Male genital infections with pictures
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
I now have comprehensive content and all the images. Let me compile the full educational response.
Male Genital Infections
A structured overview from authoritative medical textbooks (Fitzpatrick's Dermatology, Robbins & Kumar Basic Pathology, Sabiston Textbook of Surgery, Textbook of Family Medicine).
1. Gonorrhea (Neisseria gonorrhoeae)
Pathogen: Gram-negative diplococcus, typically visualized intracellularly within PMNs.
Mechanism: The bacteria attach to columnar/transitional mucosal epithelium via pili and membrane adhesion molecules, then penetrate deeper tissues. In males this causes urethritis.
Clinical Features in Men:
- Incubation: 2-8 days (rarely beyond 2 weeks)
- ~90% of cases are symptomatic in men
- Spontaneous, profuse, purulent urethral discharge from the penile meatus
- Dysuria, meatal erythema and swelling
- "Bull head clap" - marked swelling of the entire distal shaft due to urethral inflammation
- Ascending infection can cause epididymitis, prostatitis, orchitis
- Untreated: urethral stricture, sterility, chronic carrier state
Microbiology image - Gram stain of urethral discharge:
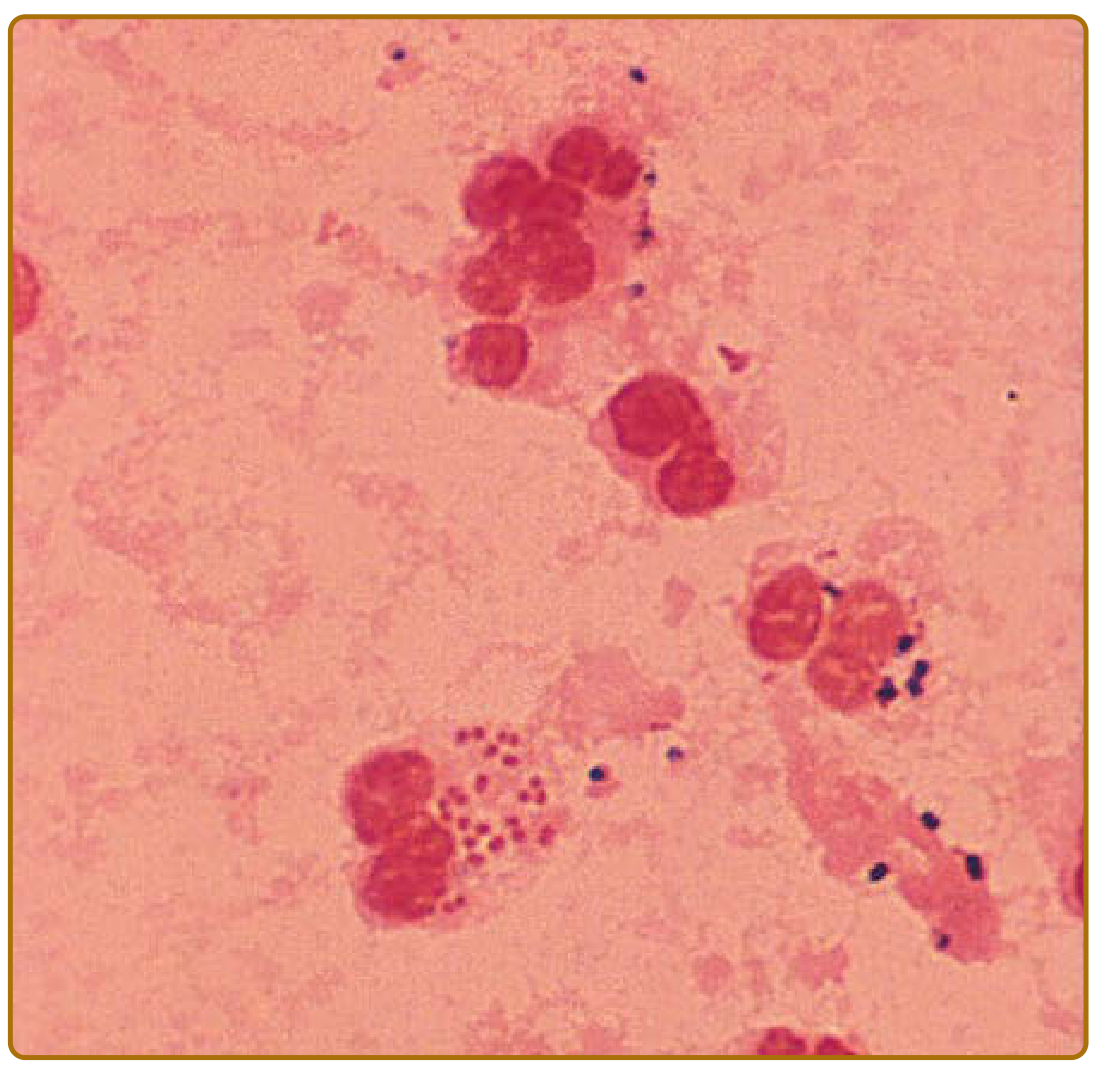
Figure: Diagnostic Gram-stained smear of urethral discharge in acute gonorrhea. Gonococci (red) within a polymorphonuclear leukocyte - also gram-positive cocci visible (dark blue). - Fitzpatrick's Dermatology
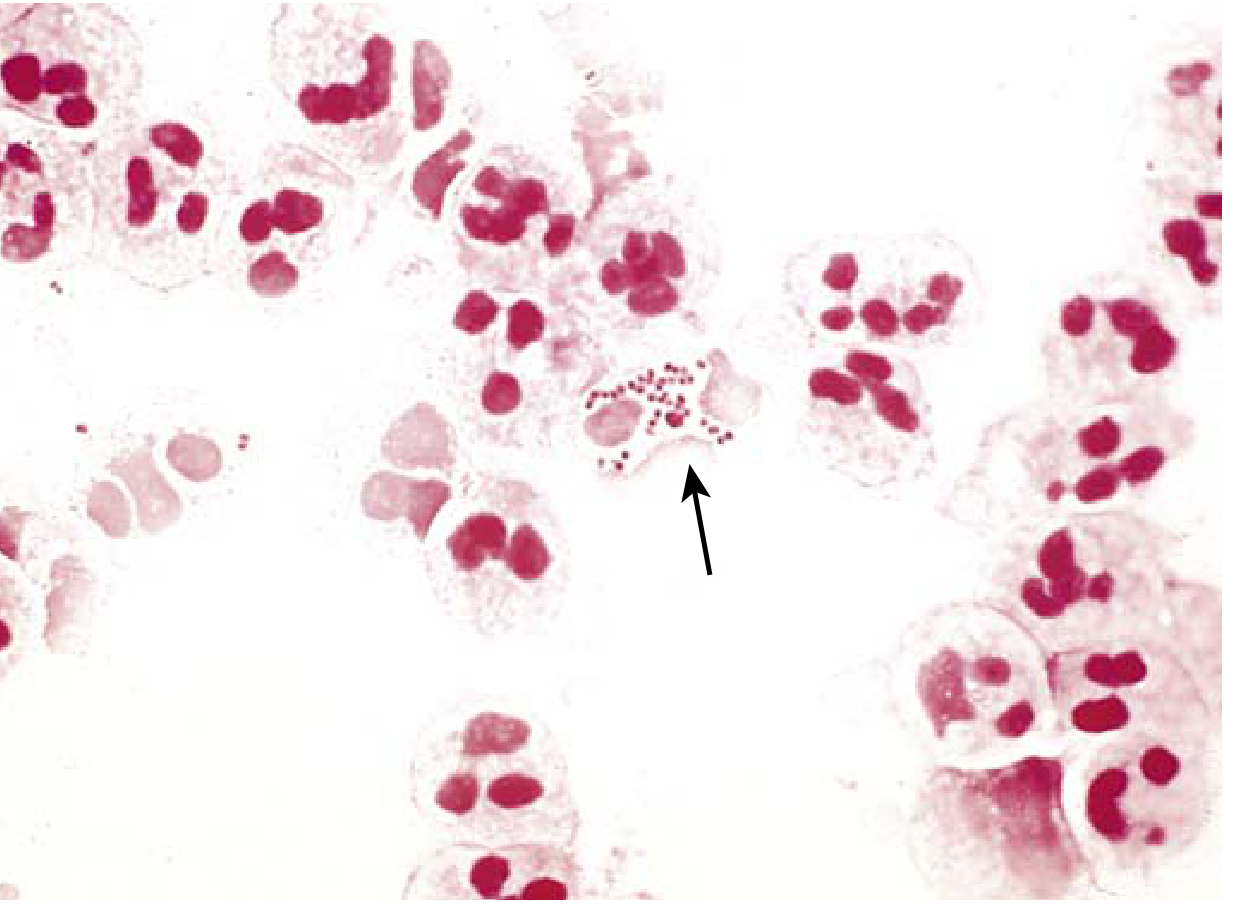
Figure: N. gonorrhoeae Gram stain - characteristic gram-negative, intracellular diplococci (arrow). - Robbins & Kumar Basic Pathology
Clinical photo - Acute gonorrhea with purulent discharge:
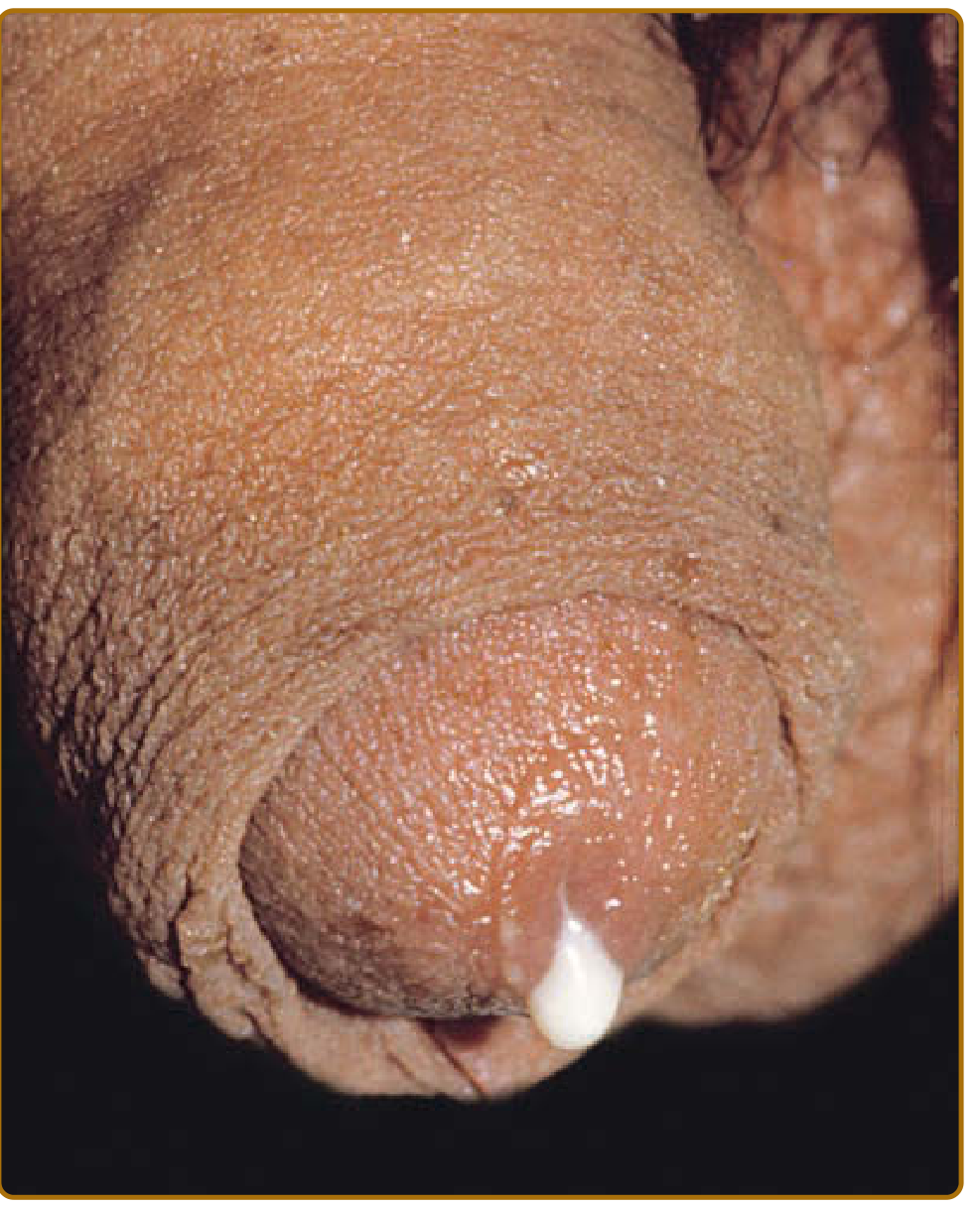
Figure: Acute gonorrhea - creamy purulent urethral discharge in an uncircumcised male. - Fitzpatrick's Dermatology
Clinical photo - Purulent discharge with glans/prepuce inflammation:

Figure: Acute gonorrhea - purulent urethral discharge with concomitant inflammation of the prepuce and glans. - Fitzpatrick's Dermatology
Clinical photo - "Bull head clap":

Figure: "Bull head clap" - swelling of the entire distal shaft, a manifestation of urethral gonococcal infection. - Fitzpatrick's Dermatology
Pathology specimen - Gonococcal epididymitis:

Figure: Gonococcal epididymitis - cross-section shows large area of purulent exudate within the epididymis. - Robbins & Kumar
Disseminated Gonococcal Infection (DGI): Occurs in 0.5-3% of cases. Classic triad = dermatitis + migratory polyarthritis + tenosynovitis. Skin lesions are hemorrhagic vesicopustules on an erythematous base.
Treatment: Dual therapy per current guidelines - typically ceftriaxone IM + azithromycin (due to emerging resistance).
