Cerebellum
Reading File
Finding Sources
Searching the Web
cerebellum anatomy function clinical overview
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Finding Sources
Reading File
Reading File
I now have comprehensive information from multiple authoritative textbooks. Let me compile the full answer.
The Cerebellum
Overview
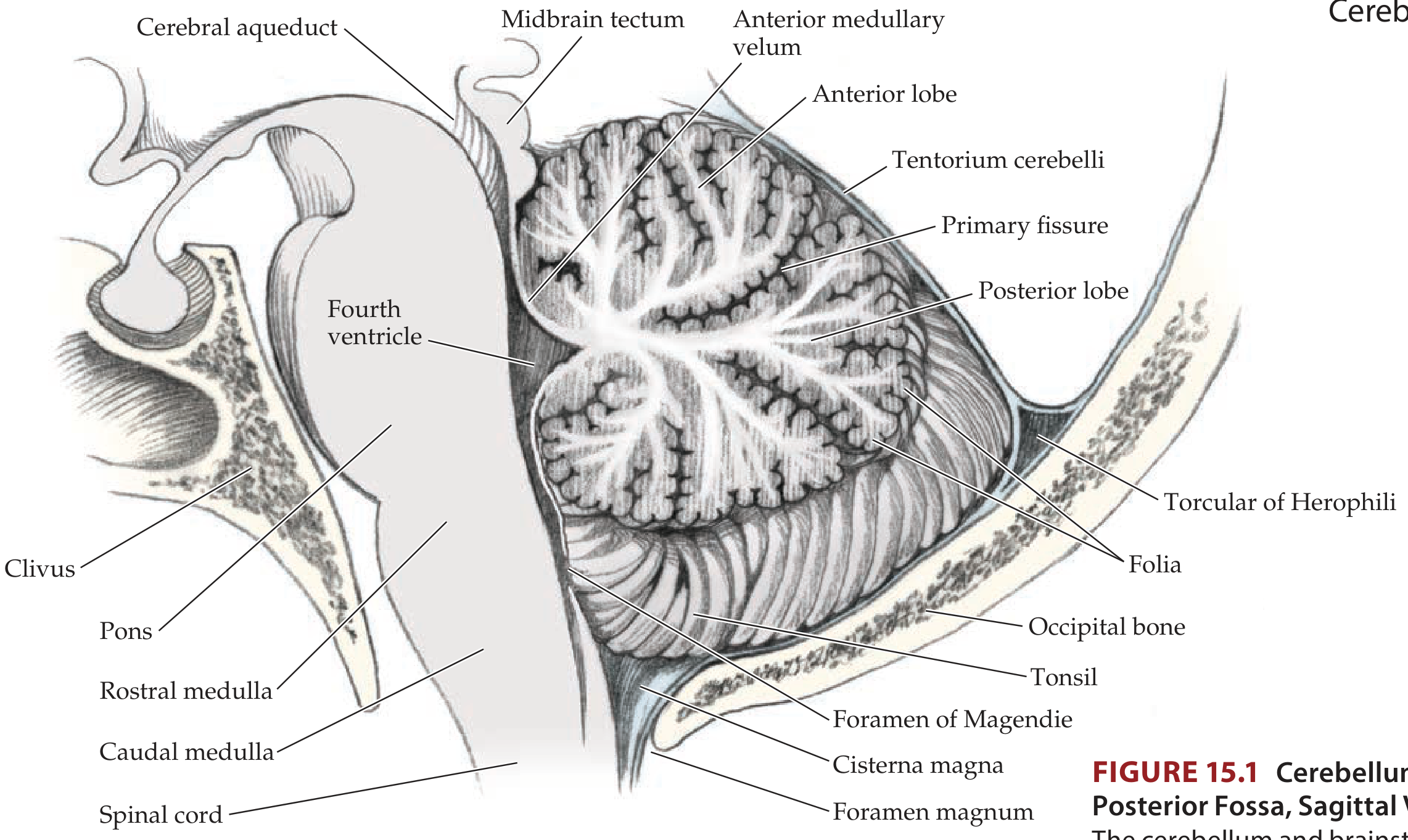
The cerebellum ("little brain") is a foliated, highly convoluted structure located in the posterior cranial fossa, dorsal to the pons and medulla, inferior to the occipital and temporal lobes. It forms the roof of the fourth ventricle. Despite weighing only ~10% as much as the cerebral cortex, its surface area is approximately 75% of the cortex - thanks to its densely packed folia ("leaves"). It contains more neurons than the entire cerebral cortex combined.
