Compliance of lungs and thorax together
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have everything needed for a thorough answer. Here it is:
Compliance of Lungs and Thorax Together
Definition of Compliance
Compliance is the change in volume produced per unit change in pressure (C = ΔV / ΔP), expressed in mL/cm H₂O. It reflects how easily the respiratory system can be distended.
Individual Compliances
| Structure | Normal Compliance |
|---|---|
| Lungs alone | ~200 mL/cm H₂O |
| Chest wall (thorax) alone | ~200 mL/cm H₂O |
| Lungs + thorax together | ~110 mL/cm H₂O |
Why the Combined Compliance Is Lower - The "Springs in Series" Concept
The lungs and thorax are mechanically coupled and act like two springs in series (not in parallel). For springs in series, the total compliance follows:
1/C(total) = 1/C(lungs) + 1/C(thorax)
Substituting:
1/C(total) = 1/200 + 1/200 = 2/200 → C(total) = 100 mL/cm H₂O
Experimentally, this works out to approximately 110 mL/cm H₂O - essentially half the compliance of the lungs alone. To inflate the total pulmonary system, almost twice as much pressure is needed compared to expanding the lungs alone (after removal from the chest cage).
- Guyton and Hall Textbook of Medical Physiology, p. 531
Measurement
Combined lung-thorax compliance is measured by forcing air into the lungs of a totally relaxed or paralyzed subject in small increments and recording pressure and volume at each step. The paralysis eliminates any active muscle contribution, ensuring you are measuring purely passive elastic properties.
The Coupling Mechanism: Pleural Pressure
The key to understanding why the two structures are mechanically coupled is the pleural space:
- The inward recoil of the lungs and the outward recoil of the chest wall act in opposite directions.
- At FRC (functional residual capacity), these two recoil forces are balanced, and pleural pressure is negative (approximately -3 to -4 cm H₂O).
- Any change in volume during breathing requires overcoming the elastic recoil of both structures simultaneously.
Campbell Diagram (Graphical Integration)
The diagram below (from Murray & Nadel's Textbook of Respiratory Medicine) illustrates how lung and chest wall mechanics integrate:
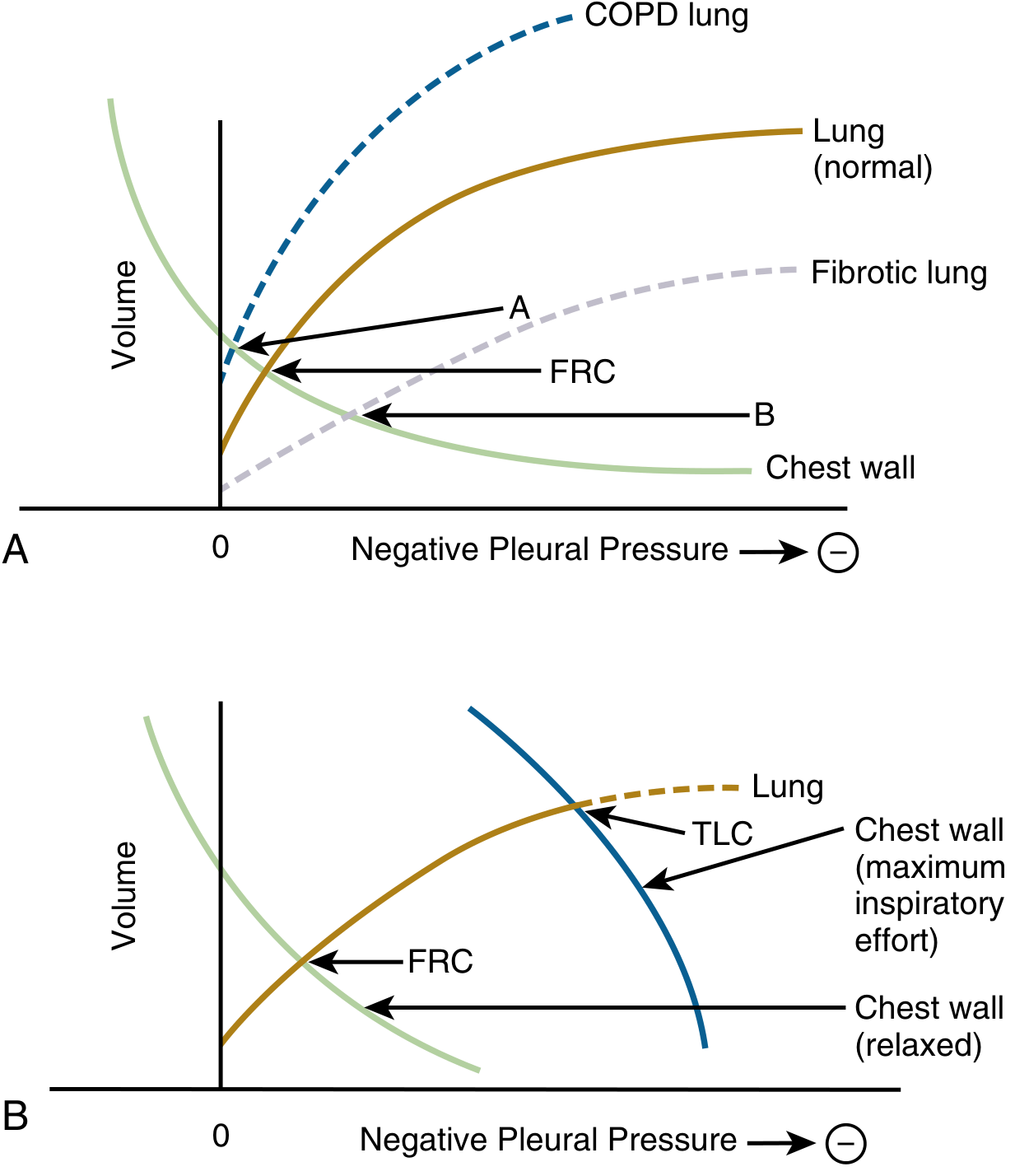
Panel A - The point where the lung recoil curve and the relaxed chest wall curve intersect is FRC. In COPD (increased lung compliance), FRC shifts upward (A). In fibrosis (reduced lung compliance), FRC shifts downward (B).
