CVP and its importantance . Make md anaesthesia notes
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Running Command
ls -la /home/daytona/workspace/ 2>/dev/null || echo "workspace not found"
Writing File
~/CVP_Anaesthesia_Notes.md
# Central Venous Pressure (CVP) — Anaesthesia Notes
---
## 1. Definition
**Central Venous Pressure (CVP)** is the blood pressure measured in the superior vena cava or right atrium. It approximates **right atrial pressure (RAP)** and therefore serves as an index of:
- Right ventricular preload
- Circulating blood volume
- Venous tone
- Right ventricular performance
> Normal CVP: **2–8 mmHg** (supine, at rest)
---
## 2. Physiological Basis
CVP reflects the balance between venous return to the right heart and the ability of the right ventricle to eject that volume. It is influenced by:
| Factor | Effect on CVP |
|--------|---------------|
| Hypovolaemia | ↓ CVP |
| Hypervolaemia | ↑ CVP |
| Right heart failure | ↑ CVP |
| Cardiac tamponade | ↑ CVP |
| Tension pneumothorax | ↑ CVP |
| PEEP / high intrathoracic pressure | ↑ CVP |
| Vasodilation (sepsis, anaesthesia) | ↓ CVP |
| Tricuspid regurgitation | ↑ CVP (ventricularised waveform) |
> **Key limitation**: CVP reflects **right-sided** heart function, NOT left ventricular performance.
---
## 3. Indications for CVP Monitoring / CVC Insertion
*(Miller's Anaesthesia, 10e — Box 32.5)*
### Monitoring indications
- CVP and haemodynamic monitoring in unstable patients / major surgery
- Pulmonary artery catheterisation
- Transvenous cardiac pacing
### Access indications
- Infusion of vasoactive drugs (adrenaline, noradrenaline, vasopressin)
- Hyperalimentation / total parenteral nutrition (TPN)
- Chemotherapy or agents irritating to peripheral veins
- Prolonged antibiotic therapy (e.g., endocarditis)
- Rapid fluid resuscitation via large-bore introducer sheath
- Trauma or major surgery
- Aspiration of venous air emboli
- No adequate peripheral IV access
- Repeated blood sampling
---
## 4. Access Sites
| Site | Advantages | Disadvantages |
|------|-----------|---------------|
| **Right internal jugular (RIJ)** | Most direct route to RA/RV; highest success rate; preferred for pacing wire / PA catheter | Carotid artery risk; patient discomfort |
| **Left internal jugular** | Alternative when right unavailable | Longer to SVC (3–5 cm extra); thoracic duct risk |
| **Subclavian** | Patient comfort; lower infection risk | Higher pneumothorax risk — avoid in severe emphysema; difficult to compress if bleeding |
| **External jugular** | Easy in some patients | Kinks in lateral decubitus (problem during thoracotomy / OLV) |
