How hernioplasty is done prodcedure surgery Bailey and love
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive material. Here is a thorough answer on hernioplasty procedure:
Note: Bailey & Love's Short Practice of Surgery is not available in this library's collection. The following is based on Schwartz's Principles of Surgery, 11th Edition — which covers the same material in equivalent or greater depth.
Hernioplasty — Surgical Procedure
Hernioplasty (tension-free prosthetic mesh repair) is the most commonly performed general surgical procedure worldwide. It fundamentally differs from older herniorrhaphy techniques by reinforcing the inguinal floor with a prosthetic mesh rather than approximating native tissues under tension.
Preoperative Setup
- Patient position: supine
- Anaesthesia: local, spinal, or general (open approach); general anaesthesia is mandatory for laparoscopic repair
- The inguinal region is prepared and draped
Open Approach
Step 1 — Incision & Exposure
- A skin incision is made 2 cm above and parallel to the inguinal ligament, from the pubic tubercle to the anterior superior iliac spine
- Subcutaneous fat is divided; Scarpa's fascia is incised to expose the external oblique aponeurosis (EOA)
- The EOA is incised along the direction of its fibres from the external ring, taking care to avoid the underlying ilioinguinal nerve
- The spermatic cord (or round ligament in females) is mobilised by blunt dissection and looped with a Penrose drain
Step 2 — Hernia Sac Identification & Management
- Indirect hernia sac: found anteromedially within the cord; dissected free from cord structures; reduced or transfixed and excised at the level of the internal ring
- Direct hernia sac: lies medial to the inferior epigastric vessels; the sac (transversalis fascia bulge) is reduced; no need for high ligation
The Lichtenstein Tension-Free Hernioplasty (Gold Standard Open Repair)
This is the technique described in Bailey and Love as the standard open mesh repair.
Steps:
-
Exposure: identical initial exposure as above — inguinal canal dissected to expose the shelving edge of the inguinal ligament, pubic tubercle, and Hesselbach's triangle
-
Mesh selection & sizing: A "flat-iron" shaped polypropylene mesh with a keyhole cut for cord egress is used. It must be large enough to extend 2–3 cm superior to Hesselbach's triangle
-
Medial fixation: The medial edge is affixed to the anterior rectus sheath, overlapping the pubic tubercle by 1.5–2 cm — this refinement minimises medial recurrence
-
Inferior fixation: A permanent, synthetic, monofilament suture (e.g., Prolene) fixes the inferior margin along the shelving edge of the inguinal ligament from medial to lateral, ending at the internal ring. Care is taken not to place sutures directly into the periosteum of the pubic tubercle
-
Superior fixation: The upper border of the mesh is fixed to the internal oblique aponeurosis and medial edge to the rectus sheath using a synthetic absorbable suture
-
Keyhole/internal ring: The lateral tails of the mesh are tailored to fit snugly around the spermatic cord at the internal ring (not tightly). The tails are sutured to the inguinal ligament and tucked beneath the EOA
-
Femoral hernia extension (if present): A triangular extension of the inferior mesh is sutured to Cooper's ligament medially and the inguinal ligament laterally
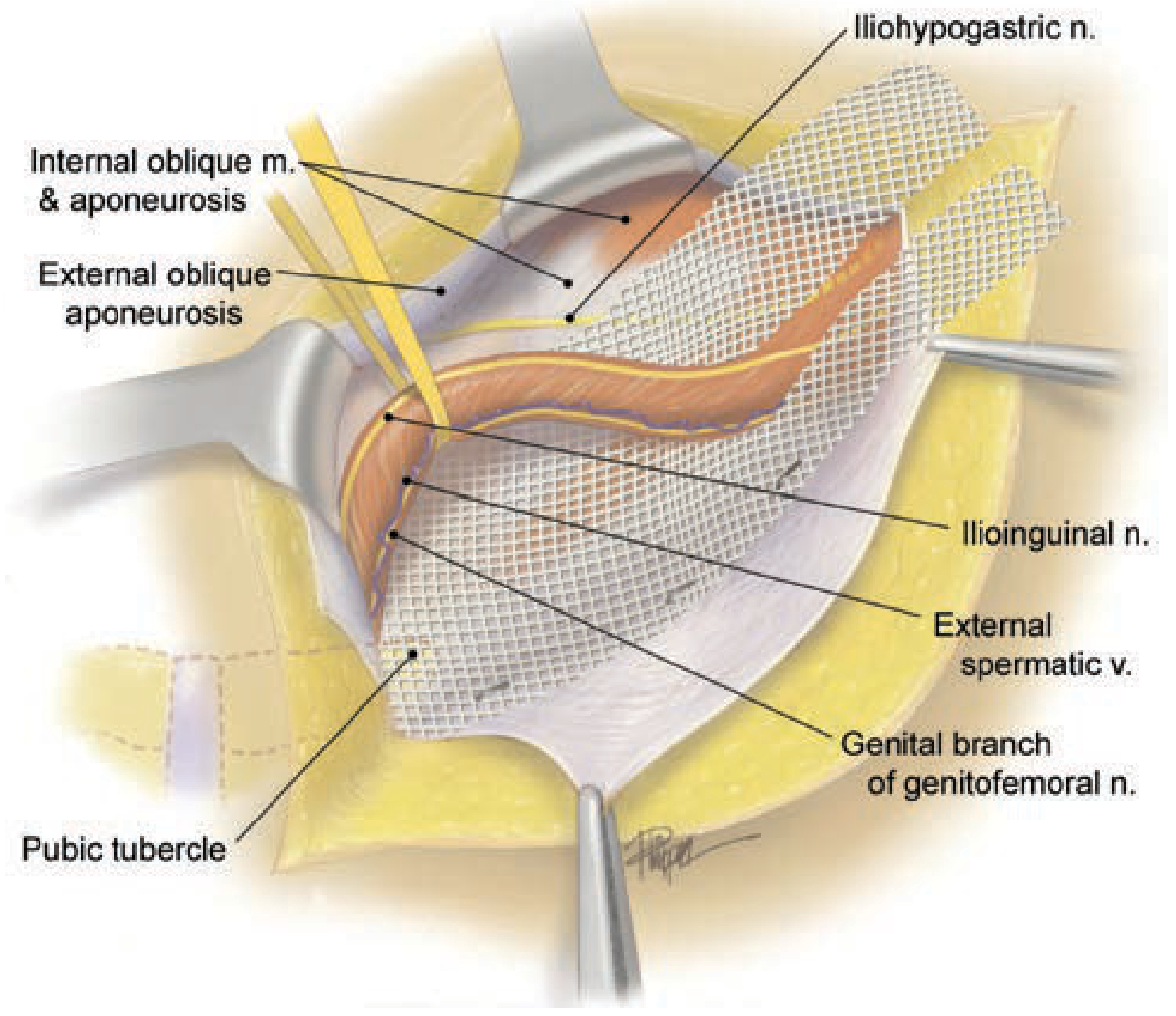
