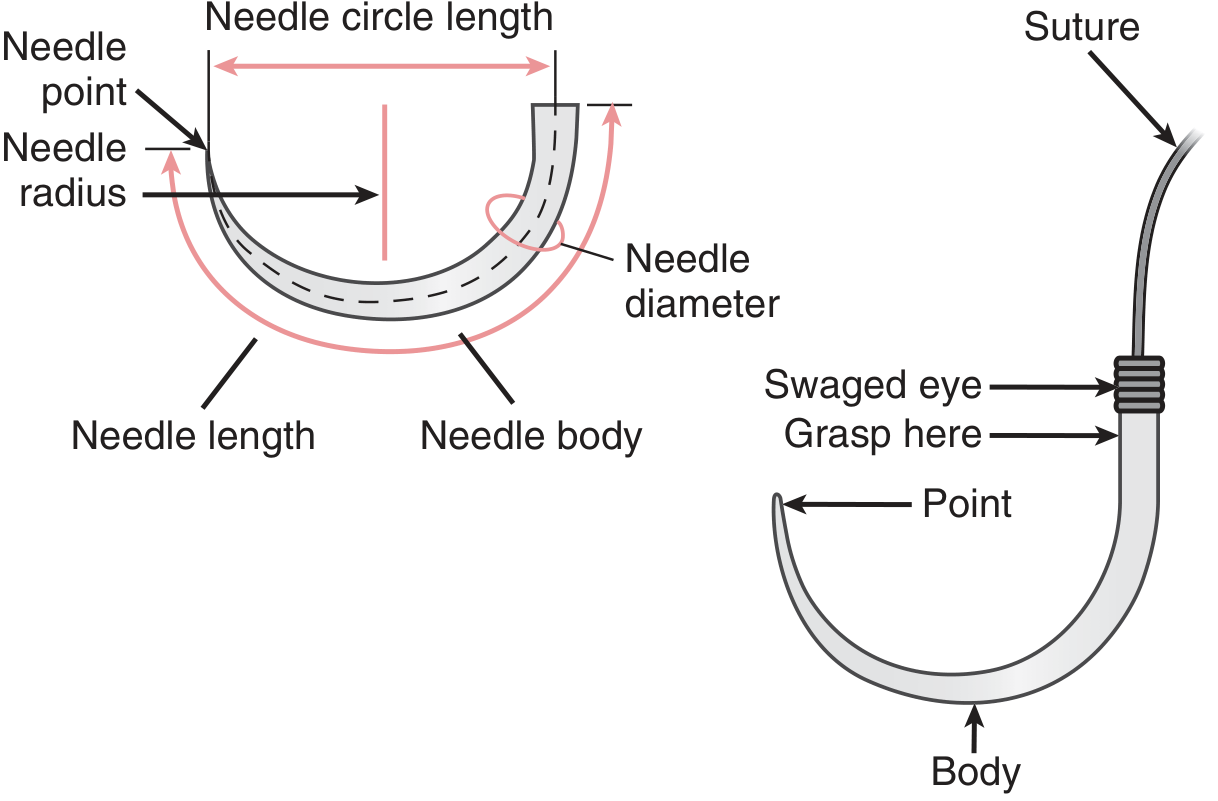
The needle has 3 parts:
| Part | Description |
|---|---|
| Point | Penetrates tissue; shape determines tissue trauma |
| Body | The shaft; grasped by needle holder; shape determines strength and resistance to rotation |
| Eye / Shank (Swage) | Where suture attaches |
Material: Most needles are made of non-corrosive stainless steel, heated to maximize strength and ductility (ability to bend under pressure without breaking). Coated with silicone to reduce friction during tissue passage.
