Teach me in simple way about enteric fever (typhoid) Epidemiology Pathogenesis Lab diagnosis Widal test Drug resistance prophylaxis Vaccine
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have everything I need. Let me write a comprehensive, well-organized, simple explanation of enteric fever.
Enteric Fever (Typhoid) - A Simple, Complete Guide
Sources: Harrison's Principles of Internal Medicine 22E (2025), Park's Textbook of Preventive & Social Medicine, Jawetz Melnick & Adelberg's Medical Microbiology 28E
What Is It?
Enteric fever (typhoid) is a severe, systemic illness - meaning it affects the whole body, not just the gut - caused mainly by Salmonella Typhi or, less commonly, Salmonella Paratyphi (A, B, C). It was originally called "typhoid fever" because it resembled typhus. The term "enteric fever" came later (1869) to reflect the intestinal site of infection.
Think of it simply: You swallow contaminated food/water → bacteria invade your gut → spread to the bloodstream and organs → cause prolonged high fever and systemic illness.
1. EPIDEMIOLOGY
Global burden:
- An estimated 9.2-21 million cases of typhoid and ~5 million of paratyphoid occur annually, causing 110,000-280,000 deaths per year.
- Worldwide distribution of typhoid incidence (cases per 100,000 population per year):
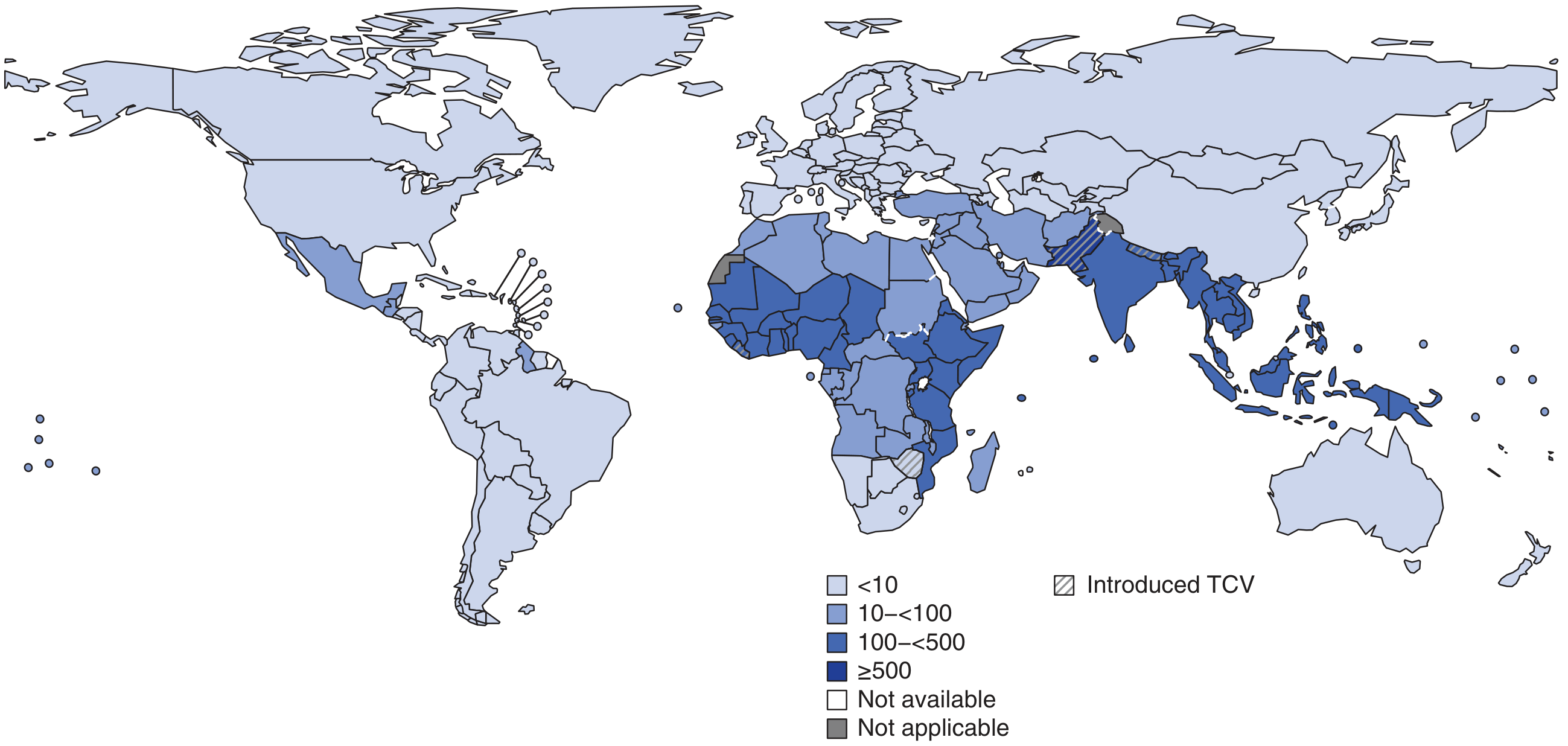
Incidence exceeds 1,000/100,000 children in some urban areas of the Indian subcontinent (Pakistan, Bangladesh, Nepal, India). - Harrison's 22E, p.1359
Who gets it?
- Most common in children and adolescents (5-15 years) in endemic areas
- Urban slum areas: incidence can hit 180-494 per 100,000 children aged 5-15
- After age 20, incidence drops as immunity builds from prior exposure