Lichtenstein tension-free hernioplasty — mesh in situ covering the inguinal floor
Step 3 — Wound Closure
- Cord contents are returned to anatomic position
- EOA is re-approximated continuously from medial to lateral with absorbable suture; external ring reconstructed snugly around the cord
- Scarpa's fascia and skin closed in layers
Plug and Patch Technique (Gilbert–Rutkow Modification)
A 3D prosthetic plug is inserted into the space previously occupied by the sac (through the internal ring for indirect; sutured to Cooper's ligament and inguinal ligament for direct), before laying the flat mesh patch over the inguinal floor. The plug is fixed to the internal ring margins with interrupted sutures.
Caution: isolated case series have reported plug migration causing bowel obstruction and chronic pain.
Laparoscopic Approaches
Two principal techniques are used:
1. Transabdominal Preperitoneal (TAPP)
- Pneumoperitoneum to 15 mmHg; patient in Trendelenburg
- Three ports: one umbilical (12 mm) + two lateral 5-mm ports
- Peritoneal incision made at the medial umbilical ligament, 3–4 cm superior to the defect, carried laterally to the ASIS
- Preperitoneal space developed; cord skeletonised; sac reduced
- Mesh 10 × 15 cm rolled and inserted through the 12-mm port; unrolled in the preperitoneal space
- Secured medially to Cooper's ligament with an endoscopic tacker; laterally toward the ASIS
- Peritoneum closed with a running suture or tacker
2. Totally Extraperitoneal (TEP)
- Avoids peritoneal entry entirely
- Preperitoneal space developed using a balloon dissector via infraumbilical incision
- CO₂ insufflation to 8–12 mmHg in the extraperitoneal space
- Two additional trocars inserted under direct vision
- Dissection, hernia reduction, and mesh placement identical to TAPP
- No peritoneal closure required
- Preferred for bilateral and recurrent hernias after prior open anterior repair (Grade A recommendation, IEHS guidelines)
Key Anatomical Landmarks to Protect
| Structure | Risk |
|---|---|
| Ilioinguinal nerve | Chronic groin pain if entrapped in sutures |
| Iliohypogastric nerve | Numbness/pain in suprapubic region |
| Genital branch of genitofemoral nerve | Pain/numbness in scrotum/labia |
| Femoral vessels | Avoid sutures into Cooper's ligament laterally |
| Vas deferens | Infertility if damaged |
| Inferior epigastric vessels | Haematoma if injured during laparoscopic port insertion |
Comparison of Techniques
| Feature | Lichtenstein | TEP/TAPP |
|---|---|---|
| Anaesthesia | Local/spinal/GA | GA mandatory |
| Recurrence | ~1–2% | ~1–2% (non-inferior) |
| Recovery | Slightly longer | Faster return to activity |
| Bilateral hernias | Two incisions needed | Single session |
| Recurrent hernia | Difficult (scarring) | Preferred approach |
| Learning curve | Short | Longer |
— Schwartz's Principles of Surgery, 11th Edition, Chapter 37 (Inguinal Hernia)
Lichenstein techniques
Reading File
Reading File
Loading Image
Loading Image
Here is a detailed, step-by-step account of the Lichtenstein Tension-Free Hernioplasty technique:
Lichtenstein Tension-Free Hernioplasty
Concept: Introduced by Irving Lichtenstein in 1989. The core principle is reinforcing the posterior wall of the inguinal canal (inguinal floor) with a flat polypropylene mesh placed without tension — eliminating the tension that caused high recurrence rates in older tissue repairs (Bassini, Shouldice).
