Bacterial corneal ulcers
Reading File
Finding Sources
Finding Sources
Searching PubMed
"bacterial keratitis" OR "bacterial corneal ulcer"
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive material from both Wills Eye Manual and Kanski's Clinical Ophthalmology to produce a detailed answer.
Bacterial Corneal Ulcers (Bacterial Keratitis)
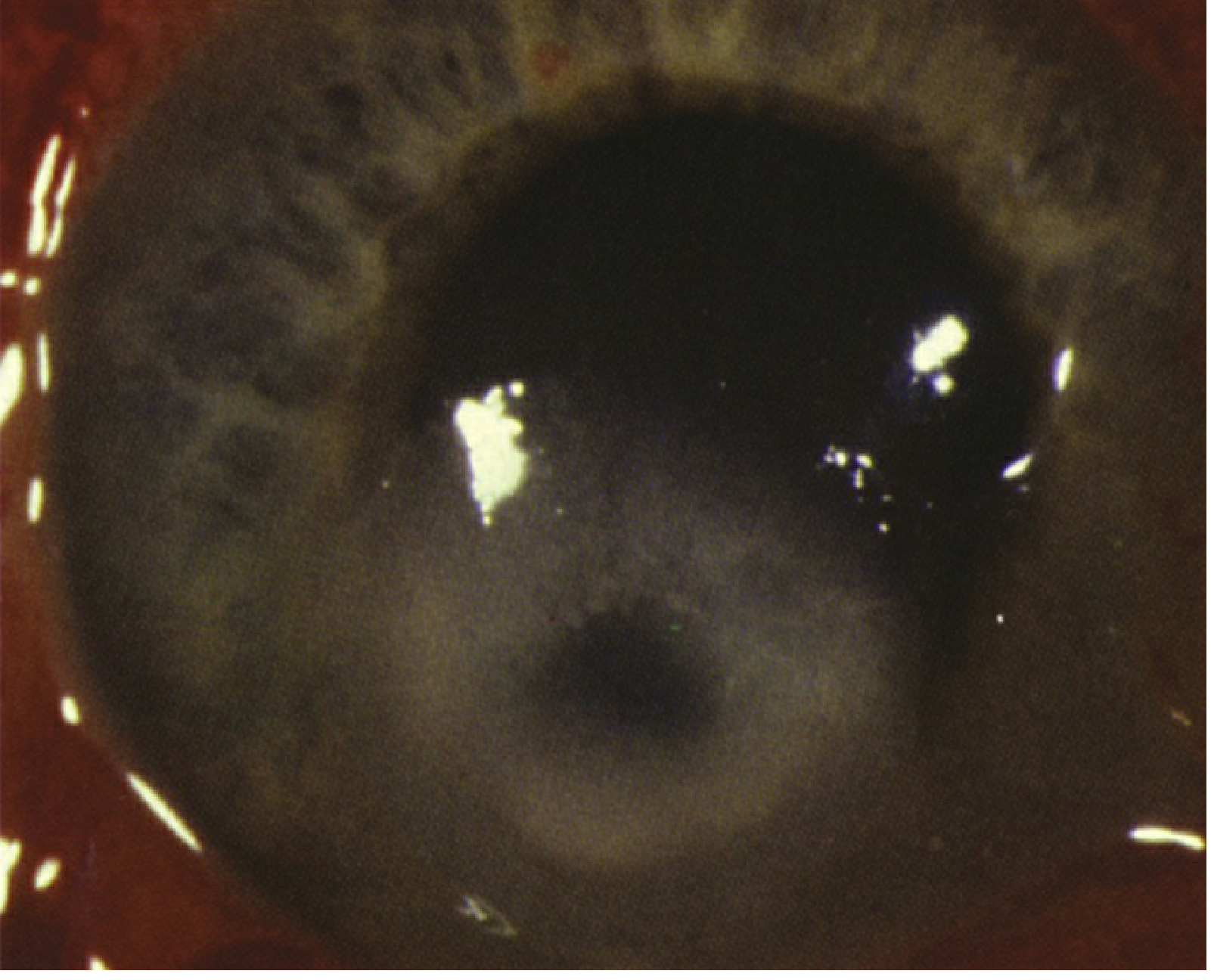
Bacterial keratitis with large central corneal infiltrate
Definition
Bacterial keratitis is an infection of the corneal stroma, typically presenting as a focal white stromal opacity (infiltrate) with an overlying epithelial defect - the corneal ulcer. An examiner using a slit beam cannot see clearly through an infiltrate or ulcer to the iris, distinguishing it from the more transparent picture of stromal edema or mild scars.