1. Types of Eye (Suture Attachment)
| Type | How It Works | Advantage / Disadvantage |
|---|---|---|
| Closed Eye | Like a sewing needle; must be threaded | Causes double suture strand → more tissue damage |
| French (Split/Spring) Eye | Suture snapped in; spring-loaded | Still threaded; less common |
| Swaged (Atraumatic) ✅ | Suture molded/crimped directly into needle — no threading | Single strand → minimal tissue trauma; most widely used since the 1960s |
"Needles have been almost exclusively swaged because threaded needles have many undesirable characteristics." — Pfenninger & Fowler's, p. 200
2. Types by Needle Point
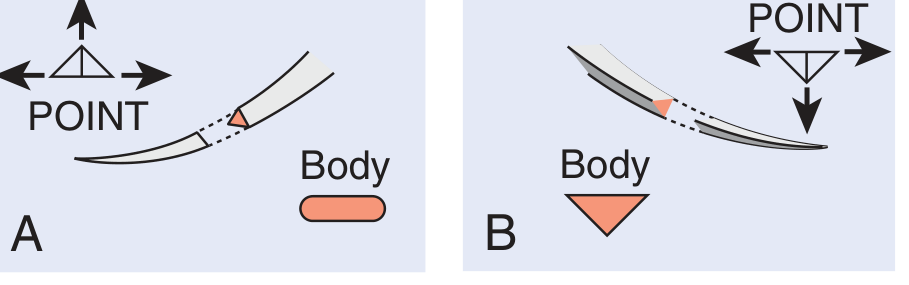
A. Cutting Needles — for tough, dense tissue
i. Conventional Cutting Needle
- Triangular cross-section
- Cutting edge on the inner (concave) curvature
- Force concentrates at the apex → tendency to cut/tear toward the wound edge
- Rarely used today due to this disadvantage
ii. Reverse Cutting Needle ✅ (Most common cutting type)
- Cutting edge on the outer (convex) curvature
- Flat inner surface distributes suture tension across the base → less risk of tissue tear
- Used for: skin, fascia, tendon sheaths
- Unless specified otherwise, "cutting needle" = reverse cutting
iii. Spatula Needle
- Flat on top and bottom, cutting side edges
- Used in: ophthalmic surgery — allows needle to travel in plane of tissue layers
B. Tapered (Round) Needles — for soft, delicate tissue
- Round/oval body, tapers to a sharp point without cutting edges
- Creates a small, clean hole by pushing tissue aside without cutting
- Used for: bowel, blood vessels, peritoneum, nerve repair
- A cutting needle would never be used in bowel anastomosis — risk of leakage
C. Blunt-Point Needles
- Round body, blunt tip that dissects without cutting
- Used for: friable parenchymal tissue — liver, kidney
- Also used in obstetrics to reduce needlestick injuries
3. Types by Body Shape (Curvature)
| Shape | Use |
|---|---|
| Straight | Accessible, superficial tissue; rarely used; finger is used as guide |
| 1/4 circle | Ophthalmic and microsurgery |
| 3/8 circle ✅ | Most common — skin closure, general surgery |
| 1/2 circle | Deep cavity work — abdomen, pelvis; requires restricted wrist movement |
| 5/8 circle | Very deep, confined spaces — urology, rectal surgery |
| Compound curve (J-shape) | Plastic surgery, narrow deep wounds |
"In general, a 3/8-inch curvature is adequate for most cutaneous procedures." — Pfenninger & Fowler's, p. 201
4. Needle Size Selection
- Larger needle → deeply buried sutures, thick tissue
- Smaller needle → thin skin layers, facial closures
- Facial closure: P-3 needle (precision cosmetic)
- Thick skin (trunk, extremities): FS-2, FS-3 needles (for skin)
5. Complications of Needles
| Complication | Cause |
|---|---|
| Needle bending | Needle too small for tissue resistance; wrong angle of penetration |
| Needle breakage | Unexpected bone/scar; reshaping a bent needle further weakens it |
| Lost needle | Grasping suture near shank weakens it → needle detaches |
| Needlestick injury | Free needle is a serious hazard to surgeon |
| Increased resistance | Multiple passes wear away silicone lubricant |
"When a needle bends during suturing, the act of straightening it further weakens the metal." — Pfenninger & Fowler's, p. 201
PART 2: NEEDLE HOLDERS
Definition
A needle holder is a scissor-like locking instrument used to grasp and drive a surgical needle through tissue. It provides controlled, precise needle passage and is the only acceptable instrument for this purpose.
