Basics of surgery
Reading File
Asking for Preferences
Finding Sources
Searching the Web
basics of surgery medical student overview wounds healing asepsis pre-op post-op
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have excellent material from multiple authoritative surgical textbooks. Let me compile the comprehensive answer.
Basics of Surgery - Medical Student Overview
Sources: Bailey and Love's Short Practice of Surgery (28th ed.), Schwartz's Principles of Surgery (11th ed.), Mulholland & Greenfield's Surgery (7th ed.), Pye's Surgical Handicraft (22nd ed.)
1. Surgical Terminology & Wound Classification
Wounds are classified by mechanism and contamination level:
| Class | Description | Infection Risk |
|---|---|---|
| Clean (Class I) | Elective, no GI/GU/respiratory entry, no break in technique | <2% |
| Clean-contaminated (Class II) | GI/GU/respiratory entry under controlled conditions | 5-10% |
| Contaminated (Class III) | Open fresh traumatic wound, major break in technique | 15-20% |
| Dirty/Infected (Class IV) | Old traumatic wound, perforated viscus, pus encountered | >30% |
Intention of healing:
- Primary intention (1st intention): Wound edges are approximated immediately (e.g., surgical incision closed with sutures). Clean wounds with no tissue loss. Best cosmetic outcome.
- Secondary intention (2nd intention): Wound left open, heals by granulation tissue formation from the base upward. Used for infected or heavily contaminated wounds.
- Tertiary / Delayed primary intention: Wound left open initially, then closed 4-5 days later after infection risk decreases (e.g., perforated bowel repair).
2. Phases of Wound Healing
Wound healing is a dynamic, overlapping four-phase process spanning up to 1 year:
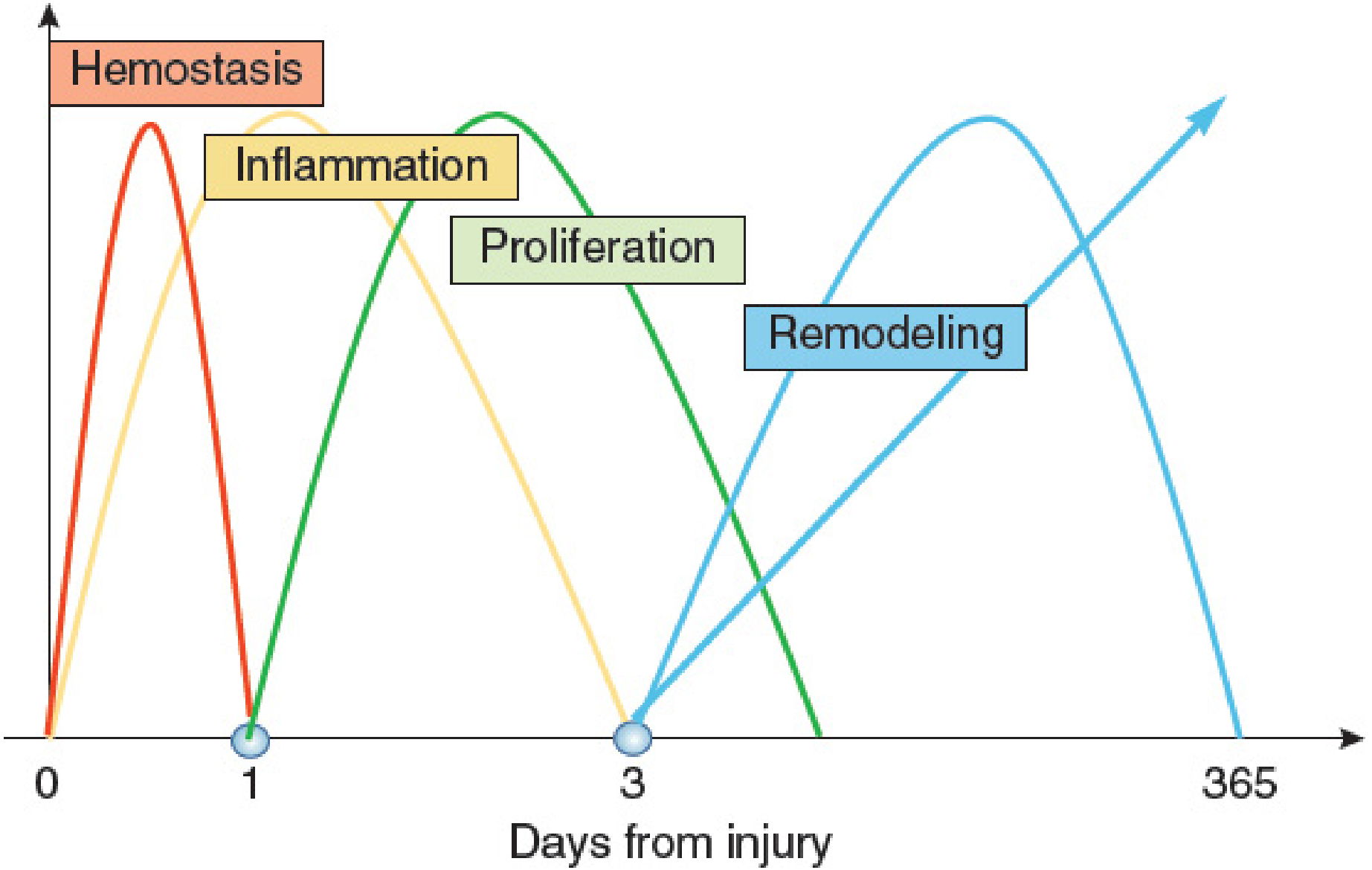
Figure: Four overlapping phases of wound healing (Mulholland & Greenfield's Surgery, 7th ed.)
Phase 1 - Hemostasis (minutes to hours)
- Injured vessels constrict; platelets adhere to exposed collagen via GP Ia/IIa complex
- Platelet aggregation forms a primary platelet plug; coagulation cascade activates -> fibrin clot
- Platelets release PDGF, TGF-β, VEGF - signaling molecules that drive subsequent healing
- The fibrin clot serves as a scaffold for migrating inflammatory cells
Phase 2 - Inflammation (days 1-4)
- PMNs (neutrophils) are the first cells recruited, peaking at 24-48 hours; they phagocytose bacteria/debris and release cytokines (TNF-α, IL-1)