- More cases in males (more exposure), but carrier rate higher in females
- In the US/Western Europe, most cases are travel-related (78%), mostly from visiting South Asia
Why does it spread?
- Only humans are the natural host - no animal reservoir
- Spread via the fecal-oral route - contaminated water, food (especially milk, raw vegetables, street food), ice, and flies
- Typhoid bacilli survive 48 hours in water, >1 month in ice, and can multiply rapidly in milk without changing its taste
- Peak incidence: July-September (rainy season, more flies)
- Typhoid fever is literally an index of poor sanitation in a country
Carriers (chronic): 1-4% of patients become chronic carriers, harboring the organism in the gallbladder and shedding it in stools/urine for >1 year.
2. PATHOGENESIS
Step-by-step: How S. Typhi causes disease
Ingestion of contaminated food/water
↓
Bacteria reach the small intestine
(infective dose for typhoid: as low as 10³ organisms)
↓
Enter via specialized M-cells overlying Peyer's patches
(lymphoid tissue in the gut wall)
↓
Pass into intestinal lymphatics
↓
Primary bacteremia (1st bacteremia) → seeded into:
Liver, Spleen, Bone marrow, Gallbladder
(bacteria multiply inside macrophages - INTRACELLULAR phase)
↓
Secondary bacteremia (causes the prolonged fever and systemic illness)
↓
Bacteria re-enter intestine via bile
→ Hyperplasia then NECROSIS of Peyer's patches
→ Risk of ulceration, hemorrhage, perforation (3rd week)
Key pathological lesions:
- Hyperplasia and necrosis of Peyer's patches (classic hallmark)
- Focal liver necrosis (hepatitis)
- Enlarged mesenteric lymph nodes
- Inflammation of gallbladder (bacteria multiply here - this is why carriers exist)