Its core functions are:
- Coordination of movement (rate, range, force, direction - collectively "synergy")
- Planning and execution of movement
- Maintenance of posture and balance
- Coordination of head and eye movements
- Motor learning
- Certain aspects of cognition and speech articulation
The cerebellum has no direct connections to lower motor neurons. It exerts its influence indirectly through motor systems of the cortex and brainstem.
Gross Anatomy and Lobes
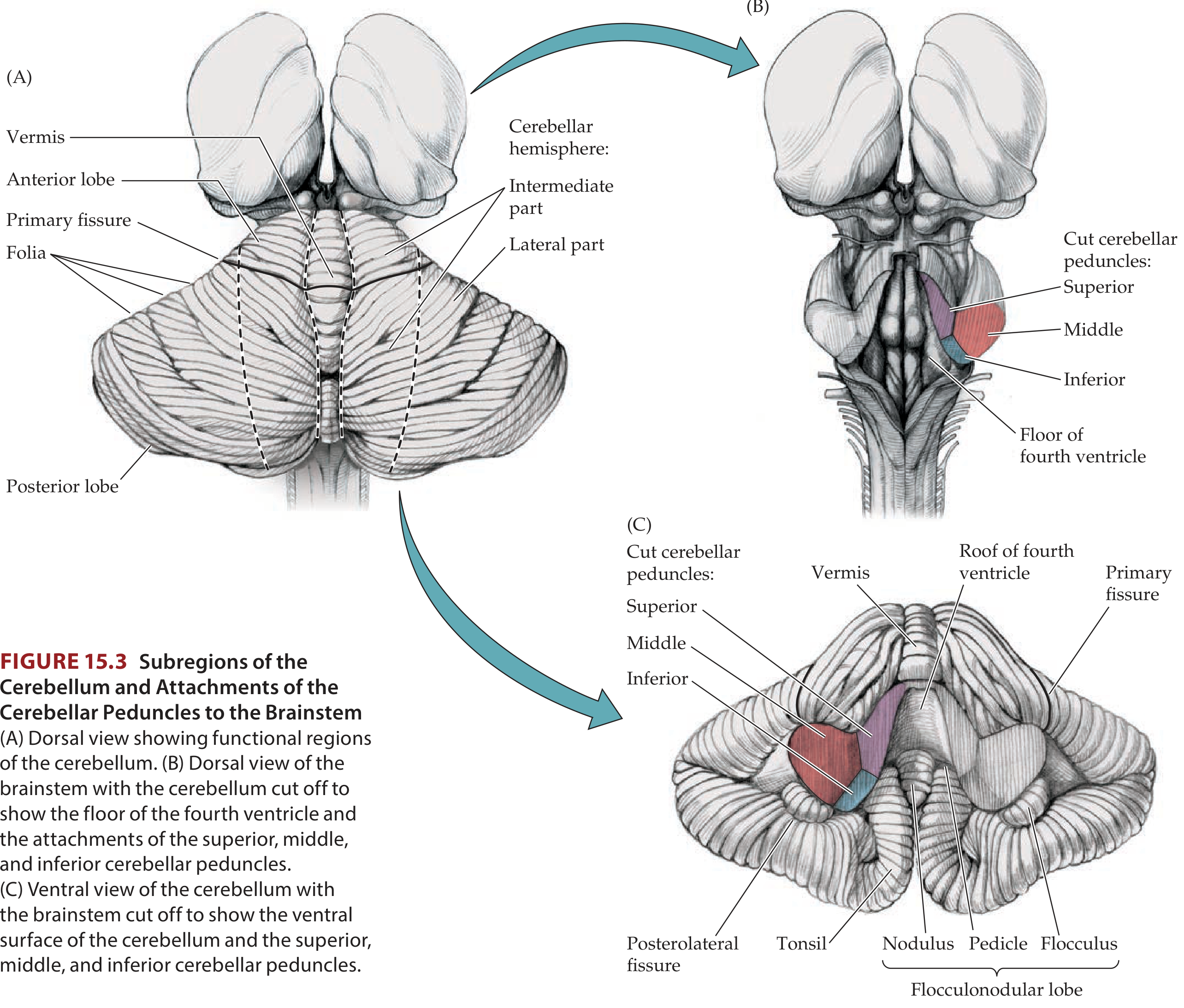
The cerebellum is divided by two transverse fissures:
| Fissure | Separates |
|---|---|
| Primary fissure | Anterior lobe from posterior lobe |
| Posterolateral fissure | Posterior lobe from flocculonodular lobe |
This gives three anatomical lobes:
- Anterior lobe - spinocerebellar input; synergy of movement
- Posterior lobe - largest; cerebrocortical input; motor planning
- Flocculonodular lobe - vestibular input; balance and eye movement
The midline vermis (wormlike) connects the two cerebellar hemispheres. The vermis contains 10 lobules (I-X, superior to inferior). The branching pattern of white matter within the cortex is called the arbor vitae ("tree of life").
Functional Divisions
There are three functionally distinct regions:
| Division | Dominant Input | Primary Function |
|---|---|---|
| Vestibulocerebellum (flocculonodular lobe + inferior vermis) | Vestibular | Balance, eye movements |