| **Femoral** | Useful when neck immobilised (trauma) | Infection risk; catheter may not reach central circulation reliably |
| **Antecubital (PICC)** | Minimally invasive | Longer insertion; positional |
### Site selection principles
- **Coagulopathic patients** → internal or external jugular (compressible); avoid subclavian
- **Severe emphysema** → internal jugular (lower pneumothorax risk vs subclavian)
- **Emergency transvenous pacing** → right internal jugular (most direct route to RV)
- **Cervical collar / trauma** → femoral or subclavian approach
---
## 5. Technique Essentials
- Use **real-time ultrasound guidance** — strongly recommended, especially for internal jugular (reduces complications, increases first-pass success)
- Use **maximal barrier precautions** (cap, mask, sterile gown, sterile gloves, full-body drape)
- **Seldinger technique**: needle → guide wire → dilator → catheter
- Confirm venous placement with **waveform manometry or pressure measurement** before use
- Verify catheter tip position on **chest X-ray** — tip should lie in SVC above the right atrial junction (within 2 cm of cardiac silhouette on AP CXR for PA catheter)
---
## 6. CVP Waveform
### 6.1 Normal Waveform Components
*(Miller's Anaesthesia 10e — Table 32.3)*
| Component | Phase | Mechanical Event | ECG Timing |
|-----------|-------|------------------|------------|
| **a wave** | End-diastole | Atrial contraction ("atrial kick") | After P wave |
| **c wave** | Early systole | Isovolumic ventricular contraction; tricuspid valve bulges into RA | End of QRS |
| **x descent** | Mid-systole | Atrial relaxation + descent of tricuspid annulus toward apex | Before T wave |
| **v wave** | Late systole | Venous filling of atrium while tricuspid is closed | End of T wave |
| **y descent** | Early diastole | Tricuspid valve opens; blood flows RA → RV | Before P wave |
| **h wave** | Mid-to-late diastole | Diastolic plateau (only seen at slow HR or elevated CVP) | — |
**Mnemonic**: a = Atrial contraction; c = Closure of tricuspid; x = eXit of blood (atrial relaxation); v = Venous filling; y = Yield to ventricle
> CVP is read at the **base of the c wave at end-expiration** (Fishman's Pulmonary, 5e)
### 6.2 CVP Waveform Image
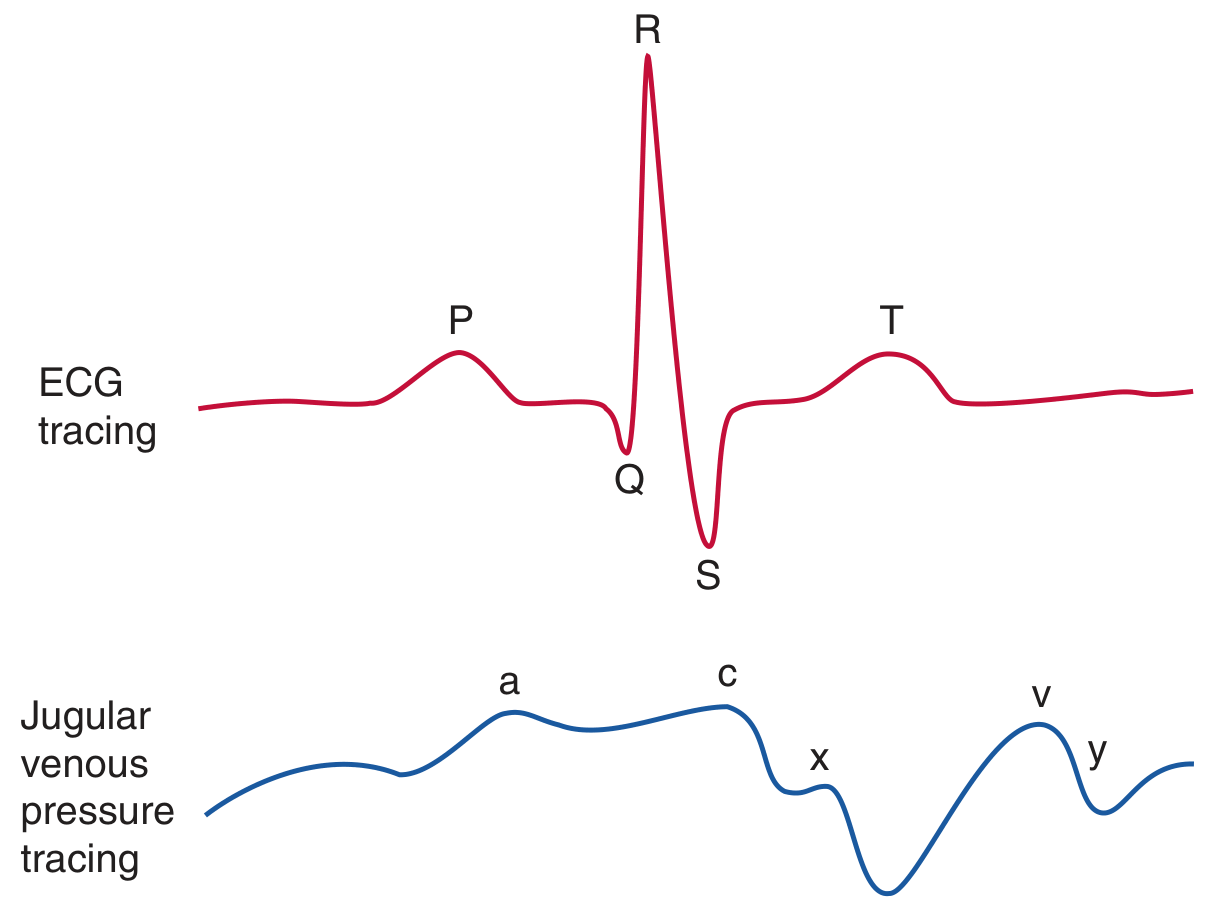
*CVP waveform with simultaneous ECG. The a wave follows the P wave; the c wave follows the QRS; the v wave peaks after the T wave.*
---
## 7. CVP Waveform Abnormalities
*(Miller's Anaesthesia 10e — Table 32.3 Abnormalities)*
| Condition | Waveform Change | Mechanism |
|-----------|----------------|-----------|
| **Atrial fibrillation** | Loss of a wave; prominent c wave | No organised atrial contraction |