- Splenomegaly
Host defenses that protect you:
- Gastric acidity (low stomach pH kills bacteria)
- Normal gut microbiota
- Cell-mediated immunity (S. Typhi is intracellular, so CMI is more important than antibodies)
Clinical progression by weeks:
| Week | What happens | Signs |
|---|---|---|
| Week 1 | Bacteremia begins | Step-ladder fever, headache, malaise, constipation, dry cough |
| Week 2 | Peak fever, systemic illness | Rose spots (~30%), splenomegaly, relative bradycardia, "toxic" appearance |
| Week 3 | Peyer's patch necrosis | Diarrhea ("pea soup"), risk of intestinal bleeding or perforation |
| Week 4 | Recovery or complications | Improvement if treated; relapse possible 2 weeks after therapy ends |
"Rose spots" - the classic rash of typhoid:
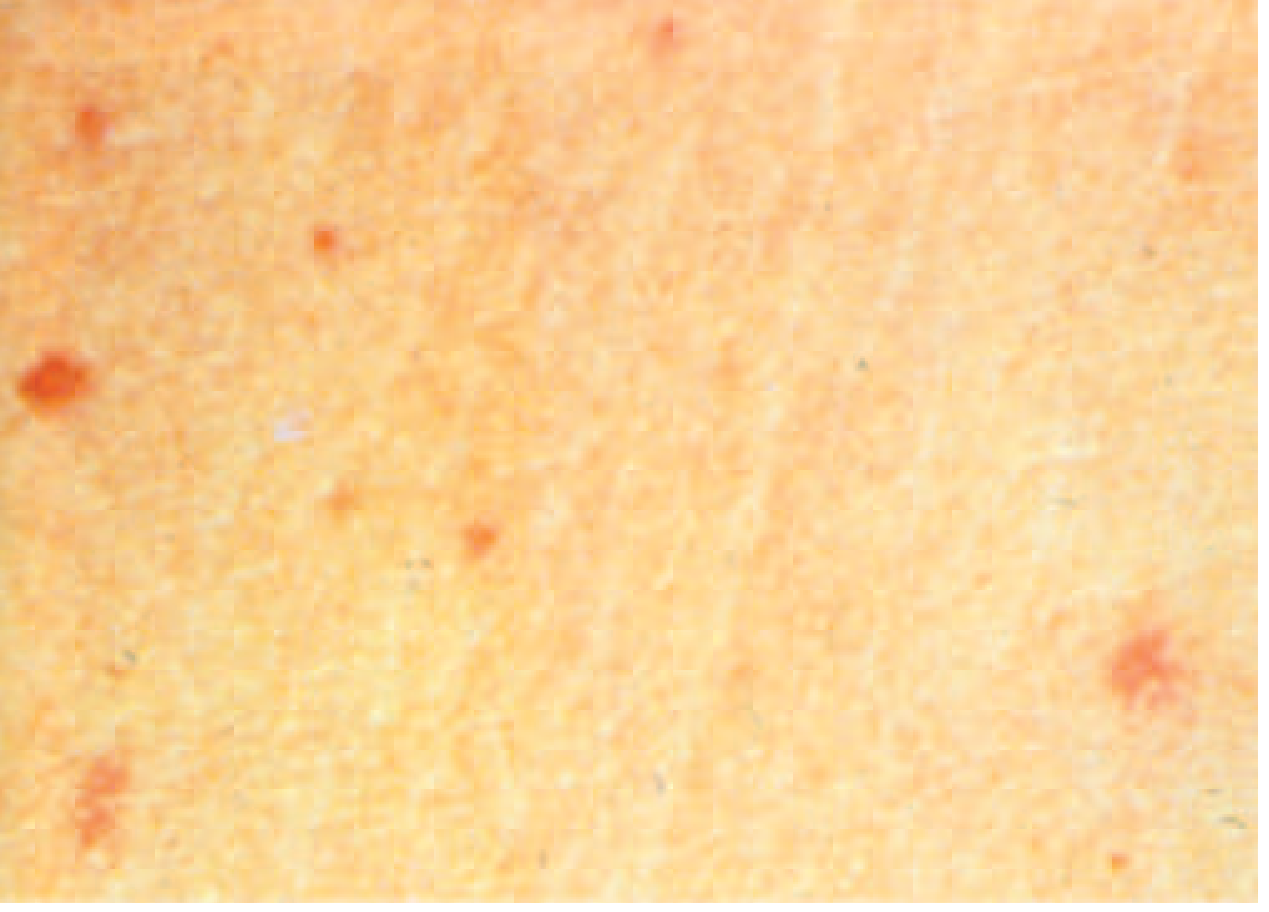
Faint, salmon-colored, 2-3 mm papules on the trunk. Blanch on pressure. Appear in Week 2 in ~30% of patients. - Harrison's 22E, p.1360
Complications (occur in up to 10% of cases):
- Intestinal perforation (most likely Week 3) - sudden drop in temperature + signs of shock
- Intestinal hemorrhage
- Myocarditis, pneumonia, cholecystitis, nephritis, osteomyelitis, meningitis
3. LABORATORY DIAGNOSIS
A. Culture (Gold Standard)
| Specimen | Sensitivity | When Best |
|---|---|---|
| Blood culture | 40-60% | Week 1-2 (early disease) |
| Bone marrow culture | ~80% | Any time, even after 5 days of antibiotics |
| Stool culture | 30-40% in Week 1; better in Week 3 | Week 3 onwards |
| Urine culture | Less reliable | Week 2-3 |
| Duodenal string test (intestinal secretions) | High if bone marrow negative | Confirms carrier state |
Combined yield: If blood + bone marrow + intestinal secretions are all cultured together, yield exceeds 90%.