- Macrophages (from monocytes) dominate by 48-96 hours - they are essential to healing; they release TGF-β, VEGF, IGF, EGF to regulate proliferation, matrix synthesis, and angiogenesis
- T-lymphocytes peak at ~1 week; CD8+ suppressor cells downregulate healing (their depletion enhances healing), while CD4+ helpers have minimal direct effect
- Clinical signs: redness, warmth, swelling, pain around wound
Phase 3 - Proliferation (days 4-12)
- Fibroblasts migrate in (chemotaxis by PDGF) -> proliferate -> synthesize collagen (types I and III) and extracellular matrix
- Lactate accumulation (~10 mmol) in the wound potently regulates collagen synthesis via ADP-ribosylation
- Angiogenesis: endothelial cells form new capillaries under VEGF, TNF-α, TGF-β stimulation
- Re-epithelialization: keratinocytes migrate from wound edges and skin appendages
- Wound contraction occurs via myofibroblasts (transformed fibroblasts)
Phase 4 - Maturation & Remodeling (weeks to 1 year)
- Collagen remodels: type III collagen is replaced by stronger type I collagen
- Collagen cross-linking increases wound tensile strength
- Maximum wound tensile strength = 80% of unwounded skin (never reaches 100%)
- Excess collagen deposition -> hypertrophic scar (stays within wound margins) or keloid (extends beyond wound margins, more common in dark skin, deltoid/presternal regions)
Factors impairing wound healing:
- Local: infection, foreign body, ischemia, radiation, poor technique
- Systemic: diabetes, malnutrition (esp. Vitamin C, zinc), corticosteroids, chemotherapy, jaundice, uremia, advanced age
3. Surgical Asepsis & Infection Prevention
Key concepts:
| Term | Definition |
|---|---|
| Asepsis | Absence of pathogenic organisms in a field |
| Antisepsis | Use of chemical agents on living tissue to destroy/inhibit organisms |
| Sterilization | Complete destruction of ALL microorganisms (including spores) |
| Disinfection | Destruction of most pathogens (not necessarily spores) |
Methods of sterilization:
- Autoclaving (steam under pressure): 134°C for 3 min or 121°C for 15 min - gold standard for heat-stable instruments
- Dry heat: 160°C for 60 min - for heat-stable items damaged by moisture
- Ethylene oxide gas: For heat-sensitive instruments (scopes, plastics)
- Gamma irradiation: Industrial sterilization of single-use items
Surgical scrub technique: 3-5 minute scrub with antiseptic (chlorhexidine or povidone-iodine) from fingertips to elbows, followed by gowning and gloving in a sterile manner.