Causative Organisms
Most bacterial keratitis occurs when ocular defenses are compromised. Notable exceptions include Neisseria gonorrhoeae, N. meningitidis, Corynebacterium diphtheriae, and Haemophilus influenzae, which can penetrate an intact corneal epithelium (usually in the setting of severe conjunctivitis).
Common pathogens (Kanski's Clinical Ophthalmology, 10th ed.):
| Organism | Key Features |
|---|---|
| Pseudomonas aeruginosa | Gram-negative rod; >60% of contact lens-related keratitis; typically aggressive |
| Staphylococcus aureus | Gram-positive coagulase-positive; focal, fairly well-defined yellow-white infiltrate |
| Streptococcus pneumoniae | Gram-positive; upper respiratory tract commensal; often aggressive course |
| S. pyogenes | Gram-positive; often aggressive |
| Nocardia | Atypical; associated with prior eye surgery/trauma |
| Atypical mycobacteria | Associated with prior LASIK; indolent course |
Infections may be polymicrobial, including bacterial-fungal co-infection.
Risk Factors
- Contact lens wear - the most important risk factor, especially extended/overnight wear and soft lenses (higher risk than rigid gas-permeable); poor hygiene amplifies risk, but infections can occur even with daily disposables
- Trauma - including vegetable matter injury, corneal foreign body, prior refractive surgery (particularly LASIK - risk for atypical mycobacteria and interface keratitis)
- Ocular surface disease - dry eye, neurotrophic keratopathy, bullous keratopathy, prior herpetic keratitis
- Systemic immunocompromise - diabetes, immunosuppressive therapy
- Prior topical steroid use
Symptoms
- Red eye with moderate-to-severe ocular pain
- Photophobia
- Decreased/blurred vision
- Mucopurulent discharge
- Acute contact lens intolerance
Signs
Critical finding: Focal white opacity (infiltrate) in the corneal stroma with an overlying epithelial defect and underlying stromal thinning/tissue loss.
Other signs:
- Epithelial defect (fluorescein staining)
- Mucopurulent discharge
- Stromal edema and Descemet membrane folds
- Anterior chamber reaction - cells and flare
- Hypopyon - layered white cells in the anterior chamber (in the absence of perforation, usually represents sterile inflammation from toxin release)
- Conjunctival injection; upper lid edema
- Endothelial fibrin/cell deposition
- Severe cases: posterior synechiae, hyphema, raised IOP
Differential Diagnosis
| Condition | Distinguishing Features |
|---|---|
| Fungal keratitis | Feathery border, satellite lesions; history of vegetable trauma or contact lens wear |
| Acanthamoeba keratitis | Extremely painful; perineural infiltrate; ring infiltrate in late stages; contact lens wearer with water exposure |
| HSV stromal keratitis | Eyelid vesicles or corneal dendrites; history of recurrent unilateral disease |
| Non-infectious infiltrate | Small, peripheral, non-staining; in contact lens wearer; minimal pain; likely sterile |
| Marginal keratitis | Peripheral, separated from limbus by clear zone; associated with blepharitis/staphylococcal hypersensitivity |
Workup
- History: Contact lens type and hygiene, trauma, water exposure while lens-wearing, prior refractive surgery, systemic illness, prior antimicrobials or topical steroids
- Slit lamp exam: Fluorescein staining, document size/depth/location of infiltrate and epithelial defect, measure hypopyon, check IOP
- Corneal scrapings for Gram stain, KOH prep, cultures - indicated when:
- Infiltrate >1-2 mm in diameter
- Located in the visual axis
- Unresponsive to initial treatment
- Suspicion of atypical organism
- Culture contact lens and case if available (interpret carefully - contaminant vs. pathogen)
Treatment
All ulcers and infiltrates are initially treated as bacterial unless there is strong suspicion of another etiology. Initial therapy is broad spectrum.
Step 1 - Cycloplegia
Cyclopentolate 1% t.i.d. for comfort and to prevent posterior synechiae. Atropine 1% b.i.d.-t.i.d. preferred if hypopyon is present.