"A hemostat or other grasping instrument is not an acceptable substitute for a needle holder when suturing. The needle will easily roll out of position because it requires a flat surface to maintain its operative position." — Pfenninger & Fowler's, p. 200
Anatomy
- Jaws — grasp the needle (serrated or smooth)
- Box joint — pivot mechanism
- Ratchet lock — locks jaws at required tension
- Ring handles — for finger placement and control
Types of Needle Holders
| Needle Holder | Jaw Type | Best Used For |
|---|---|---|
| Webster (4.5–5 inch) | Smooth or fine serrations, tapered tip | Fine needles (P-3), facial/hand surgery |
| Halsey | Smooth/delicately serrated, tapered | Fine sutures (6-0), facial surgery |
| Mayo-Hegar ✅ | Short serrated jaws, strong | Larger needles, trunk & extremity surgery |
| Baumgartner | Short tips, serrated jaws | Thicker skin, large procedures |
| Crile-Wood | Gently tapered blunt tip | Larger needles, skin surgery trunk/extremities |
| Olsen-Hegar | Serrated jaws + built-in scissors | Convenient for solo operator; risk of inadvertent suture cutting |
| Castroviejo | Spring-loaded, very fine | Ophthalmic/eyelid surgery, microsurgery |
Jaw Types Compared
| Jaw Type | Advantage | Disadvantage |
|---|---|---|
| Serrated | Prevents needle rotation/twisting with large needles | Can damage fine-caliber needles, tear fine sutures |
| Smooth | Gentle on fine needles and sutures (6-0) | Needle may slip if not grasped carefully |
| Tungsten carbide inserts (gold handles) ✅ | Hardest, strongest grip; 5-year guarantee | More expensive |
Correct Technique for Holding the Needle
- Grasp the needle at the junction of the posterior one-third and middle one-third of its body — one needle-holder's width past the curved center
- Never grasp the shank — it is the thinnest, weakest part and will bend
- Apply only one to two clicks of the ratchet — excessive pressure weakens the needle
- Advance force in the direction of the needle's curvature (pronate/supinate wrist)
- The tip of the needle holder should just cover the needle
"The needle should be grasped below the shank portion, but beyond the mid-body region. The tip of the needle holder should just cover the needle, and the handle should be closed only to the first or second ratchet." — Pfenninger & Fowler's, p. 200
Matching Needle Holder to Surgery Site
| Surgical Site | Needle Holder |
|---|---|
| Face / eyelid | Webster, Halsey, Castroviejo |
| Trunk / extremities | Mayo-Hegar, Baumgartner, Crile-Wood |
| Deep abdominal / pelvic | Long-handled heavy holders |
| Solo operator | Olsen-Hegar (with caution) |
| Microsurgery | Castroviejo (spring-loaded) |
Key Rules — Needle Holders
- Never use a hemostat as a substitute — needle rolls out of position
- Gold handles = tungsten carbide inserts = superior quality
- Serrated holders for large needles in thick skin; smooth holders for fine needles on face
- Do not use large needles with fine holders — damages the inserts
- Olsen-Hegar is convenient but easy to accidentally cut the suture when regripping
Summary Table
| Feature | Cutting Needle | Tapered Needle | Blunt Needle |
|---|---|---|---|
| Tip shape | Triangular | Round, tapers to point | Round, blunt |
| Mechanism | Cuts tissue | Pushes tissue aside | Dissects without cutting |
| Tissue | Skin, fascia | Bowel, vessels, nerves | Liver, kidney |
| Risk | Tissue tear (conventional) | Leakage if wrong type used | Pushes, doesn't cut |
Sources: Pfenninger & Fowler's Procedures for Primary Care, 3e | Roberts & Hedges' Clinical Procedures in Emergency Medicine | Dermatology 2-Volume Set 5e
This is a shared conversation. Sign in to Orris to start your own chat.