Typhoid fever
Reading File
Finding Sources
Searching PubMed
"typhoid fever"[MeSH Terms] AND treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I have comprehensive information. Let me now compile a thorough, well-organized answer.
Typhoid Fever (Enteric Fever)
Definition & Etiology
Typhoid fever — more precisely called enteric fever — is a severe systemic illness caused by Salmonella enterica serotype Typhi (S. Typhi) or, less commonly, S. Paratyphi A, B, or C. The original name "typhoid" reflected its clinical resemblance to typhus; in 1869 the term "enteric fever" was proposed to distinguish the two, but both names persist today.
- Harrison's Principles of Internal Medicine 22E, p. 1359
Epidemiology
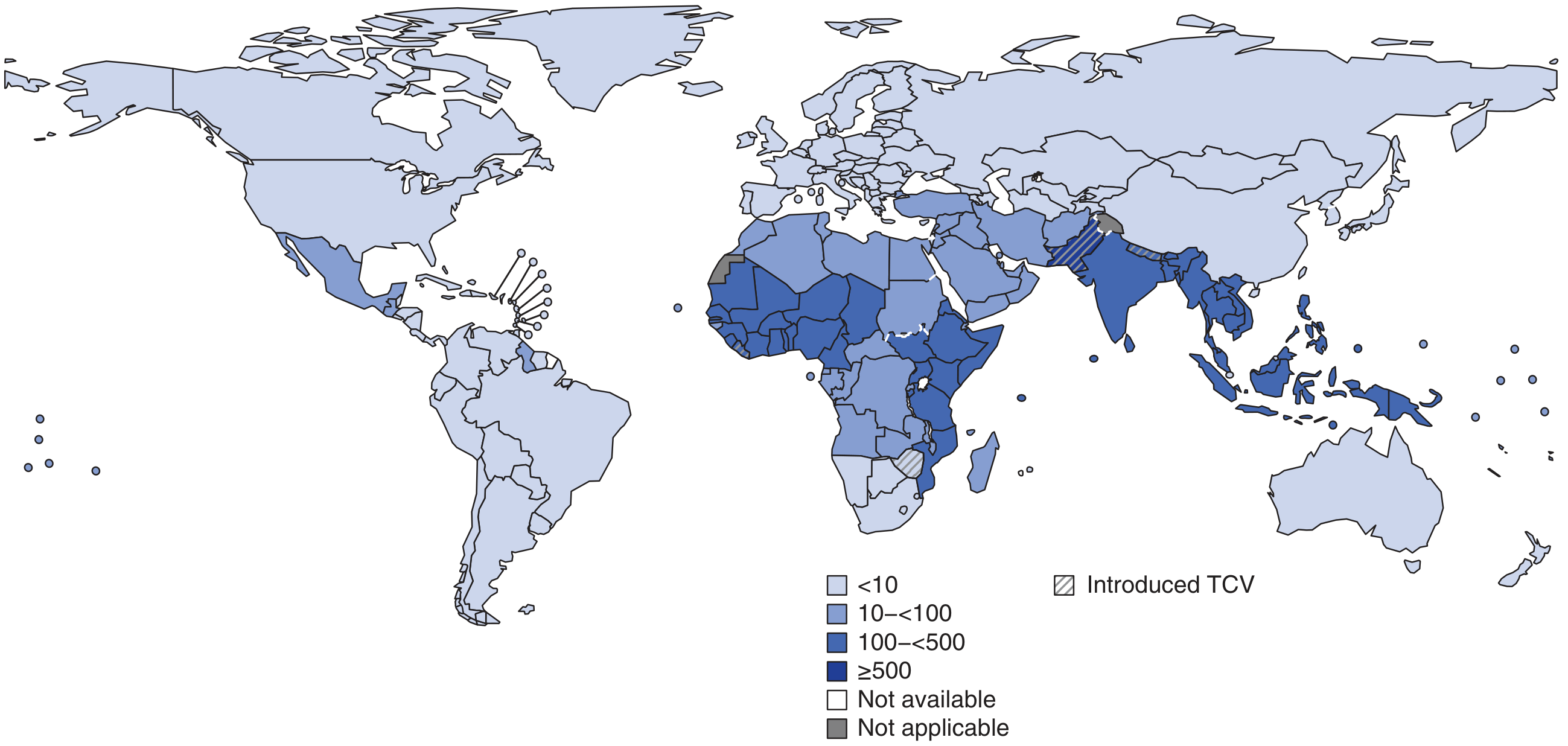
- ~9.2–21 million cases of typhoid and ~5 million cases of paratyphoid per year worldwide; 110,000–280,000 deaths annually
- Highest burden: Indian subcontinent (India, Pakistan, Bangladesh, Nepal), Eastern Mediterranean, and sub-Saharan Africa — exceeding 1,000 cases per 100,000 children in some urban areas
- Transmitted via fecally contaminated food or water; humans are the only reservoir for S. Typhi and S. Paratyphi
- Risk factors: contaminated drinking water, street food, raw vegetables fertilized with sewage, H. pylori infection (associated with reduced gastric acidity), lack of hand hygiene
In developed countries, the disease is rare and almost exclusively travel-associated (especially from the Indian subcontinent).