Recurrence rate: ~1–2% (vs. 10–15% with tissue repairs)
Anaesthesia: Can be performed under local, spinal, or general anaesthesia — a major advantage over laparoscopic methods
Step-by-Step Technique
Step 1 — Incision
- A skin incision 2 cm above and parallel to the inguinal ligament, from just medial to the anterior superior iliac spine (ASIS) to the pubic tubercle
- Subcutaneous fat divided; Scarpa's fascia incised
Step 2 — Opening the Inguinal Canal
- The external oblique aponeurosis (EOA) is split along its fibres from the external ring toward the internal ring
- The ilioinguinal nerve is identified and carefully preserved just beneath the EOA
- The iliohypogastric nerve is identified running along the superior edge of the internal oblique
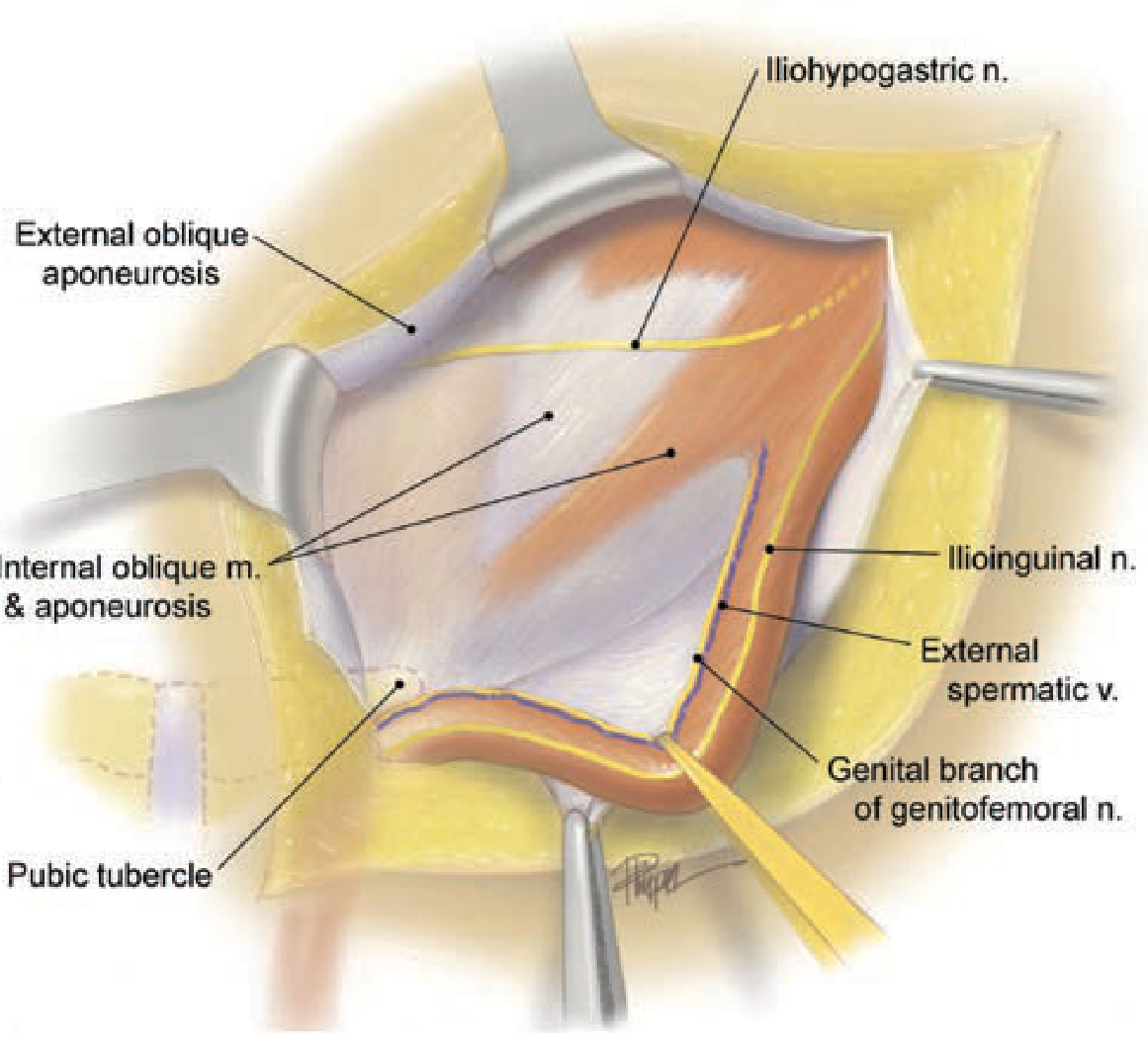
Anterior open exposure of the inguinal canal — key nerves and structures to protect
Step 3 — Cord Mobilisation
- The spermatic cord is mobilised from the floor of the inguinal canal using blunt and sharp dissection
- The cord is looped with a Penrose drain or finger
- The cremaster muscle fibres are divided to inspect for a hernia sac
Step 4 — Hernia Sac Handling
- Indirect sac: found anteromedially within the cord; dissected free from cord structures; reduced into the preperitoneal space or transfixed and excised at the internal ring
- If the sac extends into the scrotum, it is divided in the canal (not fully dissected) to avoid injury to testicular blood supply
- Direct sac: the transversalis fascia bulge is simply reduced — formal sac excision is not required
Step 5 — Mesh Preparation
- A flat, "flat-iron" shaped polypropylene mesh is used — pre-shaped with a keyhole slit at the lateral end for cord egress
- The mesh must be large enough to extend 2–3 cm superior to Hesselbach's triangle to cover the entire myopectineal orifice
Step 6 — Mesh Fixation (the critical step)
The mesh is laid flat over the posterior inguinal floor:
| Point of Fixation | Detail |
|---|---|
| Medial edge | Sutured to the anterior rectus sheath, overlapping the pubic tubercle by 1.5–2 cm — this prevents medial recurrence |
| Inferior border | Fixed with a permanent monofilament suture (e.g., 0-Prolene) along the shelving edge of the inguinal ligament, from medial to lateral, ending at the internal ring |