Surgical site infection (SSI) prevention:
- Prophylactic antibiotics given within 60 minutes before incision (30 min for vancomycin)
- Hair removal with clippers (not razor shaving) if needed
- Maintain normothermia, normoglycemia intraoperatively
- Gentle tissue handling; avoid dead space and haematomas
4. Preoperative Assessment & Preparation
History: full surgical, medical, drug, allergy, family, and social history. Focus on cardiovascular, respiratory, renal, hepatic, and haematological status.
Examination: general, cardiorespiratory, and system-specific exam.
Investigations (tailored by risk):
| Investigation | Indication |
|---|---|
| FBC | All major surgery |
| U&E, Creatinine | Renal disease, diuretics, ACEi/ARB use, major surgery |
| LFTs, Coagulation | Liver disease, jaundice, anticoagulation |
| ECG | Age >40, cardiac disease |
| Chest X-ray | Cardiorespiratory symptoms, major thoracic surgery |
| Pulmonary function tests (FEV1, FVC, PFR) | COPD, respiratory disease |
| Group & Save / Crossmatch | Any surgery with blood loss risk |
Optimisation before elective surgery (Pye's Surgical Handicraft):
- Treat respiratory infections; avoid elective surgery during acute illness
- Stop smoking 3 weeks preoperatively to reduce bronchial hypersecretion
- Carious teeth removed 3 weeks before (risk of lung abscess from dental sepsis)
- Obese patients encouraged to diet/lose weight before elective surgery
- Physiotherapy teaching of breathing exercises preoperatively
Fasting (NBM): "2-4-6 rule"
- Clear fluids: 2 hours before
- Breast milk: 4 hours before
- Solids/formula/cow's milk: 6 hours before
Consent: informed, voluntary, and patient must have capacity. Covers procedure, alternatives, material risks, and expected outcomes.
5. Surgical Instruments & Sutures
Suture Classification
Absorbable sutures (for deep tissues, subcutaneous layers):
- Natural: Plain catgut (absorbed in 7-10 days), Chromic catgut (absorbed in 21 days)
- Synthetic: Vicryl (polyglactin), Dexon (polyglycolic acid), PDS (polydioxanone) - longer absorption, less tissue reaction, preferred
Non-absorbable sutures (for skin and permanent repairs):
- Braided (silk, braided nylon): easier to handle and knot, tension adjustable - but cause drag and may cause stitch abscess via capillary action
- Monofilament (nylon, polypropylene/Prolene): less tissue reaction, less drag - but harder to knot and tension harder to adjust
Needles:
- Cutting needles - for skin
- Round-bodied needles - for bowel, muscle, deep layers
- Fine slim-line cutting needles for facial work (4/0 suture)
- 3/0 gauge on stout cutting needle for most minor surgical procedures
Other wound closure methods:
- Staples: Fast; avoid on face and hands
- Adhesive strips (Steri-strips): Painless; useful for small superficial lacerations
- Tissue glue (cyanoacrylate): Clean lacerations with good apposition
Basic Instruments
- Needle holder (e.g., Gillies combined needle holder/scissors)
- Retractors: Catspaw retractors, skin hooks
- Haemostatic forceps: Mosquito/artery forceps
- Scissors: Mayo scissors (curved), Metzenbaum scissors (tissue dissection)
- For abscesses: Sinus forceps, Volkmann spoon
Drains
Used to prevent accumulation of blood, pus, bile, or serous fluid:
- Corrugated (open) drains - passive, drain by gravity
- Closed suction drains (Redivac, Jackson-Pratt) - fine perforated plastic tubes connected to negative-pressure reservoir; reduce infection risk
6. Postoperative Care & Complications
