Ventricular depolarization.
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
I now have comprehensive, well-sourced content. Here is the complete answer on ventricular depolarization:
Ventricular Depolarization
Overview
Ventricular depolarization is the electrical process by which the resting membrane potential of ventricular myocytes rapidly reverses, triggering the mechanical contraction of the ventricles. On the ECG, it is represented by the QRS complex (normally ≤0.09-0.10 s). The process is fast, coordinated, and depends entirely on the specialized His-Purkinje conduction system.
1. The Conduction System - Getting the Impulse to the Ventricles
The SA node fires at 60-100 times/min. The impulse travels across both atria, reaching the AV node in about 0.04 s, then is delayed for another 0.11 s within the AV node due to its slowly-conducting, calcium-channel-dependent small fibers. This AV nodal delay is physiologically important: it allows atrial contraction to complete and fill the ventricles before ventricular contraction begins.
The lower AV nodal fibers merge to form the bundle of His, which passes into the interventricular septum before splitting into:
- Right bundle branch (RBB) - runs along the right side of the interventricular septum
- Left bundle branch (LBB) - fans out over the left ventricular septum, functionally organized into anterior and posterior fascicles
These branches terminate in a dense network of Purkinje fibers covering virtually the entire endocardial surface of both ventricles.
(Morgan and Mikhail's Clinical Anesthesiology, 7e, pp. 644-645)
2. The Ionic Basis of Ventricular Depolarization
Unlike the SA and AV nodes (which rely primarily on slow L-type Ca²+ channels), ventricular myocytes and Purkinje fibers depolarize via fast voltage-gated Na⁺ channels. When the membrane threshold is reached (~-70 mV), fast Na⁺ channels open, producing a rapid phase-0 upstroke of the action potential. This results in extremely fast conduction velocities in the His-Purkinje system (the fastest in the heart), enabling near-simultaneous activation of the entire ventricular endocardium.
The ventricular action potential has 5 phases:
- Phase 0: Rapid depolarization - fast Na⁺ influx
- Phase 1: Rapid early repolarization - Na⁺ channels inactivate; transient outward K⁺ current
- Phase 2: Plateau - L-type Ca²+ influx balanced by K⁺ efflux (this Ca²+ triggers myofilament contraction)
- Phase 3: Rapid repolarization - delayed rectifier K⁺ channels dominate
- Phase 4: Stable resting membrane potential (~-90 mV) - unlike nodal cells, ventricular myocytes do not spontaneously depolarize under normal conditions
(Katzung's Basic and Clinical Pharmacology, 16e; Morgan & Mikhail, 7e)
3. Sequence of Ventricular Activation
The spread of depolarization follows a precise, reproducible order:
| Step | Region Activated | Direction |
|---|---|---|
| 1 | Interventricular septum (left-to-right side) | Left → Right |
| 2 | Endocardium of both ventricles nearly simultaneously | Base → Apex |
| 3 | Ventricular myocardium proper | Endocardium → Epicardium |
| 4 | Base of ventricles and posterior wall (last to depolarize) | Apex → Base |
Key points:
- Septal activation comes first: The left bundle branch activates the left side of the septum slightly before the right bundle activates the right side, so the initial depolarization vector is directed right and anteriorly. This inscribes the small "septal q" wave visible in leads I, aVL, V5, V6.
- His-Purkinje fibers transmit the impulse almost simultaneously to both endocardial surfaces - this is why normal QRS duration is narrow (< 0.10 s).
- Spread from endocardium to epicardium: Once the Purkinje fibers deliver the impulse to the subendocardium, it travels through working myocardium cell-to-cell via gap junctions outward toward the epicardium.
- The left ventricle dominates the QRS vector because its myocardial mass greatly exceeds that of the right ventricle.
- The net depolarization vector therefore points inferiorly, leftward, and posteriorly - yielding a positive QRS in leads I, II, aVF, and V4-V6, and the characteristic R-wave progression across the precordium.
