Give me relevant things for ent viva of MANDIBLE
Reading File
Finding Sources
Finding Sources
Searching Images
mandible anatomy ENT fracture sites
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a comprehensive ENT viva guide on the Mandible, organized by key topics:
MANDIBLE — ENT Viva Guide
1. ANATOMY OF THE MANDIBLE
Parts
The mandible consists of:
- Body (horizontal part) — divided into the base (lower) and alveolar part (upper, tooth-bearing)
- Ramus (vertical part, bilateral) — meets the body at the angle of the mandible
Key Landmarks on the Body
- Mental protuberance — midline swelling on the anterior surface
- Mental tubercles — lateral to the protuberance
- Mental foramen — midway between upper and lower borders of the body; transmits the mental nerve and vessels (branch of inferior alveolar nerve)
- Oblique line — ridge from the anterior border of the ramus onto the body; site of attachment for muscles that depress the lower lip
Key Landmarks on the Ramus
| Feature | Detail |
|---|---|
| Coronoid process | Triangular; attachment for temporalis muscle |
| Condylar process | Head (forms TMJ) + Neck (has pterygoid fovea for lateral pterygoid) |
| Mandibular notch (sigmoid notch) | Between coronoid and condylar processes |
| Mandibular foramen | On medial surface of ramus; entry of inferior alveolar nerve + vessels |
| Lingula | Just anterosuperior to mandibular foramen; attachment of sphenomandibular ligament |
| Mylohyoid groove | Below mandibular foramen; carries the nerve to mylohyoid |
| Medial surface, posteroinferior | Roughened for medial pterygoid muscle attachment |
| Lateral surface | Smooth; mostly for masseter muscle attachment |
— Gray's Anatomy for Students, p. 1114
2. MUSCLES OF MASTICATION (Mandibular Attachments)
| Muscle | Attachment on Mandible | Action | Nerve |
|---|---|---|---|
| Masseter | Lateral surface of ramus | Elevation | Masseteric n. (V3) |
| Temporalis | Coronoid process + anterior margin of ramus | Elevation + Retraction | Deep temporal nn. (V3) |
| Medial pterygoid | Medial surface near the angle | Elevation + side-to-side | Nerve to medial pterygoid (V3) |
| Lateral pterygoid | Pterygoid fovea on neck of condyle | Protrusion + depression + side-to-side | Nerve to lateral pterygoid (V3) |
Depression of the mandible: digastric, geniohyoid, mylohyoid (all V3/ansa cervicalis) + lateral pterygoid + gravity
— Gray's Anatomy for Students, p. 1116
3. TEMPOROMANDIBULAR JOINT (TMJ)
- Type: Synovial joint
- Articular surfaces: Head of mandible ↔ Articular fossa + articular tubercle of the temporal bone
- Articular surface covering: Fibrocartilage (not hyaline — unique feature, commonly asked!)
- Articular disc: Divides the joint into upper (gliding) and lower (hinge) compartments
- Ligaments:
- Lateral (temporomandibular) ligament — main ligament
- Sphenomandibular ligament — sphenoid spine → lingula
- Stylomandibular ligament — styloid process → angle of mandible
Movements:
- Elevation — temporalis, masseter, medial pterygoid (powerful)
- Depression — digastric, geniohyoid, mylohyoid, lateral pterygoid
- Protraction — lateral pterygoid (mainly), medial pterygoid
- Retraction — posterior temporalis, geniohyoid, digastric
4. MANDIBLE FRACTURES
Incidence
Mandible fractures are the 2nd most common facial fracture after nasal fractures. They account for ~37.5% of all maxillofacial fractures.
Common Causes
Assaults, motor vehicle crashes, falls.
Fracture Sites (Frequency)
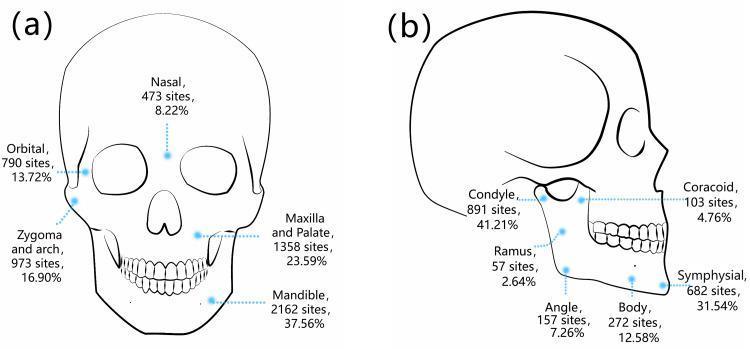
| Site | Frequency |
|---|---|
| Condyle | 41.2% (most common) |
| Symphysis/parasymphysis | 31.5% |
| Body | 12.6% |
| Angle | 7.3% |
| Coracoid/coronoid | 4.8% |
| Ramus | 2.6% (least common) |
Key point: A fracture of the mandibular body is accompanied by a contralateral fracture (often condylar neck) in approximately 50% of cases — because the mandible is a ring-like structure. — Grainger & Allison's Diagnostic Radiology
Classification of Fracture Sites
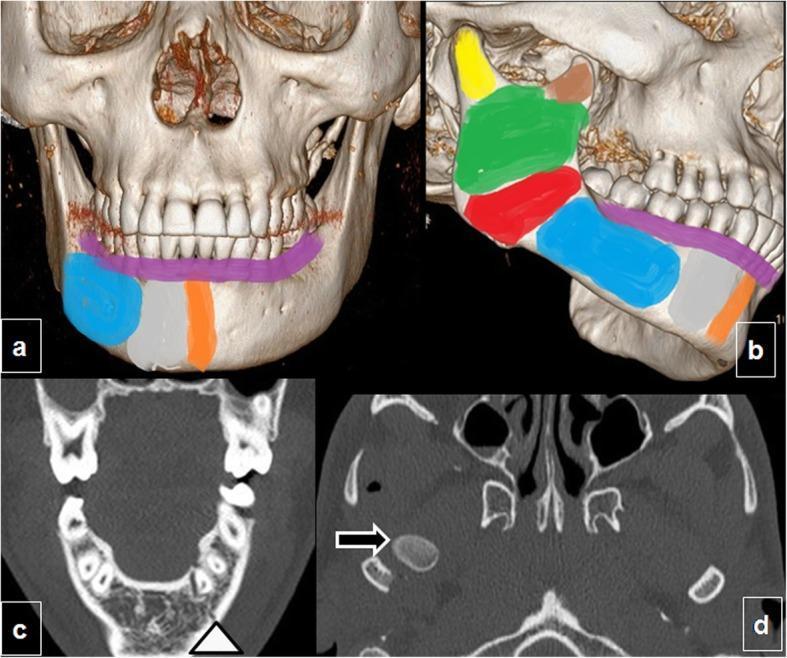
| Region | Definition |
|---|---|