Why is blood culture sensitivity low? There are very few organisms in the blood (<15/mL), and prior antibiotics reduce yield further.
Culture media used:
- Differential media: MacConkey, EMB agar - S. Typhi appears as colorless (non-lactose fermenting) colonies
- Selective media: SS agar, Hektoen Enteric (HE) agar, XLD agar - salmonellae appear as black colonies (due to H₂S production)
- Enrichment media (for stool): Selenite F broth or Tetrathionate broth - inhibit normal gut flora, let Salmonella multiply before plating
B. CBC (Non-specific but helpful)
- Leukopenia and neutropenia in 15-25% of cases (unusual for a bacterial infection - a helpful clue!)
- Leukocytosis suggests perforation or secondary infection
- Mildly elevated liver enzymes
C. Rapid Diagnostic Tests
- Typhidot and Tubex - detect IgM/IgG against O and H antigens
- Sensitivity 70-80%, specificity 80-90%
- Widely used at point-of-care in endemic areas (cheap, simple)
- Not accurate enough to replace blood culture as the main test
D. PCR
- Sensitivity 40-100% (depending on gene target)
- Previously limited to well-resourced labs, now becoming more feasible after COVID-19 expanded molecular diagnostics
4. WIDAL TEST
What is it?
The Felix-Widal test (Tube Dilution Agglutination Test) measures antibodies against the O (somatic) antigen and H (flagellar) antigen of S. Typhi. Developed in the 1890s by Georges Fernand Isidor Widal.
How it works (simple version):
- Patient's serum is mixed with S. Typhi antigens in serial dilutions in tubes
- If antibodies are present, agglutination (clumping) occurs
- The highest dilution at which clumping occurs = the titer
When do antibodies appear?