| Spinocerebellum (vermis + intermediate hemispheres) | Spinal cord (spinocerebellar tracts) | Synergy of ongoing movement; proximal & distal limb control |
| Pontocerebellum / Cerebrocerebellum (lateral hemispheres) | Cerebral cortex via pontine nuclei | Motor planning and initiation; cognition |
Cerebellar Peduncles
The cerebellum connects to the brainstem via three paired peduncles located around the fourth ventricle:
| Peduncle | Connection | Contents |
|---|---|---|
| Superior | Cerebellum - midbrain | Primarily efferent fibers from deep nuclei to red nucleus and thalamus |
| Middle | Cerebellum - pons | Only afferent fibers from contralateral pontine nuclei |
| Inferior | Cerebellum - medulla | Mixed afferents from brainstem/spinal cord; efferents to vestibular nuclei |
Deep Cerebellar Nuclei
There are four pairs of deep nuclei embedded in the white matter. From lateral to medial:
- Dentate - largest; receives from lateral hemispheres; projects via superior peduncle to contralateral VL thalamus and then motor cortex
- Emboliform - receives from intermediate hemisphere
- Globose - receives from intermediate hemisphere
- Fastigial - most medial; receives from vermis and flocculonodular lobe; projects to vestibular nuclei and medial motor systems
The emboliform and globose are sometimes combined as the interpositus nucleus.