- Harrison's, p. 1359
Pathogenesis
After ingestion of contaminated food or water, S. Typhi:
- Reaches the small intestine, passes through the epithelium via M cells overlying Peyer's patches
- Enters intestinal lymphatics → spreads to the bloodstream
- Disseminates via bacteremia to bone marrow, liver, spleen, gallbladder, and other organs
- Multiplies within intestinal lymphoid tissue; excreted in stool
Pathological hallmarks:
-
Hyperplasia and necrosis of Peyer's patches → plateau-like elevations up to 8 cm → mucosal shedding → oval ulcers along the long axis of the ileum
-
Reactive hyperplasia of mesenteric lymph nodes
-
Typhoid nodules — small foci of parenchymal necrosis with macrophage aggregates in liver, bone marrow, and lymph nodes
-
Red pulp splenomegaly due to phagocyte hyperplasia
-
S. Typhi (unlike non-typhoidal Salmonella) can disseminate via lymphatic and blood vessels
-
Robbins & Kumar Basic Pathology, p. (block 6); Jawetz Medical Microbiology 28E, p. 252
Clinical Course
Incubation period: 10–14 days (range 5–21 days depending on inoculum size and host status)
Stepwise progression:
| Week | Features |
|---|---|
| Week 1 | Insidious onset: fever rising to 39–40.5°C, headache (80%), chills (35–45%), malaise, dry cough (30%), myalgias, anorexia (55%), constipation or diarrhea |
| Week 2 | Sustained high plateau fever; rose spots appear; relative bradycardia; hepatosplenomegaly; "coated tongue" (51–56%); leukopenia |
| Week 3–4 | Risk of intestinal hemorrhage and perforation; "muttering delirium" / neuropsychiatric symptoms; prostration |
Key physical findings:
- "Rose spots" — faint, salmon-colored, blanching maculopapular rash on trunk/chest; present in ~30% at end of week 1; resolve in 2–5 days; easier to detect in lightly pigmented patients
- Relative bradycardia — pulse slower than expected for the degree of fever (Faget's sign); present in <50%
- Hepatosplenomegaly — occurs in 3–6% on presentation, increases over time
- Leukopenia/neutropenia — in 15–25% (contrast to other bacterial sepsis); leukocytosis can occur in children or with perforation
Note: Abdominal pain is present in only 30–40% despite the name "enteric fever." Fever is the universal feature (>75%).
- Harrison's, p. 1360; Tintinalli's Emergency Medicine, p. (block 13)
Complications (~27% of hospitalized patients)
| Complication | Details |
|---|---|
| Intestinal perforation (~1%) | Weeks 3–4; life-threatening; requires surgery + broad-spectrum antibiotics for peritonitis |
| GI hemorrhage (~6%) | From ulcerated Peyer's patches; may require transfusion or bowel resection |
| Neurologic (2–40%) | Meningitis, Guillain-Barré syndrome, neuritis, "muttering delirium," toxic encephalopathy |
| Hepatitis | Moderately elevated LFTs common |
| Myocarditis / Endocarditis | Rare but serious |
| Hemophagocytic syndrome (HLH) | Recognized increasingly (PMID 38579699) |
| Relapse | ~10% of patients; within 2–3 weeks of resolution; same strain and susceptibility |
| Chronic carrier state | 2–5%; S. Typhi shed in stool/urine >1 year; associated with gallstone biofilm; increased risk of gallbladder cancer |
Untreated mortality: 10–20%. With appropriate antibiotics: <1%.