| **AV dissociation / complete heart block** | Cannon a waves | Atrium contracts against closed tricuspid |
| **Tricuspid regurgitation** | Tall systolic c-v wave; loss of x descent ("ventricularised" waveform) | Regurgitant systolic filling of RA |
| **Tricuspid stenosis** | Tall a wave; attenuated y descent | Impaired diastolic emptying of RA |
| **Cardiac tamponade** | Dominant x descent; attenuated y descent ("x without y") | Equalised pressures; impaired RA filling in diastole |
| **Pericardial constriction** | Tall a and v waves; steep x AND y descents; M or W pattern | Impaired ventricular filling with exaggerated pressure equalisation |
| **RV ischaemia / infarction** | Tall a and v waves; steep x and y descents; M or W pattern | Poor RV compliance |
| **Junctional rhythm** | Loss of a wave | No P wave → no organised atrial contraction |
---
## 8. Measurement Technique
### Zeroing and levelling
- Zero reference point: **5 cm below the sternal angle** (uppermost fluid level in RA) OR **one-third of thoracic AP dimension** (mid-RA level)
- Commonly: mid-thoracic level (phlebostatic axis)
- Consistency throughout monitoring period is **most important**
### Respiratory variation
- Measure at **end-expiration** in both spontaneous and positive-pressure ventilation
- PEEP elevates CVP — account for this when interpreting values
---
## 9. Clinical Interpretation
### CVP in shock
| Shock Type | Expected CVP |
|------------|-------------|
| Hypovolaemic | Low (↓) |
| Distributive (sepsis, anaphylaxis) | Low (↓) |
| Cardiogenic (right heart failure) | High (↑) |
| Obstructive (tamponade, tension pneumothorax, massive PE) | High (↑) |
> These are generalisations — CVP must be interpreted in the full clinical context.
### CVP and fluid responsiveness
**CVP is a POOR predictor of fluid responsiveness.** (Miller's Anaesthesia 10e; Barash Clinical Anaesthesia 9e)
- Multiple RCTs and systematic reviews show **very poor relationship between CVP and circulating blood volume**
- A single static CVP value **cannot predict** response to a fluid challenge
- **Dynamic variables are preferred** for guiding fluid therapy:
- Pulse pressure variation (PPV)
- Stroke volume variation (SVV)
- Passive leg raise response
- Oesophageal Doppler
- Point-of-care echocardiography
> *"Consensus guidelines recommend against using static measures like CVP to assess the likelihood of fluid responsiveness, favouring use of dynamic variables."* — Fishman's Pulmonary Diseases and Disorders, 5e
---
## 10. Complications of CVC Insertion
*(Miller's Anaesthesia 10e — Box 32.6)*
Up to **15%** of patients may experience some adverse event.