2. Syphilis (Treponema pallidum)
Pathogen: Delicate spiral spirochete, 5-20 μm, with characteristic corkscrew motility. Cannot be cultured in vitro. Enters through skin or mucous membranes.
Transmission risk: 16-30% per sexual contact with an infected partner in the previous 30 days.
| Stage | Features |
|---|---|
| Primary | Painless, indurated ulcer (chancre) with well-defined borders and a clean base. Appears 2-6 weeks post-exposure on genital mucosa (also oral/anorectal). |
| Secondary | Disseminated disease - fever, generalized lymphadenopathy, headache, sore throat, rash. Affects CNS, eyes, liver, kidneys. RPR 99% sensitive. |
| Latent | Reactive serology without clinical signs. Early (<1 yr) vs. late. |
| Tertiary | Cardiovascular (aortic aneurysm, aortic regurgitation), neurologic (tabes dorsalis, general paresis, gumma). Earned title "the great masquerader." |
Diagnosis:
- Primary: Darkfield microscopy or direct immunofluorescence of chancre exudate
- Non-treponemal tests: RPR (for serum), VDRL (for CSF)
- Treponemal tests: MHA-TP (confirmatory)
- Coinfection with HIV complicates diagnosis and treatment
Treatment:
- Benzathine penicillin G is the treatment of choice for all stages in non-penicillin-allergic patients
- Early syphilis: single IM dose
- Late/neurosyphilis: high-dose IV penicillin G
- Chancroid (caused by Haemophilus ducreyi) mimics primary syphilis but produces a soft, painful ulcer vs. syphilis's hard, painless chancre
3. Epididymitis-Orchitis
Pathophysiology: UTI ascends via the vas deferens into the epididymis or testicle. Age-related causative organisms:
| Age Group | Common Organism |
|---|---|
| < 35 years | Chlamydia trachomatis (STI source) |
| > 35 years | Escherichia coli (gram-negative enteric) |
Clinical Features:
- Significant scrotal swelling and tenderness
- May be difficult to distinguish from testicular torsion, incarcerated hernia, or testicular tumor
- Scrotal ultrasound (Doppler) is key to rule out associated abscess and assess blood flow
Management:
- Without abscess: antibiotics, rest, scrotal elevation
- With abscess: surgical drainage + often orchiectomy
- Persistent ischemia on Doppler imaging warrants exploration
4. Prostatitis (Acute Bacterial)
Pathogen: Most commonly gram-negative bacteria; secondary to ascending UTI.
Key Points:
- Avoid vigorous digital rectal examination (DRE) - pressure on an infected prostate can cause hematogenous bacterial dissemination
- Patients not improving promptly should be evaluated for prostatic abscess (does not respond to antibiotics alone)
- Treatment: transurethral unroofing or percutaneous drainage for abscess
5. Genital Herpes (Herpes Simplex Virus)
Pathogen: HSV-2 causes most cases of genital herpes; however HSV-1 is increasingly responsible. Approximately 1 in 8 persons aged 14-49 in the US is infected with HSV-2.
Primary Infection - Signs in Men:
- Incubation: 2-12 days
- Painful erythematous vesicles on mucosa/skin of lower genitalia
- Dysuria, urethral discharge, tender inguinal lymphadenopathy
- Systemic symptoms: fever, myalgia, headache
- Active viral shedding continues until all mucosal lesions heal; asymptomatic shedding can persist up to 3 months after diagnosis
Histology: Intraepithelial vesicles with necrotic debris, neutrophils, and characteristic Cowdry type A intranuclear inclusions (light purple, homogeneous, surrounded by clear halo). Infected cells form multinucleate syncytia.
Recurrences: Milder and shorter than primary episode. Virus latent in dorsal root ganglia between outbreaks.
Treatment: Acyclovir, valacyclovir, or famciclovir (antiviral therapy shortens duration and reduces shedding).
6. Genital Warts - Condyloma Acuminata (HPV)
Pathogen: Human papillomavirus (HPV) types 6 and 11 (low-risk; not oncogenic) cause condylomata acuminata.
Features: Soft, flesh-colored, cauliflower-like papillomas on the penis, perianal area, and scrotum. HPV types 16 and 18 (high-risk) can cause penile carcinoma.
Treatment: Topical agents (imiquimod, podophyllin), cryotherapy, laser ablation, or surgical excision. Prevention: HPV vaccine (covers types 6, 11, 16, 18).
7. Fournier Gangrene (Necrotizing Fasciitis of the Genitalia)
A urologic emergency - polymicrobial necrotizing infection of the male genital and perineal skin and subcutaneous tissues.
Microbiology: Polymicrobial - microaerobes, anaerobes, gram-positive and gram-negative organisms acting synergistically.