Panel B - During maximum inspiratory effort, the chest wall curve shifts rightward, increasing volume above FRC toward TLC. TLC is reached where the lung's elastic recoil is maximal and no further inspiratory muscle effort can overcome it.
- Murray & Nadel's Textbook of Respiratory Medicine, p. 256
Compliance at Extremes of Lung Volume
At normal tidal volumes, combined compliance (~110 mL/cm H₂O) applies. However:
- At high lung volumes (near TLC): the chest wall recoils strongly inward, and lung tissues reach their elastic limit. Combined compliance can fall to less than 20% of the lungs-alone value.
- At low lung volumes (near RV): the chest wall becomes very stiff as it tries to recoil outward below its resting volume.
This is why breathing at extremes of the volume range requires disproportionately more muscular effort.
Clinical Significance
| Condition | Effect on Compliance | Mechanism |
|---|---|---|
| Pulmonary fibrosis | Reduced lung compliance | Stiff parenchyma; FRC decreases |
| Emphysema / COPD | Increased lung compliance | Tissue destruction; FRC increases |
| Severe kyphoscoliosis | Reduced chest wall compliance | Deformed thoracic cage |
| Obesity | Reduced chest wall compliance | Excess fat on thorax/abdomen |
| Burns (skin eschar) | Reduced chest wall compliance | Inelastic chest wall |
| Paralysis/anesthesia | FRC decreases ~20% | Loss of inspiratory muscle tone reduces resting chest wall outward recoil |
| ARDS | Severely reduced lung compliance | Alveolar flooding, surfactant dysfunction |
- Murray & Nadel's Textbook of Respiratory Medicine, p. 257; Barash Clinical Anesthesia, 9e
Work of Breathing and Compliance
Reduced combined compliance means the respiratory muscles must generate more pressure per unit volume - this increases the elastic (compliance) work of breathing. In extreme low-compliance states (e.g., severe ARDS or fibrosis), the increased work leads to:
- Progressive respiratory muscle fatigue
- Hypoventilation
- Respiratory acidosis
During normal quiet breathing, only 3-5% of total body energy expenditure goes to breathing; this can increase up to 50-fold in diseases with severely reduced compliance.
- Guyton and Hall Textbook of Medical Physiology, p. 531
Now say it in Bengali without changing the medical terms
Lungs এবং Thorax একসাথে Compliance
Compliance এর সংজ্ঞা
Compliance হলো প্রতি একক pressure পরিবর্তনে যে volume পরিবর্তন হয় তার পরিমাপ (C = ΔV / ΔP), যা mL/cm H₂O তে প্রকাশ করা হয়। এটি respiratory system কে কতটা সহজে প্রসারিত করা যায় তা বোঝায়।
আলাদা আলাদা Compliance
| Structure | স্বাভাবিক Compliance |
|---|---|
| শুধু Lungs | ~200 mL/cm H₂O |
| শুধু Chest wall (Thorax) | ~200 mL/cm H₂O |
| Lungs + Thorax একসাথে | ~110 mL/cm H₂O |
Combined Compliance কেন কম হয় - "Springs in Series" ধারণা
Lungs এবং Thorax যান্ত্রিকভাবে যুক্ত এবং এরা দুটি springs in series এর মতো কাজ করে (parallel এ নয়)। Springs in series এর ক্ষেত্রে মোট compliance এইভাবে হিসাব করা হয়:
1/C(total) = 1/C(lungs) + 1/C(thorax)
মান বসালে:
1/C(total) = 1/200 + 1/200 = 2/200 → C(total) = 100 mL/cm H₂O
পরীক্ষামূলকভাবে এটি প্রায় 110 mL/cm H₂O হয় - অর্থাৎ শুধু lungs এর compliance এর প্রায় অর্ধেক। পুরো pulmonary system কে inflate করতে শুধু lungs কে (chest cage থেকে বের করে) প্রসারিত করার চেয়ে প্রায় দ্বিগুণ pressure লাগে।