Cerebellar Cortex - Layers and Cell Types
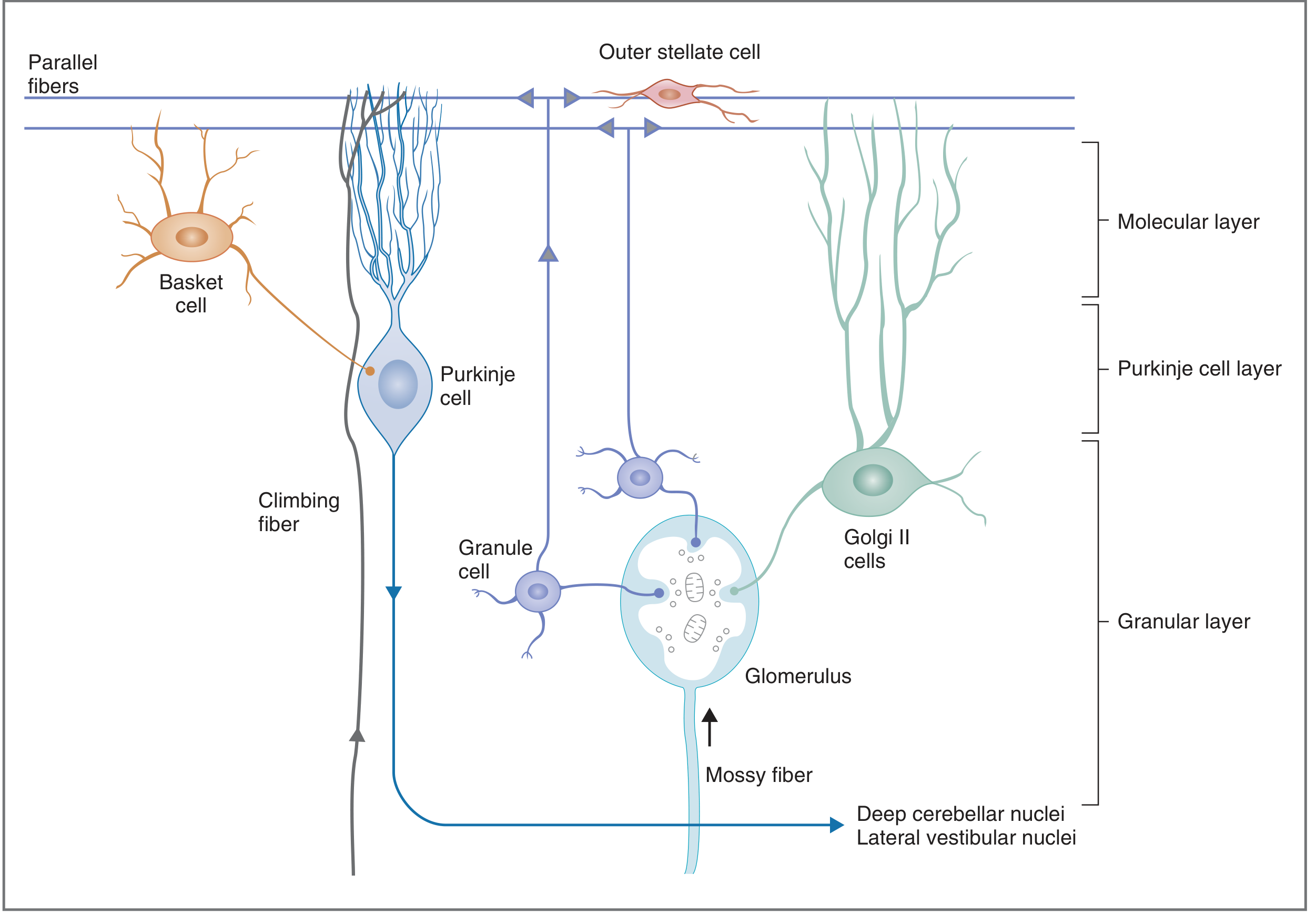
The cerebellar cortex has three layers containing five cell types:
Layers (outer to inner):
- Molecular layer - outer stellate cells, basket cells, dendrites of Purkinje/Golgi II cells, parallel fibers (axons of granule cells)
- Purkinje cell layer - one cell thick; Purkinje cells (only output of cortex)
- Granular layer - innermost; granule cells, Golgi II cells, glomeruli
Key Cells:
Purkinje cells are among the largest neurons in the CNS. Their extensively flattened dendritic arbors span the molecular layer, oriented perpendicular to parallel fibers. Their axons are the sole output of the cerebellar cortex, projecting to the deep cerebellar nuclei and lateral vestibular nuclei via inhibitory (GABA-ergic) synapses. Each Purkinje cell dendrite can receive input from up to 250,000 parallel fibers.