| Symphyseal | Between the two mental foramina (midline = symphysis; off-midline = parasymphysis) |
| Body | Between mental foramen and angle |
| Angle | Region of third molar, behind dentition |
| Ramus | Behind angle; posterior edge of fracture behind angle |
| Subcondylar | Traverses sigmoid notch, exits behind angle |
| Vertical ramus | Sigmoid notch fracture exiting anterior to angle |
| Coronoid | Extends anteriorly from sigmoid notch |
| Alveolar | Separates tooth-bearing segment from rest of mandible |
— K.J. Lee's Essential Otolaryngology, p. 1108
Favorable vs. Unfavorable Fractures
- Favorable: Muscles pull fragments together (compress the fracture line)
- Unfavorable: Muscles distract fragments apart — harder to stabilize
Clinical Features of Mandible Fracture
- Malocclusion (key sign)
- Jaw deviation (toward the fracture side)
- Trismus / pain on jaw movement
- Lower lip/chin numbness (inferior alveolar nerve injury)
- Mucosal ecchymosis / floor of mouth hematoma
- Step deformity on palpation
Imaging
- OPG (orthopantomogram) — first-line for mandible fractures
- CT face — gold standard for complex fractures; 3D reconstruction aids surgical planning
- X-ray PA face + lateral oblique views
Management
- Occlusal restoration first — arch bars are the primary means of establishing correct occlusion (intermaxillary fixation, IMF)
- Fixation principles:
- Mini-plate (1.5–2.0 mm, monocortical) along the "ideal line of osteosynthesis" — below tooth roots, overcomes distraction at alveolar border
- Mandibular reconstruction plate (≥2.0 mm, bicortical) along inferior border for severe fractures
- Lag screws for overlapping/symphyseal fractures
- Subcondylar fractures:
- Closed treatment with elastic MMF (preferred in children) — "forced adaptation"
- Open reduction via submandibular (Risdon) incision, retromandibular (transparotid), or preauricular approach
— K.J. Lee's Essential Otolaryngology, p. 1114; Schwartz's Principles of Surgery
5. MANDIBLE DISLOCATION
- Head of mandible dislocates anteriorly (most common) over the articular tubercle
- Causes: wide mouth opening, yawning, trauma
- Clinical features: Open mouth that cannot close, jaw deviated contralaterally, pain
- Management: Manual reduction — thumbs on lower molars, press down and back (Hippocratic method); local anesthesia/sedation if needed
6. NERVE SUPPLY — QUICK VIVA POINTS
| Nerve | Relevance to Mandible |
|---|---|
| Inferior alveolar nerve (V3) | Enters mandibular foramen, runs in mandibular canal → exits at mental foramen as mental nerve |
| Mental nerve | Sensation to lower lip and chin |
| Nerve to mylohyoid | In mylohyoid groove on medial ramus |
| Lingual nerve | Passes medial to mandible near third molar area (at risk during wisdom tooth extraction) |
| Marginal mandibular branch (VII) | Crosses the body of mandible anterior to masseter — at risk in submandibular incisions |
7. EDENTULOUS MANDIBLE
- After tooth loss, the alveolar part is resorbed from top down → bone becomes thin and atrophic
- More vulnerable to fracture with less trauma
- More difficult to repair due to limited bone stock for screw fixation
- Increased risk at the mental foramen level
8. HIGH-YIELD VIVA FACTS
| Fact | Answer |
|---|---|
| Most common mandibular fracture site | Condyle (41%) |
| Most common facial fracture | Nasal bone; mandible is 2nd |
| Joint surface covered by | Fibrocartilage (not hyaline) |
| Lingula is attachment for | Sphenomandibular ligament |
| Muscle that depresses mandible | Digastric, mylohyoid, geniohyoid |
| Most powerful mandibular elevators | Temporalis + masseter + medial pterygoid |
| Nerve at risk in wisdom tooth surgery | Lingual nerve and inferior alveolar nerve |
| Nerve at risk in submandibular incision | Marginal mandibular branch of VII |
| Ring fracture rule | Body fracture → ~50% chance of contralateral condylar fracture |
| Edentulous mandible fracture is difficult because | Atrophic bone, limited fixation points |
This is a shared conversation. Sign in to Orris to start your own chat.