### Mechanical
- **Arterial puncture** — most common acute complication (1.9–15%); can cause haematoma, AV fistula, pseudoaneurysm, or stroke (carotid)
- **Pneumothorax** — higher with subclavian approach; catastrophic if in dependent lung during OLV
- **Haemothorax / hydrothorax / haemomediastinum**
- **Chylothorax** (left subclavian / left IJ — thoracic duct injury)
- **Air embolism** — risk during insertion (Trendelenburg position reduces risk)
- **Catheter malposition** — tip in wrong vessel or chamber
- **Arrhythmias** — guide wire irritation of RV/RA
### Thromboembolic
- **Deep vein thrombosis** — especially femoral and subclavian sites
- **Pulmonary embolism**
- **Catheter-related thrombosis**
### Infectious
- **Central line-associated bloodstream infection (CLABSI)** — significant cause of ICU morbidity/mortality
- Prevention: maximal barrier precautions, chlorhexidine skin prep, standardised insertion checklists, daily review of necessity
---
## 11. Specific Anaesthetic Contexts
### Thoracic surgery / pneumonectomy
- CVP catheter commonly placed for oesophagectomy and pneumonectomy
- **Avoid subclavian approach** — pneumothorax risk in dependent lung during OLV is catastrophic
- **External jugular should be avoided** during thoracotomy — kinks when patient turned to lateral decubitus
- CVP no longer considered accurate guide for fluid responsiveness in thoracic surgery
- *(Barash Clinical Anaesthesia 9e)*
### Cardiac surgery / haemodynamically unstable patients
- CVP used alongside other haemodynamic monitors (PA catheter, TOE)
- PA catheter placed through right IJ via the CVC site
- Characteristic pressure waveforms confirm passage through RA → RV → PA → wedge position
### Transvenous pacing emergencies
- **Right internal jugular** preferred — most direct route to RV
---
## 12. Summary — Key Points for Exams
1. CVP = right atrial pressure ≈ RV preload (NOT LV preload)
2. Normal: **2–8 mmHg**; measured at **end-expiration** at the **base of the c wave**
3. CVP waveform: **a, c, v** waves and **x, y** descents — timed against ECG
4. **Cannon a waves** = AV dissociation; **loss of a wave** = AF; **c-v fusion + loss of x** = tricuspid regurgitation
5. **CVP is a poor predictor of fluid responsiveness** — dynamic variables are preferred
6. **Right internal jugular** = preferred site for pacing wires and PA catheters
7. **Subclavian** has highest pneumothorax risk — avoid in emphysema and OLV cases
8. Complications: arterial puncture, pneumothorax, CLABSI, arrhythmias, air embolism
9. Always use **ultrasound guidance** (strongly recommended for IJ)
10. Waveform abnormalities are diagnostically useful — especially tamponade (dominant x, absent y) vs. constriction (steep x AND y)
---
*Sources: Miller's Anaesthesia 10e (Elsevier); Barash, Cullen & Stoelting's Clinical Anaesthesia 9e; Fishman's Pulmonary Diseases and Disorders 5e; Morgan & Mikhail's Clinical Anaesthesiology 7e*
Here are your comprehensive anaesthesia notes on CVP:
CVP Anaesthesia Notes
MD File · MD
Central Venous Pressure (CVP) — Anaesthesia Notes
1. Definition
CVP = pressure in the superior vena cava / right atrium ≈ right atrial pressure (RAP)
Reflects:
- RV preload
- Circulating blood volume
- Venous tone
- RV performance
Normal CVP: 2–8 mmHg
2. Physiological Basis
| Factor | Effect on CVP |
|---|---|
| Hypovolaemia | ↓ |
| Right heart failure | ↑ |
| Cardiac tamponade | ↑ |
| Tension pneumothorax | ↑ |
| PEEP | ↑ |
| Vasodilation (sepsis, anaesthesia) | ↓ |
| Tricuspid regurgitation | ↑ (ventricularised) |
CVP reflects right-sided heart function — NOT left ventricular performance. (Barash Clinical Anaesthesia 9e)
3. Indications for CVC Insertion
- CVP monitoring in haemodynamically unstable patients and major surgery
- Transvenous cardiac pacing
- Infusion of vasoactive drugs, TPN, chemotherapy, vesicant agents
- Rapid fluid resuscitation (large-bore introducer)
- Pulmonary artery catheterisation
- Aspiration of air emboli
- No peripheral access; repeated blood sampling
4. Access Sites
| Site | Key Points |
|---|---|
| Right IJ | Highest success; direct route to RA/RV; preferred for pacing + PA catheter |
| Subclavian | Highest pneumothorax risk — avoid in emphysema and OLV cases |
| Left IJ / EJ | 3–5 cm longer to SVC; EJ kinks in lateral decubitus (problem in thoracotomy) |
| Femoral | Useful when neck immobilised (trauma); infection risk |
Site selection:
- Coagulopathy → IJ or EJ (compressible); avoid subclavian