| Superior border | Fixed to the internal oblique aponeurosis and medial edge to the rectus sheath using synthetic absorbable suture |
| Lateral tails | Wrapped around the spermatic cord at the internal ring — tailored to fit snugly but not constrictingly — tails sutured to the inguinal ligament and tucked beneath the EOA |
Critical rule: Do NOT place sutures directly into the periosteum of the pubic tubercle — this causes severe chronic pain.
Lichtenstein hernioplasty — mesh in situ covering the inguinal floor; spermatic cord exits through keyhole
Step 7 — Femoral Hernia Modification (if present)
- A triangular extension of the inferior aspect of the mesh is created
- Sutured to Cooper's ligament medially and to the inguinal ligament laterally
- This closes the femoral ring from above
Step 8 — Wound Closure
- Cord contents returned to anatomic position in the inguinal canal
- EOA re-approximated continuously from medial to lateral with absorbable suture
- The external ring is reconstructed in close apposition to the spermatic cord — not too tight (causes strangulation), not too loose (appears as recurrence on exam)
- Scarpa's fascia closed with absorbable sutures
- Skin closed with subcuticular sutures or staples
Key Points to Remember
| Feature | Detail |
|---|---|
| Mesh material | Polypropylene (heavyweight or lightweight) |
| Mesh size | Must overlap pubic tubercle by ≥1.5–2 cm medially |
| Fixation suture, inferior | Permanent monofilament (Prolene) |
| Fixation suture, superior | Synthetic absorbable |
| Nerve at risk | Ilioinguinal, iliohypogastric, genitofemoral (genital branch) |
| Most important step | Medial overlap of pubic tubercle — prevents medial recurrence |
| Avoid | Sutures into pubic tubercle periosteum → chronic pain |
Advantages of Lichtenstein over Tissue Repairs
| Parameter | Lichtenstein | Bassini/Shouldice |
|---|---|---|
| Tension on suture line | None | Significant |
| Recurrence | ~1–2% | 10–15% |
| Anaesthesia | Local/spinal/GA | Local/spinal/GA |
| Chronic pain | Low (if nerves spared) | Higher |
| Day-case suitability | Yes | Yes |
— Schwartz's Principles of Surgery, 11th Edition, Chapter 37
This is a shared conversation. Sign in to Orris to start your own chat.