Risk Factors: Diabetes mellitus, peripheral vascular disease, malnutrition, alcoholism, immunocompromised states.
Clinical Presentation:
- Severe genital/scrotal pain and swelling
- Skin discoloration or frank necrosis
- Crepitus (gas-producing organisms)
- Foul-smelling discharge
Important anatomy: The infection rarely involves the testes (protected by tunica vaginalis) or deep penile structures (protected by Buck's fascia) - these should be preserved during debridement.
Treatment: Surgical emergency requiring:
- Urgent wide surgical debridement of all necrotic tissue
- Broad-spectrum IV antibiotics (polymicrobial coverage)
- ICU-level supportive care
- Delayed skin grafting for wound coverage
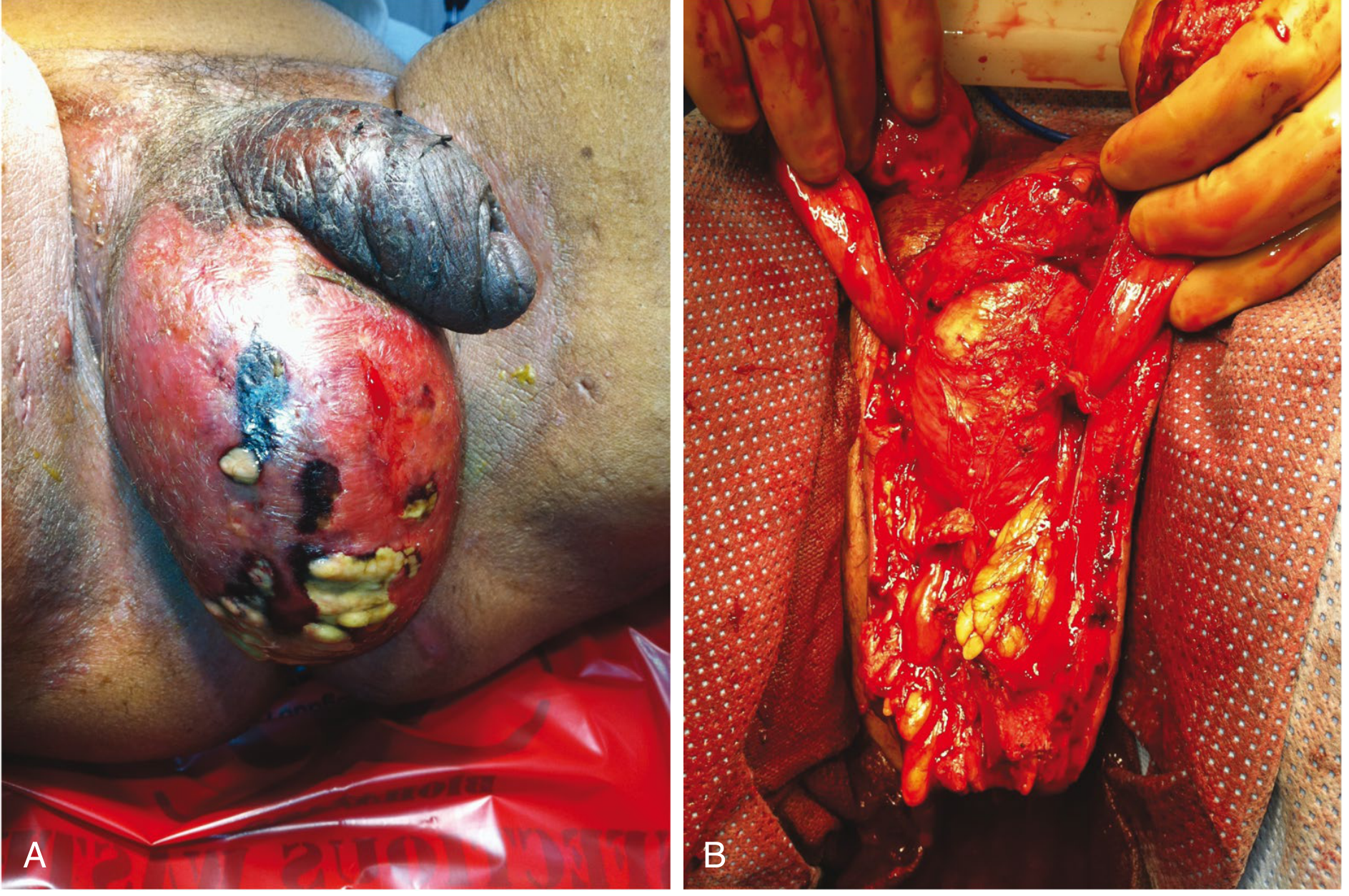
Figure: Fournier gangrene. (A) Skin necrosis, purulence, and edema of the scrotum. (B) Appearance after extensive debridement - the base of the penis is visible centrally; the testes are elevated and spermatic cords visible anteriorly. - Sabiston Textbook of Surgery
8. Genitourinary Tuberculosis
Route: Hematogenous spread from pulmonary TB to the GU tract (3rd most common extrapulmonary site).