- Emergency pacing → right IJ (most direct to RV)
- Trauma with cervical collar → femoral or subclavian
- OLV / thoracic surgery → avoid subclavian; avoid EJ (Barash 9e)
5. CVP Waveform — Normal Components
(Miller's Anaesthesia 10e — Table 32.3)
| Wave | Phase | Mechanical Event | ECG timing |
|---|---|---|---|
| a | End-diastole | Atrial contraction (atrial kick) | After P wave |
| c | Early systole | Tricuspid closure + isovolumic RV contraction | End QRS |
| x descent | Mid-systole | Atrial relaxation + annular descent | Before T wave |
| v | Late systole | Venous atrial filling (tricuspid still closed) | After T wave |
| y descent | Early diastole | Tricuspid opens; RA → RV filling | Before next P |
| h wave | Mid-diastole | Plateau (only at slow HR or high CVP) | — |
Mnemonic: atrial contraction → closure of tricuspid → exit (atrial relaxation) → venous filling → yield to ventricle

Read CVP at the base of the c wave at end-expiration
6. CVP Waveform Abnormalities
| Condition | Change | Mechanism |
|---|---|---|
| Atrial fibrillation | Loss of a wave | No organised atrial contraction |
| AV dissociation | Cannon a waves | Atrium contracts against closed tricuspid |
| Tricuspid regurgitation | Tall systolic c-v wave; loss of x descent | Regurgitant RA filling in systole |
| Tricuspid stenosis | Tall a wave; attenuated y descent | Impaired diastolic RA emptying |
| Cardiac tamponade | Dominant x descent; absent/attenuated y | Extrinsic compression; impaired diastolic filling |
| Pericardial constriction | Steep x AND y descents; M/W pattern | Exaggerated pressure equalisation |
| RV ischaemia / infarction | Tall a + v; steep x + y; M/W pattern | Reduced RV compliance |
7. Measurement — Practical Points
- Zero reference: 5 cm below sternal angle OR mid-thoracic level (phlebostatic axis)
- Always consistent levelling throughout monitoring period
- Measure at end-expiration (both spontaneous and PPV)
- PEEP artificially elevates CVP — factor this in
- Use ultrasound guidance (strongly recommended; mandatory for IJ per most guidelines) (Miller's 10e)
8. CVP and Fluid Responsiveness
CVP is a POOR predictor of fluid responsiveness. Multiple RCTs and systematic reviews confirm:
- No reliable relationship between CVP and circulating blood volume
- A single static CVP cannot predict haemodynamic response to a fluid bolus
- Guidelines recommend dynamic variables instead:
| Dynamic Variable | Method |
|---|---|
| Pulse pressure variation (PPV) | Arterial line |
| Stroke volume variation (SVV) | LiDCO / Vigileo |
| Passive leg raise (PLR) | Clinical |
| Oesophageal Doppler | Probe |
| Point-of-care echocardiography (POCUS) | TOE / TTE |
(Fishman's Pulmonary 5e; Miller's Anaesthesia 10e)
9. CVP in Shock
| Shock Type | Expected CVP |
|---|---|
| Hypovolaemic | ↓ Low |
| Distributive (sepsis, anaphylaxis) | ↓ Low |
| Cardiogenic (right heart failure) | ↑ High |
| Obstructive (tamponade, tension PTX, massive PE) | ↑ High |
10. Complications
Up to 15% of patients experience some adverse event. (Miller's 10e)
Mechanical
- Arterial puncture (1.9–15%) — most common acute complication
- Pneumothorax (↑ subclavian)
- Haemothorax / hydrothorax / chylothorax (L subclavian)
- Air embolism
- Catheter malposition, arrhythmias (guide wire in RV)
Thromboembolic
- DVT, PE, catheter-related thrombosis
Infectious
- CLABSI (central line-associated bloodstream infection)
- Prevention: chlorhexidine prep, maximal sterile barrier, insertion checklist, daily need review
11. Exam Summary — 10 High-Yield Facts
- CVP = RAP ≈ RV preload — not LV preload
- Normal: 2–8 mmHg; read at end-expiration, base of c wave
- Waveform: a, c, v peaks; x, y descents — timed against ECG
- Cannon a waves = AV dissociation; loss of a = AF; c-v fusion + no x = tricuspid regurgitation
- Tamponade: dominant x descent, absent y — Constriction: steep x AND y (M/W)
- CVP is a poor predictor of fluid responsiveness — dynamic variables preferred
- Right IJ = best site for pacing wires and PA catheters
- Subclavian = highest pneumothorax risk; avoid in emphysema and OLV
- EJ kinks in lateral decubitus — avoid for thoracotomy
- Always use ultrasound guidance; complications occur in up to 15% of insertions
Sources: Miller's Anaesthesia 10e; Barash, Cullen & Stoelting's Clinical Anaesthesia 9e; Fishman's Pulmonary Diseases and Disorders 5e; Morgan & Mikhail's Clinical Anaesthesiology 7e
This is a shared conversation. Sign in to Orris to start your own chat.