Sunderland classification
Reading File
search_medical_text
Sunderland classification peripheral nerve injury
search_medical_image
Sunderland nerve injury classification diagram
GradeResponse
GradeResponse
The retrieved text touched on Sunderland only briefly, so I'll supplement with comprehensive knowledge.
Sunderland Classification of Peripheral Nerve Injuries
The Sunderland classification (1951) is a five-degree system that expanded Seddon's three-category scheme (neurapraxia, axonotmesis, neurotmesis) by subdividing the middle category based on the layers of connective tissue damaged.
Anatomical Background
A peripheral nerve is organized into layers:
- Endoneurium — surrounds individual axons
- Perineurium — surrounds each fascicle
- Epineurium — surrounds the entire nerve trunk
The Five Degrees
| Degree | Seddon Equivalent | Structure Injured | Pathology | Recovery |
|---|---|---|---|---|
| 1st | Neurapraxia | Myelin only | Local conduction block; axon intact | Complete, weeks–3 months; no Wallerian degeneration |
| 2nd | Axonotmesis | Axon + myelin | Wallerian degeneration distal to lesion; endoneurial tubes intact | Complete; rate ~1 mm/day (proximal to distal) |
| 3rd | Axonotmesis | Axon + endoneurium | Wallerian degeneration; endoneurial tubes disrupted but perineurium intact | Incomplete; intraneural fibrosis leads to mixed/partial recovery |
| 4th | Axonotmesis | Axon + endoneurium + perineurium | Fascicular architecture lost; epineurium intact | Negligible spontaneous recovery; usually requires surgery |
| 5th | Neurotmesis | Complete nerve trunk | Full transection | No spontaneous recovery; requires surgical repair |
A 6th degree (Mackinnon, 1988) was later added to describe a mixed injury — different fascicles sustaining different degrees of injury within the same nerve trunk (common in complex trauma).
Key Points by Degree
1st Degree (Neurapraxia)
- Focal demyelination or conduction block without axonal disruption
- Common cause: compression (Saturday night palsy, tourniquet)
- EMG: reduced conduction velocity across the lesion; normal distal to it
- No denervation potentials on needle EMG
2nd Degree (Pure Axonotmesis)
- Axon is severed but the endoneurial tube acts as a guide rail
- Wallerian degeneration occurs distally
- Reinnervation is orderly and complete because axons regenerate down their original tubes
- Best prognosis among axon-disrupting injuries
3rd Degree
- Endoneurial tubes are disrupted by intraneural hemorrhage and fibrosis
- Regenerating axons may misdirect into wrong tubes (aberrant reinnervation)
- Recovery is variable and often incomplete
- EMG shows denervation + reinnervation over months
4th Degree
- Only the epineurium holds the nerve together as a cord
- The nerve in continuity is essentially a fibrous scar
- Clinically resembles complete transection
- Surgical neurolysis or nerve grafting is usually required
5th Degree (Neurotmesis)
- Complete anatomical disruption of the nerve
- Spontaneous recovery is impossible
- Management: primary neurorrhaphy (if tension-free) or nerve grafting (sural nerve most common)
Clinical Assessment Tools
| Tool | What It Shows |
|---|---|
| NCS/EMG | Differentiates 1st degree (conduction block) from axon loss; tracks reinnervation |
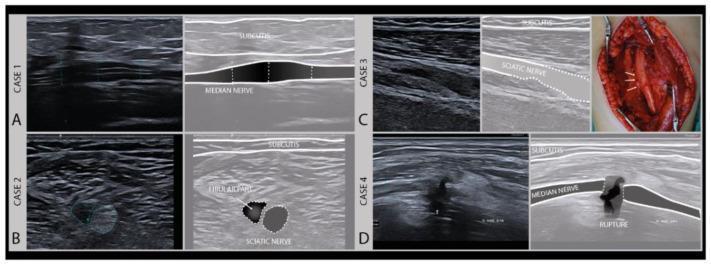
| High-resolution ultrasound | Fascicular integrity, swelling, neuroma-in-continuity (Sunderland Grades II–V visible as shown above) |
| MRI neurography | Wallerian degeneration, fascicular disruption, muscle denervation |
| Tinel's sign | Advancing Tinel's = regeneration occurring (positive in 2nd–3rd degree) |
Management Summary
| Degree | Initial Management | Surgical Indication |
|---|---|---|
| 1st | Conservative; splinting, PT | None |
| 2nd | Conservative; serial EMG | None |
| 3rd | Conservative 3–6 months; serial EMG + US | If no reinnervation by expected time |
| 4th | Early surgical exploration | Neurolysis ± grafting |
| 5th | Early surgical repair | Primary repair or nerve graft |
Prognosis Determinants
- Level of injury — more proximal = longer regeneration distance = worse motor recovery
- Age — younger patients regenerate more effectively
- Mechanism — crush/stretch injuries often higher degree than they appear clinically
- Time to repair — delays >6 months worsen motor end-plate viability
The Sunderland system remains the standard framework for surgical decision-making and prognosis in peripheral nerve trauma.
This is a shared conversation. Sign in to Orris to start your own chat.