| Antibody | Appears on | Peaks by |
|---|---|---|
| O antibodies | Day 6-8 | 2nd-3rd week |
| H antibodies | Day 10-12 | 2nd-3rd week |
| Vi antibodies | Variable | Present in ~80% of chronic carriers |
Interpretation:
- Significant titer: O ≥ 1:80 and H ≥ 1:160 in a single sample (varies by endemic background)
- Better evidence: 4-fold rise in titer between acute and convalescent sample (2 samples, 7-10 days apart) is stronger evidence
- Vi agglutinins useful for identifying chronic carriers (present in ~80%)
Limitations of Widal test (important!):
- False positives - S. Typhi shares O and H antigens with other Salmonella serotypes and even other bacteria → cross-reactions
- False negatives - prior antibiotic therapy blunts antibody response; test can be negative in up to 30% of culture-proven cases
- Difficult to interpret in endemic areas - baseline antibody levels are elevated in the general population
- Prior vaccination raises H antibody titers (vaccinated person looks positive even without disease)
- Single sample is unreliable - must use two samples ideally
The CDC does not recommend the Widal test for diagnosing acute typhoid because it is too difficult to interpret in endemic populations. It is still widely used on the Indian subcontinent. - Red Book 2021, Park's Textbook
5. DRUG RESISTANCE AND TREATMENT
The Evolution of Resistance
| Era | What happened |
|---|---|
| 1940s-1980s | Chloramphenicol, ampicillin, trimethoprim-sulfamethoxazole (TMP-SMX) used as first-line drugs |
| 1980s-1990s | MDR (Multidrug-Resistant) S. Typhi emerged in China/SE Asia → spread worldwide. MDR = resistance to chloramphenicol + ampicillin + TMP-SMX (carried on plasmids) |
| 1990s onward | Fluoroquinolones (ciprofloxacin, ofloxacin) became the treatment of choice |
| 2000s onward | DSC S. Typhi emerged (Decreased Susceptibility to Ciprofloxacin) on Indian subcontinent |
| 2016-present | XDR (Extensively Drug-Resistant) S. Typhi in Pakistan - resistant to fluoroquinolones + third-gen cephalosporins + all first-line drugs. Only azithromycin or carbapenems remain effective |
Treatment Table
| Type of S. Typhi | Drug of Choice | Alternatives |
|---|---|---|
| Fully sensitive | Fluoroquinolone (ciprofloxacin/ofloxacin) 15 mg/kg/day × 5-7 days | Chloramphenicol, Amoxicillin, TMP-SMX |
| MDR (resistant to Cl/Amp/TMP) | Fluoroquinolone OR Cefixime (oral) | Ceftriaxone IV |
| DSC (reduced fluoroquinolone susceptibility) | Azithromycin OR Ceftriaxone | High-dose fluoroquinolone (less reliable) |
| XDR | Azithromycin (if susceptible) or Carbapenems | Clinical trials ongoing |
A 2022 systematic review of 27 RCTs found no significant difference between ceftriaxone, fluoroquinolones, and azithromycin in treatment failure when the strain is susceptible. - Harrison's 22E
Severely ill/toxic patients: Hydrocortisone 100 mg IV daily for 3-4 days can be added.
Prophylaxis (Control Measures)
Individual level:
- Boil or chemically treat drinking water
- Avoid raw fruits/vegetables from possibly sewage-irrigated fields
- Avoid street food and ice in endemic areas
- Hand washing (especially food handlers)
Community level:
- Safe water supply and sewage treatment
- Proper food handling and hygiene
- Fly control
- Notification of cases (enteric fever is a notifiable disease)
Carriers:
- Identified via stool culture + Vi antibody testing
- Treated with ampicillin or amoxicillin (4-6 g/day) + Probenecid × 6 weeks (concentrated in bile) - achieves eradication in ~70%
- Cholecystectomy (removal of gallbladder) + ampicillin if medical treatment fails (gallbladder is the reservoir)
- Carriers must NOT work as food handlers or healthcare workers
6. VACCINES
Why vaccines matter:
Typhoid vaccines are an adjunct to sanitation - they help when you cannot yet guarantee safe water and food.