(Goldman-Cecil Medicine, ELECTROCARDIOGRAPHIC LEADS; Braunwald's Heart Disease, Terminal Purkinje Fibers)
4. Purkinje Fiber Architecture and Its Clinical Importance
Braunwald's Heart Disease details that Purkinje fibers:
- Cover most of the endocardium of both ventricles
- Are less concentrated at the base and papillary muscle tips
- In humans, penetrate only the inner third of the endocardium (unlike pigs, where they almost reach the epicardium)
- Action potentials propagate from base to apex within Purkinje bundles before activating surrounding myocytes
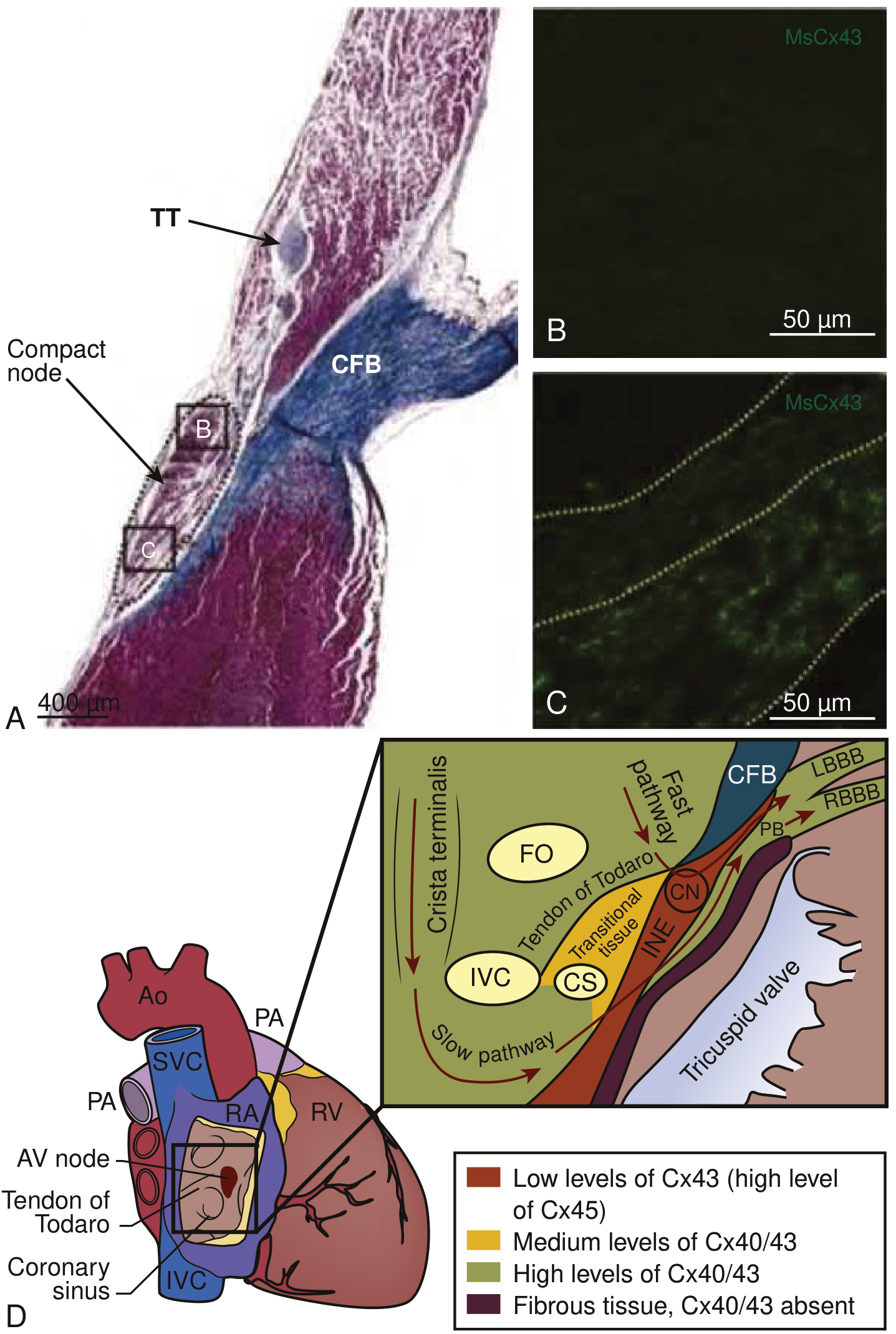
- Rely on connexins 40 and 45 (not Cx43 which dominates working myocardium)
- Have markedly longer repolarization times than surrounding myocytes - a key factor in ventricular arrhythmia substrate
(Braunwald's Heart Disease, 2-Vol Set, Terminal Purkinje Fibers)
5. ECG Correlates
| ECG Waveform | Corresponds to |
|---|---|
| P wave | Atrial depolarization |
| QRS complex | Ventricular depolarization |
| ST segment | Ventricular muscle uniformly depolarized (plateau phase) |
| T wave | Ventricular repolarization |
- Q wave: Small initial deflection; reflects septal depolarization (left → right)
- R wave: Large positive deflection; the main left ventricular depolarization moving toward the exploring electrode in lateral leads
- S wave: Terminal depolarization moving away (toward the base/posterobasal wall)
- Normal QRS duration: ≤0.09 s (≥0.12 s = abnormal, suggesting bundle branch block or ventricular pacing)
- When the His-Purkinje system fails (bundle branch block), the impulse spreads cell-to-cell via gap junctions - this is slow and inefficient, producing a wide QRS (≥0.12 s)
(The Harriet Lane Handbook, 23e; Rosen's Emergency Medicine; Guyton and Hall Textbook of Medical Physiology)
6. When Ventricular Depolarization Goes Wrong
- Bundle branch block: Failure of one bundle branch forces the affected ventricle to depolarize slowly from the other side - produces wide QRS and altered vector
- Wolff-Parkinson-White (WPW): An accessory pathway (bundle of Kent) bypasses the AV node, inserting directly into ventricular muscle. Depolarization spreads slowly cell-to-cell (not via Purkinje), producing a delta wave and short PR interval
- Premature ventricular contraction (PVC): Ectopic focus in ventricular muscle fires spontaneously; spreads cell-to-cell, producing a wide, bizarre QRS
- Ventricular fibrillation: Completely disorganized, chaotic depolarization with no coordinated QRS - electrically or mechanically lethal
(Medical Physiology, Boron & Boulpaep; Symptom to Diagnosis, 4e)
Summary: Ventricular depolarization is an exquisitely organized electrical cascade. The AV node delays the impulse, the His-Purkinje system rapidly distributes it to the entire endocardium within milliseconds, and depolarization then sweeps from endocardium to epicardium and from apex to base. The resulting net vector - leftward, inferior, and posterior - is the QRS complex on the ECG. Any disruption of this sequence, whether at the bundle branch level or the working myocardium, widens and distorts the QRS.
This is a shared conversation. Sign in to Orris to start your own chat.