Diagnosis
Gold standard: Blood culture (positive in 40–80% week 1–2; 90% of cultures positive during febrile phase per some series). Bone marrow culture is the most sensitive test and remains positive even after antibiotics have been started.
| Test | Details |
|---|---|
| Blood culture | Best weeks 1–2; 40–80% sensitivity |
| Stool culture | Positive from week 2 onward |
| Urine culture | Positive from week 2–3 |
| Bone marrow culture | Most sensitive (~90%); positive even post-antibiotics |
| Widal test | Unreliable (false positives in endemic areas); not recommended as sole diagnostic test |
| Rapid antigen tests | Increasingly used; variable sensitivity |
No other specific laboratory test confirms enteric fever definitively.
Treatment
Antibiotic therapy
Current recommendations account for increasing drug resistance:
| Drug | Route | Use |
|---|---|---|
| Ceftriaxone | IV | Severe disease; first-line for hospitalized patients |
| Azithromycin | Oral | Uncomplicated disease; first-line for outpatients |
| Cefixime | Oral | Alternative oral option for uncomplicated disease |
| Ciprofloxacin | Oral/IV | Only if confirmed susceptible; avoid empirically due to widespread resistance |
| Chloramphenicol, Ampicillin, TMP-SMX | — | Largely unreliable due to resistance |
Duration: 7–14 days depending on severity; 10–14 days typical for systemic disease.
Dexamethasone: Add for severe typhoid meningitis/encephalitis or shock.
Drug resistance — critical update:
- MDR strains (resistant to chloramphenicol, ampicillin, TMP-SMX) emerged in the 1980s
- Fluoroquinolone-resistant / decreased susceptibility strains common from Indian subcontinent — treat as resistant even if disk diffusion appears susceptible (use MIC testing)
- XDR (extensively drug-resistant) S. Typhi — emerged in Pakistan 2016, resistant to all first-line + fluoroquinolones + third-generation cephalosporins; only azithromycin and carbapenems remain active
- A 2024 systematic review (PMID 39623850) confirmed azithromycin's clinical efficacy vs. comparators across all age groups
Supportive care:
- IV rehydration
- Blood transfusion if significant GI losses
- Surgical intervention for perforation or uncontrolled hemorrhage
Prevention
Vaccines (two available):
| Vaccine | Type | Route | Efficacy | Duration | Notes |
|---|---|---|---|---|---|
| Ty21a (Vivotif) | Live attenuated oral | Oral | ~50–80% | 5 years | Ages ≥6 years; 3–4 capsules over 1 week |
| Vi polysaccharide (Typhim Vi) | Parenteral polysaccharide | IM | ~50–70% | 2–3 years | Ages ≥2 years |
| Typhoid conjugate vaccine (TCV) | Vi-conjugated | IM | ~80% | Longer | Ages ≥6 months; WHO-recommended; single dose |
A 2025 meta-analysis (PMID 41125003) confirmed real-world TCV effectiveness of ~80% in children and adolescents, supporting WHO's recommendation for endemic country programs.
Other measures:
- Safe water and food handling
- Proper sewage treatment
- Hand hygiene
- Treat chronic carriers (prolonged antibiotics ± cholecystectomy if gallstones present)
Salmonella Disease Comparison (Jawetz Table 15-4)
| Feature | Enteric Fever | Septicemia | Enterocolitis |
|---|---|---|---|
| Incubation | 7–20 days | Variable | 8–48 hours |
| Onset | Insidious | Abrupt | Abrupt |
| Fever | Gradual plateau; "typhoidal state" | Rapid spiking; "septic" | Usually low |
| Duration | Several weeks | Variable | 2–5 days |
| GI symptoms | Constipation early; bloody diarrhea later | Often none | Nausea, vomiting, diarrhea at onset |
| Blood culture | Positive weeks 1–2 | Positive during high fever | Negative |
| Stool culture | Positive from week 2 | Infrequently positive | Positive soon after onset |
Sources:
- Harrison's Principles of Internal Medicine 22E (2025), Ch. 171
- Tintinalli's Emergency Medicine: A Comprehensive Study, Ch. 162
- Robbins & Kumar Basic Pathology, Ch. 13
- Jawetz, Melnick & Adelberg's Medical Microbiology 28E, Ch. 15
- Uzair M et al. (2024) — Azithromycin vs. other antimicrobials in typhoid [PMID 39623850]
- Haposan JH et al. (2025) — TCV real-world effectiveness [PMID 41125003]
This is a shared conversation. Sign in to Orris to start your own chat.