Immediate (0-24 hours)
- Airway: Ensure muscle relaxants fully reversed; suction upper airways clear before extubation
- Oxygen: Give routinely after major surgery to counteract arterial desaturation
- Analgesia: Adequate pain control enables deep breathing; narcotics given judiciously (respiratory depression risk)
- "Stir-up" regime: Patient encouraged to breathe deeply, cough, and move every hour
Common Postoperative Complications by Timing
| Time | Complication |
|---|---|
| 0-24 hrs | Reactionary haemorrhage, airway obstruction, hypotension, pain |
| 24-72 hrs | Secondary haemorrhage, wound infection starts, pulmonary atelectasis |
| Day 3-5 | Pulmonary complications (pneumonia, PE), UTI |
| Day 5-10 | Wound dehiscence, anastomotic leak, deep vein thrombosis |
| >10 days | Chronic wound infection, incisional hernia (months later) |
"The 4 Ws" of Postoperative Fever (mnemonic)
- Wind (day 1-2): Atelectasis/pneumonia
- Water (day 3-5): UTI
- Wound (day 5-7): Surgical site infection
- Walking (day 5+): DVT/PE
DVT/PE Prevention
- Early mobilisation
- TED stockings
- LMWH (low molecular weight heparin) prophylaxis
- Hydration
7. Shock in Surgical Practice
Shock = inadequate tissue perfusion. Classification critical for exams:
| Type | Mechanism | Example |
|---|---|---|
| Hypovolaemic | Low circulating volume | Haemorrhage, burns, GI losses |
| Distributive | Maldistribution of flow | Septic, anaphylactic, neurogenic |
| Cardiogenic | Pump failure | MI, cardiac tamponade |
| Obstructive | Outflow obstruction | Tension pneumothorax, PE |
Haemorrhagic shock classes (ATLS):
| Class | Blood loss | HR | BP | RR |
|---|---|---|---|---|
| I | <750 mL (<15%) | <100 | Normal | 14-20 |
| II | 750-1500 mL (15-30%) | 100-120 | Normal | 20-30 |
| III | 1500-2000 mL (30-40%) | 120-140 | Decreased | 30-40 |
| IV | >2000 mL (>40%) | >140 | Very low | >35 |
Management: 2 large-bore IV cannulae, crystalloid/blood resuscitation, treat source.
8. Surgical Anatomy Principles
Key concepts tested in exams:
- Langer's lines (relaxed skin tension lines): Incisions made along these lines produce least tension and best scars
- Anatomical planes: Surgeons work in tissue planes (e.g., fascial planes) to minimize blood loss and identify structures
- Surgical triangles & landmarks: e.g., Triangle of Calot (cystic artery, cystic duct, hepatic duct), Hesselbach's triangle (inguinal hernias)
- Nerve identification: Preserving motor/sensory nerves (e.g., facial nerve in parotid surgery, recurrent laryngeal nerve in thyroid surgery)
Quick Exam Summary
| Topic | High-Yield Points |
|---|---|
| Wound healing phases | Hemostasis -> Inflammation -> Proliferation -> Remodeling |
| Key cells | PMNs first (24-48h), Macrophages essential (48-96h), Fibroblasts in proliferation |
| Max wound strength | 80% of original (never 100%) |
| Keloid vs hypertrophic | Keloid extends beyond wound margins; hypertrophic does not |
| Sterilization | Autoclave = gold standard (134°C, 3 min) |
| Prophylactic antibiotics | Within 60 min before incision |
| Absorbable sutures | Vicryl, PDS, catgut (deep layers) |
| Shock classes | Class III (30-40% blood loss) = first drop in BP |
| Post-op fever | Wind-Water-Wound-Walking mnemonic |
Sources: Bailey and Love's Short Practice of Surgery (28th ed.); Schwartz's Principles of Surgery (11th ed.); Mulholland & Greenfield's Surgery (7th ed.); Pye's Surgical Handicraft (22nd ed.)
This is a shared conversation. Sign in to Orris to start your own chat.