Conjunctivitis
Reading File
Finding Sources
Searching Images
conjunctivitis types bacterial viral allergic
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Here is a comprehensive overview of conjunctivitis:
Conjunctivitis
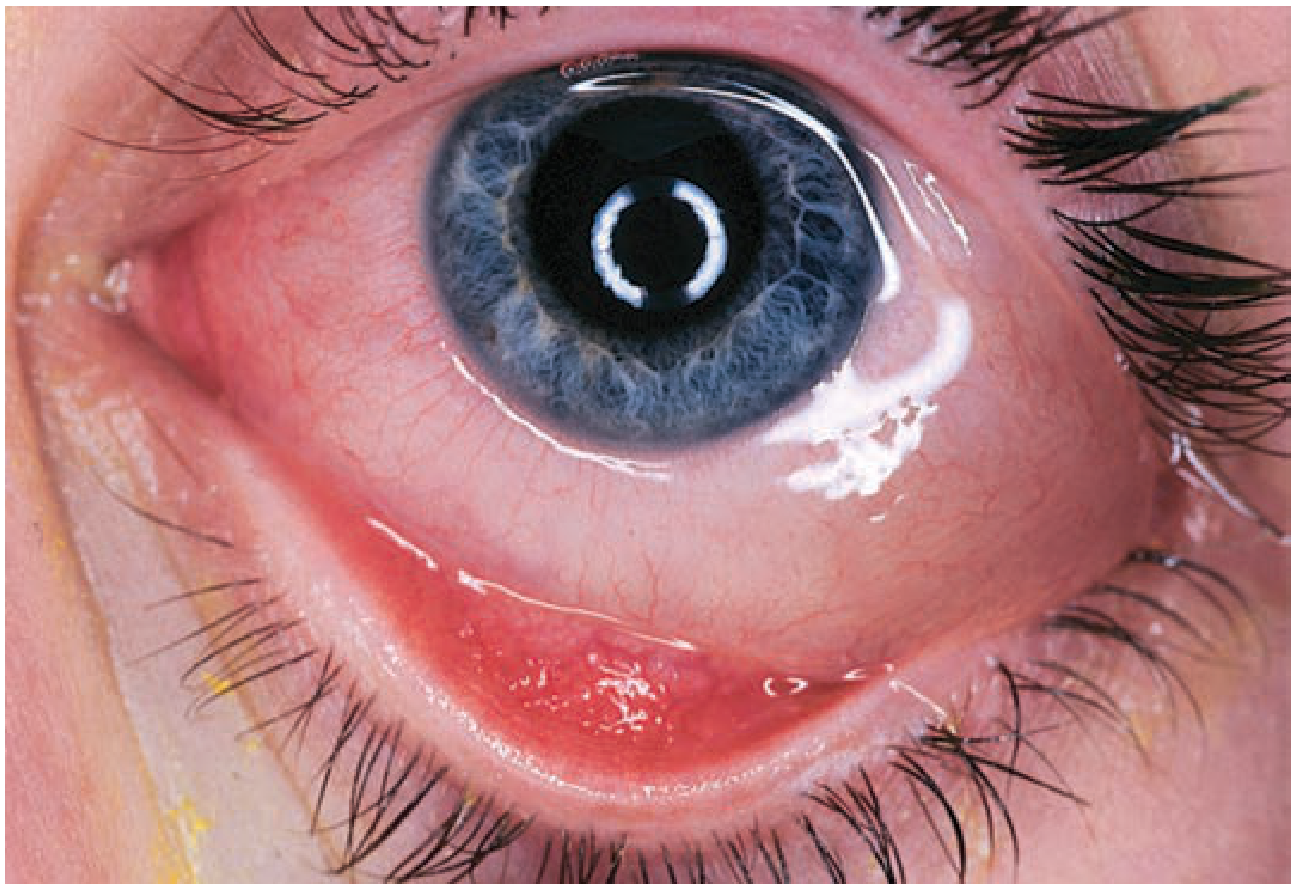
Conjunctivitis is inflammation of the conjunctiva and is one of the most common causes of the red eye. It is most often viral in etiology and typically self-limited, but certain forms (gonococcal, herpetic) can threaten vision if not treated aggressively.