Manifestations in Men:
- Voiding symptoms, sterile pyuria, hematuria
- Chronic epididymitis or epididymal mass
- Ureteral strictures (antegrade spread)
Diagnosis: Acid-fast bacilli (AFB) smears of urine, mycobacterial culture with sterile pyuria, chest X-ray, GU imaging.
Treatment: 2 months of 4-drug regimen (HRZE), then 7 months of isoniazid + rifampin. Infectious disease consultation mandatory (public health implications).
Summary Table
| Infection | Pathogen | Key Feature | Treatment |
|---|---|---|---|
| Gonorrhea | N. gonorrhoeae | Purulent urethral discharge | Ceftriaxone + azithromycin |
| Syphilis (primary) | T. pallidum | Painless chancre | Benzathine penicillin G |
| Chancroid | H. ducreyi | Soft, painful ulcer | Azithromycin or ceftriaxone |
| Genital Herpes | HSV-1/2 | Painful vesicles | Acyclovir/valacyclovir |
| Genital Warts | HPV 6/11 | Cauliflower papillomas | Imiquimod, cryotherapy |
| Epididymitis-orchitis | Chlamydia (<35 yr), E. coli (>35 yr) | Scrotal swelling, tenderness | Age-appropriate antibiotics |
| Fournier Gangrene | Polymicrobial | Scrotal necrosis + crepitus | Emergency debridement + IV ABX |
| GU Tuberculosis | M. tuberculosis | Sterile pyuria, epididymal mass | HRZE 2mo + HR 7mo |
Sources: Fitzpatrick's Dermatology (Editors Vol 1 & 2); Robbins & Kumar Basic Pathology; Sabiston Textbook of Surgery; Textbook of Family Medicine 9e; Robbins & Kumar Basic Pathology
Normal fungal infections
Asking for Preferences
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
I now have all the content and images needed for a comprehensive response.
Common (Superficial) Fungal Infections
Superficial fungal infections are among the most prevalent infections worldwide, caused primarily by dermatophytes (tinea), Candida species, and Malassezia species. They infect the skin, hair, nails, and mucous membranes in immunocompetent individuals.
Overview: The Three Main Culprits
| Group | Organisms | Infects |
|---|---|---|
| Dermatophytes | Trichophyton, Microsporum, Epidermophyton | Keratinized tissue: skin, hair, nails |
| Candida | C. albicans (mainly) | Mucosa, moist skin folds, nails |
| Malassezia | M. globosa, M. furfur | Sebaceous skin (trunk, scalp) |
PART 1: DERMATOPHYTOSES (Tinea)
Dermatophytes digest keratin using keratinases and are classified by their host origin:
- Anthropophilic - human to human (e.g., T. rubrum, T. tonsurans)
- Zoophilic - animal to human (e.g., M. canis from cats/dogs, T. verrucosum from cattle)
- Geophilic - soil origin (e.g., M. gypseum)
Diagnosis for all tinea: KOH preparation of skin scrapings showing branching hyphae; fungal culture on Sabouraud's medium; Wood's lamp (some fluoresce green).
1. Tinea Corporis ("Ringworm")
Dermatophytosis of glabrous skin (excluding scalp, beard, hands, feet, groin).
Clinical Features:
- Classic annular ("ringworm") plaque with a raised, scaly, erythematous advancing border
- Progressive central clearing produces concentric rings
- Border may be vesicular; center may be clear or scaly
- Widespread disease can be a sign of HIV/AIDS or topical steroid use
Common pathogens: T. rubrum, M. canis, T. mentagrophytes
Tinea gladiatorum - common in wrestlers, typically caused by T. tonsurans, affects head, neck, and arms.
Majocchi granuloma - deeper follicular infection, presents as scaly follicular papules and nodules in an annular arrangement; most common on legs of women who shave.

Figure: Tinea corporis - classic annular polycyclic plaques with raised erythematous scaling borders. - Fitzpatrick's Dermatology
Treatment: Topical antifungals for 2-4 weeks (terbinafine, clotrimazole, miconazole, ketoconazole). Oral agents (griseofulvin, terbinafine, itraconazole) for widespread or follicular disease. Avoid combination products with potent corticosteroids (e.g., clotrimazole/betamethasone) - they cause widespread spread and fungal folliculitis.
Differential Diagnosis: Erythema annulare centrifugum, nummular eczema, psoriasis, pityriasis rosea, secondary syphilis, subacute cutaneous lupus.