পরিমাপ পদ্ধতি
Combined lung-thorax compliance পরিমাপ করা হয় একজন সম্পূর্ণ relaxed বা paralyzed subject এর lungs এ অল্প অল্প করে বায়ু ঢুকিয়ে প্রতিটি ধাপে pressure ও volume রেকর্ড করে। Paralysis করার কারণ হলো যেকোনো active muscle এর অবদান বাদ দেওয়া, যাতে শুধু passive elastic properties পরিমাপ হয়।
সংযোগের মূল প্রক্রিয়া: Pleural Pressure
দুটি structure কেন যান্ত্রিকভাবে যুক্ত তা বোঝার চাবিকাঠি হলো pleural space:
- Lungs এর inward recoil এবং chest wall এর outward recoil বিপরীত দিকে কাজ করে।
- FRC (Functional Residual Capacity) তে এই দুটি recoil force সাম্যাবস্থায় থাকে এবং pleural pressure ঋণাত্মক থাকে (প্রায় -3 থেকে -4 cm H₂O)।
- শ্বাস-প্রশ্বাসের সময় যেকোনো volume পরিবর্তনে উভয় structure এর elastic recoil কে একসাথে অতিক্রম করতে হয়।
Campbell Diagram (চিত্রে একত্রীকরণ)
নিচের diagram টি দেখায় কীভাবে lung ও chest wall এর mechanics একসাথে কাজ করে:
Panel A - যেখানে lung recoil curve এবং relaxed chest wall curve মিলিত হয় সেটি হলো FRC। COPD তে (lung compliance বৃদ্ধি পেলে) FRC উপরে উঠে যায় (A)। Fibrosis এ (lung compliance কমে গেলে) FRC নিচে নামে (B)।
Panel B - Maximum inspiratory effort এর সময় chest wall curve ডানদিকে সরে যায়, FRC থেকে TLC এর দিকে volume বাড়ে। TLC পৌঁছায় যেখানে lung এর elastic recoil সর্বোচ্চ এবং আর কোনো inspiratory muscle effort তা অতিক্রম করতে পারে না।
Lung Volume এর চরম সীমায় Compliance
স্বাভাবিক tidal volume এ combined compliance (~110 mL/cm H₂O) প্রযোজ্য। কিন্তু:
- বেশি lung volume এ (TLC এর কাছাকাছি): chest wall জোরালোভাবে ভেতরে recoil করে এবং lung tissue তাদের elastic limit এ পৌঁছায়। Combined compliance শুধু lungs এর মানের 20% এরও কম হয়ে যেতে পারে।
- কম lung volume এ (RV এর কাছাকাছি): chest wall অত্যন্ত stiff হয়ে যায় কারণ এটি তার resting volume এর নিচে বাইরের দিকে recoil করার চেষ্টা করে।
এই কারণেই volume range এর চরম সীমায় শ্বাস নিতে অনেক বেশি muscular effort লাগে।
Clinical গুরুত্ব
| অবস্থা | Compliance এর উপর প্রভাব | প্রক্রিয়া |
|---|---|---|
| Pulmonary fibrosis | Lung compliance কমে | Stiff parenchyma; FRC কমে |
| Emphysema / COPD | Lung compliance বাড়ে | Tissue ধ্বংস; FRC বাড়ে |
| Severe kyphoscoliosis | Chest wall compliance কমে | Thoracic cage বিকৃত হয় |
| Obesity | Chest wall compliance কমে | Thorax ও abdomen এ অতিরিক্ত চর্বি |
| Burns (skin eschar) | Chest wall compliance কমে | Inelastic chest wall |
| Paralysis / Anesthesia | FRC প্রায় ২০% কমে | Inspiratory muscle tone হারিয়ে chest wall এর outward recoil কমে |
| ARDS | Lung compliance মারাত্মকভাবে কমে | Alveolar flooding, surfactant dysfunction |
Work of Breathing এবং Compliance
Combined compliance কমে গেলে respiratory muscles কে প্রতি একক volume এর জন্য বেশি pressure তৈরি করতে হয় - এতে elastic (compliance) work of breathing বেড়ে যায়। চরম low compliance অবস্থায় (যেমন severe ARDS বা fibrosis) এই বাড়তি কাজের ফলে হয়:
- Progressive respiratory muscle fatigue
- Hypoventilation
- Respiratory acidosis
স্বাভাবিক শান্ত শ্বাস-প্রশ্বাসে মোট শরীরের energy expenditure এর মাত্র ৩-৫% শ্বাসক্রিয়ায় যায়; compliance মারাত্মকভাবে কমে গেলে এটি ৫০ গুণ পর্যন্ত বাড়তে পারে।
This is a shared conversation. Sign in to Orris to start your own chat.