Etiology
| Category | Common Causes |
|---|---|
| Viral | Adenovirus (most common), HSV, enterovirus |
| Bacterial | Staphylococcus, Streptococcus, H. influenzae, N. gonorrhoeae, Chlamydia |
| Allergic | Seasonal/perennial allergens, atopic keratoconjunctivitis |
| Other | Toxic/chemical irritation, parasitic, fungal |
Keratoconjunctivitis = conjunctivitis with corneal involvement (punctate ulcerations).
1. Bacterial Conjunctivitis
Clinical features:
- Painless mucopurulent discharge — hallmark finding
- Eyelids stuck together on awakening
- Unilateral or bilateral conjunctival injection
- Clear cornea (no fluorescein uptake unless abrasion/ulcer)
- Chemosis (conjunctival edema) common
- Preauricular lymphadenopathy usually absent (except in gonococcal)

Typical pathogens: Staphylococcus spp., Streptococcus spp., H. influenzae
Treatment:
- Cases are often self-limited; antibiotics shorten the course
- Trimethoprim–polymyxin B — first-line (avoids sulfa/neomycin allergy risk)
- Fluoroquinolone (besifloxacin, moxifloxacin, levofloxacin) or tobramycin — for contact lens wearers (cover Pseudomonas)
- Avoid gentamicin ophthalmic (high ocular irritation)
- Always perform fluorescein stain of the cornea (especially in infants) to exclude corneal abrasion, ulcer, or herpetic dendrite
Special cases:
- Gonococcal conjunctivitis — hyperacute, copious purulent discharge, preauricular LAD; cause of ophthalmia neonatorum; requires urgent systemic treatment
- Chlamydial conjunctivitis — chronic follicular conjunctivitis; also causes neonatal disease
2. Viral Conjunctivitis
Clinical features:
- Often preceded by upper respiratory infection
- Watery discharge (not purulent)
- Mild to moderate "red eye," no eye pain unless keratitis present
- Starts unilateral, second eye involved within days
- Preauricular lymphadenopathy — characteristic (distinguishes from bacterial)
- Slit lamp: follicles on inferior palpebral conjunctiva
- Occasional small subconjunctival hemorrhages

Epidemic Keratoconjunctivitis (EKC):
- Caused by adenovirus (types 8, 19, 37 — Group D HAdV)
- More severe; may be preceded by fever, myalgias, malaise
- Highly contagious; tends to occur in epidemics
- Fluorescein stain shows punctate keratitis
- Common findings: conjunctival injection (91%), tearing (80%), follicular reaction (76%), petechiae (70%), foreign body sensation (67%)
Treatment:
- Supportive: cool compresses, artificial tears (5–6×/day)
- Ocular decongestants (e.g., Naphcon-A, 1 drop TID PRN)
- Course: 1–3 weeks
- Highly contagious: frequent handwashing, separate towels, disinfect slit lamp/exam chair
- Always examine the cornea with fluorescein to exclude herpetic dendrite
3. Allergic Conjunctivitis
Clinical features:
- Itching — dominant symptom (distinguishes from bacterial/viral)
- Watery discharge, redness
- Erythematous, swollen eyelids
- Conjunctival injection with papillae (irregular mounds with central vascular tuft) on inferior fornix
- Prominent chemosis may be present
Treatment (stepped by severity):
| Severity | Treatment |
|---|---|
| Mild | Artificial tears alone; identify/eliminate allergen |
| Moderate | Topical antihistamine/decongestant, mast cell stabilizers, or NSAIDs; cool compresses QID |
| Severe | Topical steroids (consult ophthalmologist first — occult herpetic infection must be excluded) |
Key Differentiating Features
| Feature | Bacterial | Viral | Allergic |
|---|---|---|---|
| Discharge | Mucopurulent | Watery | Watery |
| Itching | Absent | Absent/mild | Dominant |
| Preauricular LAD | Absent (except GC) | Present | Absent |
| Eyelids stuck | Yes (morning) | No | No |
| Conjunctival reaction | Papillae | Follicles | Papillae |
| Cornea | Clear | ± Punctate keratitis | Clear |
| Bilaterality | Can be bilateral | Starts unilateral | Bilateral |
When to Refer Urgently
- Suspected gonococcal infection (hyperacute, copious discharge)
- Corneal involvement (reduced VA, fluorescein uptake, herpetic dendrite)
- Neonatal conjunctivitis (ophthalmia neonatorum)
- Failure to improve or diagnosis uncertain after initial assessment
— Tintinalli's Emergency Medicine, p. 1582–1583
This is a shared conversation. Sign in to Orris to start your own chat.