2. Tinea Cruris ("Jock Itch")
Dermatophytosis of the groin, genitalia, pubic area, perineal, and perianal skin. Second most common dermatophytosis worldwide. 3x more common in men than women.
Risk Factors: Occlusion, humidity, sweating; autoinoculation from tinea pedis (wear socks before underwear to prevent self-reinfection).
Clinical Features:
- Well-demarcated annular plaque with raised, scaly border extending from inguinal fold to inner thigh - often bilateral
- Pruritus common; pain when macerated
- E. floccosum infection: central clearing with genitocrural fold involvement
- T. rubrum infection: confluent extension to pubic, perianal, buttock, and lower abdominal areas
- Genitalia and scrotum are spared (distinguishes from candidal intertrigo, where scrotum is involved)
Common pathogens: T. rubrum, E. floccosum

Figure: Tinea cruris - annular erythematous plaques with raised scaling border expanding from the inguinal folds to the inner thighs and pubic region. - Fitzpatrick's Dermatology
Treatment: Same as tinea corporis. Address coexisting tinea pedis to prevent reinfection.
Differential: Erythrasma (coral-red fluorescence on Wood's lamp), candidal intertrigo (involves scrotum), inverse psoriasis, contact dermatitis, seborrheic dermatitis.
3. Tinea Pedis ("Athlete's Foot")
The most common dermatophytosis (prevalence ~10%). Caused predominantly by T. rubrum and zoophilic T. interdigitale.
Three major clinical patterns:
| Type | Features |
|---|---|
| Interdigital (most common) | Scaling, erythema, maceration between lateral toes (4th-5th most common); bacterial coinfection (Pseudomonas, Staph) produces pruritus and malodor = "athlete's foot" |
| Chronic hyperkeratotic (Moccasin) | Diffuse scaling on the sole and lateral/medial foot in a moccasin distribution; most common pathogen T. rubrum |
| Vesiculobullous | Tense vesicles/bullae on soles and periplantar areas; caused by zoophilic T. interdigitale |

Figure: Tinea pedis (moccasin type) - large red scaly rash covering the sole and side of the foot. - Fitzpatrick's Dermatology
"Two feet - one hand" syndrome: Tinea pedis (both feet) + tinea manus (one hand, from scratching infected feet) - a classic presentation.
Treatment: Topical antifungals; occlusive footwear correction; oral terbinafine for widespread/resistant cases.
4. Tinea Capitis
Dermatophyte infection of the scalp and hair - primarily in children aged 3-14 years. Fungistatic fatty acids in adult sebum explain why incidence drops sharply after puberty.
Clinical Subtypes:
| Type | Features | Pathogen |
|---|---|---|
| Gray patch (noninflammatory) | Circular scaly patches with alopecia; hairs break off just above scalp leaving gray appearance; Wood's lamp green fluorescence | M. audouinii, M. ferrugineum |
| Black dot | Hairs broken at scalp surface leave black dots; polygonal alopecia patches | T. tonsurans, T. violaceum (endothrix) |
| Kerion | Boggy, crusted, suppurating, painful mass with sinus tracts; can cause scarring alopecia | Zoophilic organisms |
| Favus | Yellow cup-shaped crusts (scutula) in follicles; musky odor; slow-progressive scarring alopecia; seen in Africa/Middle East | T. schoenleinii |
Treatment: Systemic antifungals required (topical ineffective for scalp): Griseofulvin is first-line in children; terbinafine and itraconazole are alternatives.
5. Tinea Barbae (Beard Ringworm)
Dermatophytosis of the beard area in males; incidence has decreased with improved barber sanitation; now more common in farmers/ranchers via direct contact with cattle, horses, or dogs.
Two forms:
Superficial type - caused by anthropophilic T. violaceum; resembles bacterial folliculitis with perifollicular papules and pustules; alopecia is reversible.
Inflammatory type (kerion) - caused by zoophilic T. interdigitale or T. verrucosum; boggy-crusted plaques with seropurulent discharge; brittle, easily epilated hairs; may form abscess-like collections, sinus tracts, and scarring alopecia.

Figure: Tinea barbae. (A) Superficial type - scattered follicular papules/pustules, easily mistaken for Staph folliculitis. (B) Kerion type - sharply demarcated red edematous nodule with weeping pustules and hair loss. - Fitzpatrick's Dermatology
Differential: Bacterial folliculitis (sycosis vulgaris), pseudofolliculitis barbae, acne, herpes simplex.
Treatment: Systemic antifungals (oral terbinafine or itraconazole).
PART 2: CANDIDIASIS
Pathogen: Candida albicans is a commensal of the GI tract, genitourinary tract, and skin in >40% of healthy adults. It converts to a pathogen when local or systemic conditions favor overgrowth.