Afferent Fiber Systems
Two excitatory systems carry input into the cerebellar cortex (both also send collaterals directly to deep nuclei):
1. Climbing Fibers
- Originate in the inferior olive of the medulla
- Project directly onto Purkinje cell dendrites
- Each Purkinje cell receives input from only one climbing fiber, but that connection is powerful
- A single action potential generates complex spikes (multiple excitatory bursts)
- Thought to play a role in cerebellar learning and conditioning Purkinje cell responses
2. Mossy Fibers
- Constitute the majority of cerebellar afferent input
- Include vestibulocerebellar, spinocerebellar, and pontocerebellar fibers
- Synapse on granule cells in glomeruli (granular layer)
- Granule cells send axons to the molecular layer where they bifurcate into parallel fibers
- Parallel fibers run long distances, forming excitatory synapses on many Purkinje cells in a "beam" of excitation
- Produce simple spikes (single action potentials) in Purkinje cells
Inhibitory Interneurons
- Basket cells and stellate cells (molecular layer): inhibit Purkinje cells via parallel fibers
- Golgi II cells (granular layer): inhibit granule cells, reducing excitatory drive to Purkinje cells
- All interneurons except granule cells are inhibitory
Output Pathways
All output from the cerebellum is via Purkinje cells to the deep cerebellar nuclei, then:
| Region | Deep Nucleus | Peduncle | Target |
|---|---|---|---|
| Lateral hemisphere | Dentate | Superior (crosses in midbrain) | Contralateral VL thalamus → Motor cortex |
| Intermediate hemisphere | Interpositus (emboliform + globose) | Superior | Contralateral red nucleus and thalamus → Lateral motor systems |
| Vermis + flocculonodular | Fastigial / direct to vestibular nuclei | Inferior | Vestibular nuclei → Medial motor systems, eye movements |
Key principle: because cerebellar output crosses in the midbrain before reaching motor cortex (which itself crosses to the opposite side via the corticospinal tract), the net result is ipsilateral control - each cerebellar hemisphere coordinates the movements of the same-side limbs ("double crossing").
Clinical Correlations - Cerebellar Lesions
Cerebellar lesions produce ataxia - a loss of coordination in rate, range, force, and direction of movement (disrupted synergy). Three key localizing principles:
- Ataxia is ipsilateral to the cerebellar lesion (due to double-crossing of pathways)
- Midline/vermis lesions → truncal ataxia, unsteady gait, eye movement abnormalities, vertigo, nausea, vomiting
- Lateral hemisphere lesions → appendicular ataxia (limb incoordination)
Signs of Cerebellar Disease:
| Sign | Description |
|---|---|
| Ataxia | Uncoordinated, irregular movements |
| Dysmetria | Overshooting or undershooting a target (past-pointing) |
| Dysdiadochokinesia | Inability to perform rapid alternating movements |
| Intention tremor | Tremor perpendicular to movement, worsening near target (contrast with Parkinson's resting tremor) |
| Rebound phenomenon | Inability to stop a movement when resistance is suddenly removed |
| Nystagmus | Oscillating eye movements (especially with midline/vestibulocerebellum lesions) |
| Dysarthria | Slurred or scanning speech |
| Truncal ataxia | Wide-based, unsteady gait with falls |
Causes of Cerebellar Ataxia by Pattern:
| Pattern | Common Causes |
|---|---|
| Acute focal | Ischemic stroke, cerebellar hemorrhage, posterior fossa subdural hematoma, abscess |
| Acute/subacute symmetric | Alcohol, phenytoin, lithium, barbiturates, postinfectious (varicella), chemotherapy (fluorouracil, paclitaxel) |
| Subacute progressive | Paraneoplastic (anti-Yo with breast/ovarian cancer, anti-Tr with Hodgkin's), anti-GAD65 antibodies, gluten ataxia, prion disease |
| Chronic symmetric | Inherited ataxias (spinocerebellar ataxias), hypothyroidism, metabolic disorders, meningovascular syphilis |
Note on Tonsillar Herniation: Mass lesions or severe cerebral edema can force the cerebellar tonsils through the foramen magnum, compressing medullary respiratory centers - a neurosurgical emergency.
Sagittal View
Sources: Costanzo Physiology 7th Ed.; Ganong's Review of Medical Physiology 26th Ed.; Neuroanatomy through Clinical Cases 3rd Ed.; Harrison's Principles of Internal Medicine 22nd Ed. (2025)
This is a shared conversation. Sign in to Orris to start your own chat.