Step 2 - Topical Antibiotics (Risk-Stratified)
Low risk of visual loss (small, peripheral, non-staining infiltrate, minimal AC reaction):
- Non-contact lens wearer: Fluoroquinolone (moxifloxacin, gatifloxacin, besifloxacin, levofloxacin) or polymyxin B/trimethoprim q1-2h while awake
- Contact lens wearer: Fluoroquinolone q1-2h ± polymyxin B/trimethoprim q1-2h; can add tobramycin or ciprofloxacin ointment
Moderate/borderline risk (1-1.5 mm peripheral infiltrate, or any smaller infiltrate with epithelial defect or mild AC reaction):
- Fluoroquinolone q1-2h while awake; may add fortified tobramycin/gentamicin
High risk of visual loss (large, central, or aggressive infiltrate; significant AC reaction; hypopyon):
- Fluoroquinolone monotherapy (preferred agent: moxifloxacin - superior ocular penetration, broader Gram-positive coverage) q1h around the clock initially
- OR Fortified antibiotic duotherapy: cephalosporin (cefuroxime 5%) + aminoglycoside (fortified gentamicin 1.5%) alternating q30-60 min - preferred when Gram stain suggests streptococci or highly aggressive disease
Organism-Directed Treatment (Kanski's Table 7.4)
| Isolate | Preferred Agent | Concentration |
|---|---|---|
| Gram-positive cocci | Cefuroxime, vancomycin, or teicoplanin | 0.3%, 5%, 1% |
| Gram-negative rods | Fortified gentamicin, fluoroquinolone, or ceftazidime | 1.5%, varies, 5% |
| Gram-negative cocci | Ceftriaxone | 2% |
| Mycobacteria | Amikacin or clarithromycin | 2%, 1% |
| Nocardia | Amikacin or trimethoprim/sulfamethoxazole | 2% / 1.6%+8% |
| Atypical mycobacteria (post-LASIK) | Moxifloxacin + fortified amikacin ± clarithromycin (topical + oral) | - |
Note on ciprofloxacin: Associated with white corneal precipitates that may delay epithelial healing. Newer fluoroquinolones (moxifloxacin, gatifloxacin, besifloxacin) have better Gram-positive activity and address growing fluoroquinolone resistance (MRSA in USA; Pseudomonas in India).
Note on fortified antibiotics: High cost, limited availability, short shelf-life, refrigeration needed, contamination risk - must be specially prepared in a pharmaceutical dispensary.
Additional Measures
- Subconjunctival antibiotics - only if poor compliance with topical treatment
- No patching - ocular patches promote bacterial growth
- Discontinue contact lens use until fully resolved
- Treat elevated IOP if present
Follow-Up
- Daily evaluation initially: document infiltrate size, epithelial defect size, hypopyon level, and pain
- Reduced pain is often the first sign of positive response
- The epithelial defect may initially worsen after scraping - not necessarily a sign of failure
- Gradually taper antibiotic once improving, never below t.i.d.-q.i.d. (to prevent resistance emergence)
- If no response: repeat cultures, switch to fortified antibiotics, consider hospitalization
- Corneal biopsy if worsening despite negative cultures
- Corneal perforation: patch graft or penetrating keratoplasty; cyanoacrylate tissue glue may be used for small perforations once infection is controlled
Patients should be told to return immediately if: pain worsens, vision decreases, or the ulcer appears larger in the mirror.
Complications
- Corneal scarring and permanent vision loss
- Corneal thinning and perforation
- Endophthalmitis (rare)
- Secondary glaucoma
- Symblepharon/synechiae
Recent Evidence
Three recent high-quality studies are relevant:
- A Cochrane Network Meta-Analysis (Song et al., 2025 - PMID 40728038) on topical antibiotics for bacterial keratitis - most current comparative efficacy data
- A Lancet Microbe Systematic Review and Meta-Analysis (Tuft et al., 2026 - PMID 42229497) on regional and temporal antimicrobial resistance trends among bacterial keratitis isolates - clinically relevant given rising fluoroquinolone resistance in some regions
- An umbrella review on corneal cross-linking for infectious keratitis (Farhadi et al., 2025 - PMID 40269767) as adjunctive therapy
Sources: The Wills Eye Manual, 8th ed. §4.11; Kanski's Clinical Ophthalmology, 10th ed. §7 (Bacterial Keratitis, pp. 211-217)
This is a shared conversation. Sign in to Orris to start your own chat.