Predisposing Factors:
- Warmth and moisture (intertriginous areas)
- Antibiotics (reduces competing flora)
- Diabetes mellitus
- Obesity
- Immunosuppression (steroids, HIV)
- Extremes of age
Diagnosis: KOH prep shows budding yeast and pseudohyphae (Candida runs vertically unlike dermatophytes which run parallel); PAS stain highlights both; Gram stain shows gram-positive ovoid bodies 2-5 μm.
Cutaneous Candidiasis (Candidal Intertrigo)
Classic appearance: Beefy-red patches and plaques with satellite papules and pustules at the periphery.

Figure: Typical cutaneous candidiasis - erythematous papules coalescing into confluent plaques with characteristic satellite vesiculopustules. - Fitzpatrick's Dermatology
Sites: Axillae, inframammary folds, inguinal/genitocrural folds, abdominal creases, interdigital spaces, diaper area.
Key difference from tinea cruris: Candidal intertrigo involves the scrotum, whereas tinea cruris typically spares it.
Oropharyngeal Candidiasis (Thrush)
Whitish pseudomembranous plaques on erythematous buccal mucosa, tongue, and palate. Easily scraped off (distinguishes from oral hairy leukoplakia). Erythematous form presents as a shiny, depapillated tongue (median rhomboid glossitis).
Angular cheilitis (perleche): Fissuring and crusting at the oral commissures.
Vulvovaginal / Genital Candidiasis
- Patchy erythema on glans penis and prepuce with balanitis/balanoposthitis (pustules more common here than in vulvitis)
- Pruritus and burning sensation
- In women: thick, white, "cottage cheese" discharge
PART 3: PITYRIASIS (TINEA) VERSICOLOR
Pathogen: Malassezia globosa (also M. restricta, M. furfur) - a lipophilic yeast that is part of normal skin flora but converts to pathogenic mycelial form under favorable conditions (heat, humidity, oily skin, immunosuppression).
Clinical Features:
- Hypopigmented or hyperpigmented coalescing scaly macules on the trunk, upper arms, and upper back
- Pink, atrophic, and trichrome variants exist
- More prominent in summer (heat/humidity); favors oily skin
- Mild pruritus; lesions more visible after sun exposure
- Can involve scalp, pubic area, and rarely face (more common in infants/immunocompromised)

Figure: Tinea versicolor - multiple round, coalescing hypopigmented scaly macules scattered across the trunk. - Andrews' Diseases of the Skin
Mechanism of hypopigmentation: The organism produces dicarboxylic acids (azelaic acid) that inhibit melanocyte tyrosinase, producing abnormally small, poorly melanized melanosomes. Hypopigmentation may persist for weeks to months after cure.
Diagnosis:
- KOH prep shows short thick hyphae + large clusters of round spores = "spaghetti and meatballs" appearance
- Wood's lamp: yellow-green fluorescence
- Biopsy: thick basket-weave stratum corneum with hyphae and spores
Treatment: Topical selenium sulfide shampoo, ketoconazole shampoo, or topical azoles for limited disease. Oral fluconazole or itraconazole for extensive/recurrent disease. UV exposure speeds repigmentation after cure.
Antifungal Treatment Summary
| Drug Class | Examples | Mechanism | Use |
|---|---|---|---|
| Allylamines | Terbinafine, naftifine | Inhibit squalene epoxidase → ergosterol synthesis blocked | Dermatophytes (first-line) |
| Azoles (topical) | Clotrimazole, miconazole, ketoconazole, econazole | Inhibit 14α-demethylase → ergosterol depletion | Broad spectrum: tinea, candida, Malassezia |
| Azoles (oral) | Fluconazole, itraconazole, ketoconazole | Same mechanism | Systemic/extensive infections |
| Polyenes | Nystatin, amphotericin B | Bind ergosterol → membrane disruption | Candida (nystatin topical); systemic (amphotericin) |
| Ciclopirox | Ciclopirox olamine | Chelates metal ions; disrupts membrane | Broad spectrum topical |
| Griseofulvin | Griseofulvin | Disrupts microtubules → inhibits mitosis | Tinea capitis/barbae (oral) |
Key clinical notes:
- Most topical antifungals are applied twice daily for 2-4 weeks (terbinafine can be 1 week)
- Avoid combination corticosteroid-antifungal products: they suppress inflammation, masking signs of spread ("tinea incognita")
- Recurrence is common without correction of predisposing conditions (moisture, diabetes, footwear)
Sources: Fitzpatrick's Dermatology, Vols 1 & 2; Andrews' Diseases of the Skin (Clinical Dermatology); Goodman & Gilman's Pharmacological Basis of Therapeutics; Dermatology 2-Volume Set 5e
This is a shared conversation. Sign in to Orris to start your own chat.