Three main vaccines:
A. Vi Polysaccharide Vaccine (Vi CPS) - Injectable
- Composition: Purified Vi capsular polysaccharide from S. Typhi Ty2 strain
- Mechanism: T-cell independent IgG response
- Schedule: Single IM/SC dose; booster every 2-3 years
- Age: ≥ 2 years
- Efficacy: ~55% at 3 years
- Limitation: Does NOT work in children <2 years (can't mount T-cell independent response effectively); response not boosted by additional doses
- Safety: Minimal side effects; safe in HIV+ (efficacy correlates with CD4 count)
B. Ty21a Oral Live Attenuated Vaccine
- Composition: Chemically mutated live S. Typhi Ty2 strain (multiple gene mutations, including loss of Vi production) in enteric-coated capsules
- Schedule: Days 1, 3, 5, 7 (4 doses); repeat full series every 5 years
- Age: ≥ 6 years
- Efficacy: ~50% at 2.5-3 years
- Storage: 2-8°C; stable ~14 days at 25°C
- Limitation: Cannot be used with antibiotics (antibiotics kill the live vaccine); not studied in children <3 years; requires multiple doses
C. Typhoid Conjugate Vaccines (TCV) - NEW GENERATION
- Two WHO-recommended vaccines: Typbar TCV (Bharat Biotech, licensed 2018) and TYPHIBEV (Biological E, licensed 2020)
- How it's different: Vi polysaccharide is conjugated (chemically linked) to a carrier protein → this makes it T-cell DEPENDENT → works in children <2 years, generates immunologic memory, can be boosted
- Schedule: Single IM dose (0.5 mL)
- Age: From infancy (≥6 months)
- Efficacy: 79-95% protection; antibody response persists up to 7 years
- Current use: Introduced in national immunization programs in Pakistan, Nepal, Liberia, Zimbabwe, Malawi, and Samoa (as of 2023)
- This is the future of typhoid immunization - especially important for high-burden countries
Vaccine Comparison at a Glance
| Feature | Vi CPS (Injectable) | Ty21a (Oral) | TCV (Conjugate) |
|---|---|---|---|
| Route | IM/SC | Oral | IM |
| Doses | 1 | 4 | 1 |
| Min age | 2 years | 6 years | 6 months |
| Efficacy | ~55% | ~50% | 79-95% |
| Duration | 2-3 years | 5 years | ≥7 years |
| Works <2 yrs | No | No | Yes |
| WHO recommended | Yes | Yes | Priority |
Who should get vaccinated?
- Travelers to South Asia, Africa, SE Asia, Caribbean, Central/South America
- Household contacts of known S. Typhi carriers
- Clinical microbiology or research lab workers
- Children in high-burden endemic areas (via TCV national programs)
- Note: Vaccine is NOT recommended for managing post-exposure contacts in a common-source outbreak
Quick Memory Summary
ENTERIC FEVER (TYPHOID) - MEMORY MAP
Organism: S. Typhi (main) | S. Paratyphi A, B, C
Reservoir: Humans ONLY
Route: Fecal-oral (water, milk, food, flies)
IP: 10-14 days (range 5-21 days)
PATHOGENESIS: Mouth → M-cells → Peyer's patches
→ Lymphatics → Bloodstream → Organs
→ Back to gut via bile → Ulceration/Perforation
DIAGNOSIS:
Gold standard: Blood culture (sensitivity 40-60%)
Best single: Bone marrow culture (~80%)
Widal test: O antibodies (Day 6-8), H (Day 10-12)
Significant: O≥1:80, H≥1:160
LIMITATIONS: False positives, cross-reactions, prior vaccination
TREATMENT:
Fully sensitive: Fluoroquinolones
MDR: Fluoroquinolones / Ceftriaxone
XDR: Azithromycin / Carbapenems
VACCINES:
Vi CPS: 1 dose IM, age ≥2yr, efficacy 55%, booster q2-3yr
Ty21a: 4 doses oral, age ≥6yr, efficacy 50%, repeat q5yr
TCV: 1 dose IM, age ≥6mo, efficacy 79-95%, lasts ≥7yr ← BEST
References: Harrison's Principles of Internal Medicine 22E (2025), p.1359-1362 | Park's Textbook of Preventive & Social Medicine, p.277-282 | Jawetz, Melnick & Adelberg's Medical Microbiology 28E
This is a shared conversation. Sign in to Orris to start your own chat.