Jerky septal motion in echocardiography in setting of concentric LVH what is the significance?
"septal motion" echocardiography "concentric hypertrophy"
jerky septal motion echocardiography concentric LVH significance LBBB RV pacing
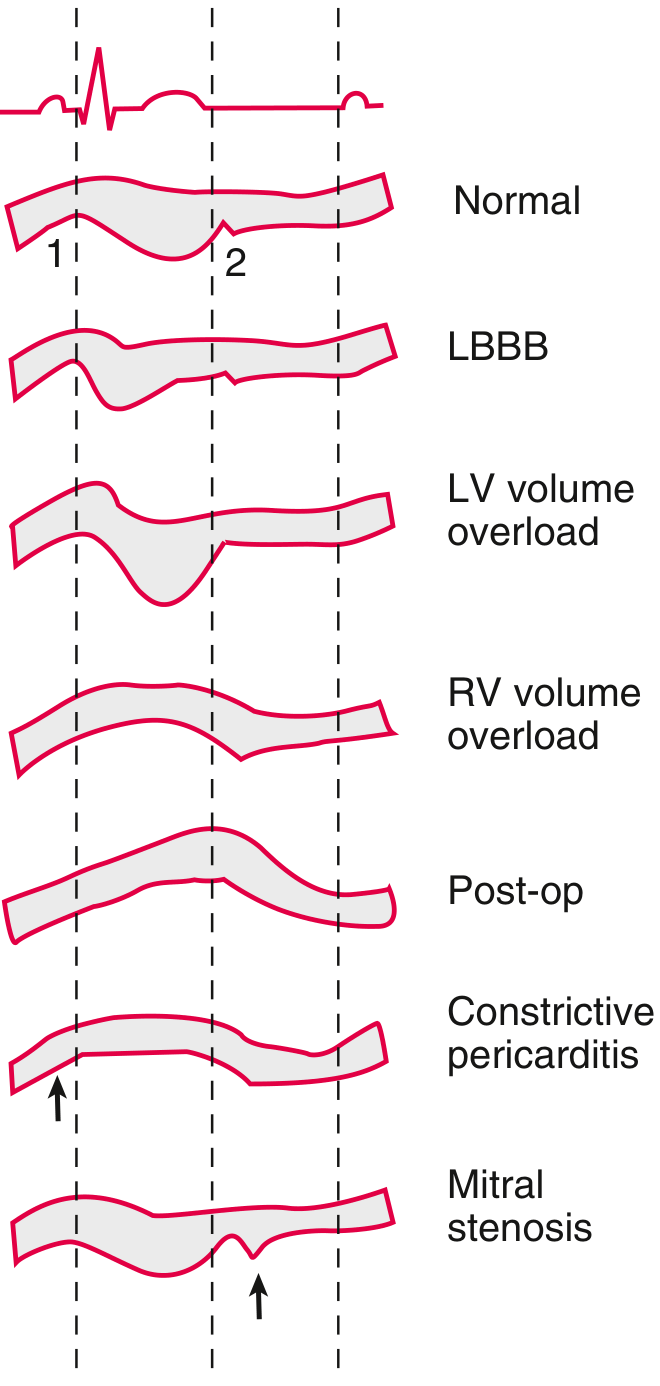
Jerky Septal Motion on Echocardiography in the Setting of Concentric LVH
What "Jerky" Septal Motion Means
Key Causes of Jerky/Abnormal Septal Motion
Significance in the Setting of Concentric LVH
1. Left Bundle Branch Block (LBBB) — Most Important Interpretation
- The RV contracts before the LV — the septum shoots posteriorly (or anteriorly on M-mode depending on convention) in early systole, then snaps back — creating the characteristic "jerky" or "paradoxical" septal motion
- In a patient with concentric LVH (e.g., from hypertension, aortic stenosis, hypertrophic cardiomyopathy), the hypertrophied septum amplifies this motion, making it even more visually striking
- LBBB is common in patients with pressure-overload LVH (hypertensive heart disease, aortic stenosis, dilated cardiomyopathy)
"Left bundle branch block (LBBB) is characterized by systolic rapid downward septal motion" — Textbook of Clinical Echocardiography, p. 196
"Dobutamine stress echocardiography may not be reliable in patients with left bundle-branch block because septal motion may be abnormal, even in the absence of left anterior descending CAD in some patients." — Morgan & Mikhail's Clinical Anesthesiology, 7e
2. RV Pacing
3. Post-Cardiac Surgery
"Left bundle branch block, right ventricular pacing, and previous open heart surgery can lead to decreased septal wall motion (abnormal septal motion usually present at rest)" — Pfenninger and Fowler's Procedures for Primary Care
4. RV Pressure Overload / Pulmonary Hypertension
"Pressure overload of the RV... results in a leftward shift of septal motion throughout the cardiac cycle" — Textbook of Clinical Echocardiography, p. 192
5. Constrictive Pericarditis (Septal Bounce)
Summary Table
| Cause | Timing of Jerk | Associated Findings |
|---|---|---|
| LBBB | Early systole | Wide QRS on ECG, no RV enlargement |
| RV pacing | Early systole | Pacemaker on CXR/ECG |
| Post-cardiac surgery | Systolic, fixed | Surgical history, normal RV |
| RV pressure overload | Throughout systole | RV hypertrophy, TR, elevated RVSP |
| Constrictive pericarditis | Early diastole (bounce) | Pericardial thickening, respiratory variation, septal bounce |
Key Takeaway
Can 6 months infant start curd?
"complementary feeding" infant yogurt dairy
WHO AAP guidelines curd yogurt for 6 month old infant complementary feeding dairy
Can a 6-Month-Old Infant Start Curd (Yogurt)?
What the Guidelines Say
- Complementary foods should begin at 6 months of age alongside continued breastfeeding
- Dairy (including yogurt/curd and cheese) is listed as one of the eight key food groups recommended as part of a diverse complementary diet from 6 months onward
- WHO and UNICEF define minimum dietary diversity as 5 out of 8 groups, with dairy counting as one group
- Yogurt and cheese can be introduced once the baby is 6 months old, as long as they continue to eat iron-rich foods alongside
- Plain, full-fat, pasteurized yogurt is preferred
Why Curd/Yogurt Is Suitable at 6 Months
| Reason | Detail |
|---|---|
| Easier to digest than cow's milk | Fermentation breaks down milk proteins (casein) into smaller peptides — easier on an infant's immature gut |
| Probiotic bacteria | Live cultures (Lactobacillus, Streptococcus thermophilus) support gut microbiome development |
| Nutrient-dense | Rich in protein, calcium, phosphorus, fat-soluble vitamins — important for bone and brain development |
| No iron-displacement risk | Unlike liquid cow's milk as a main drink, yogurt as a complementary food does not displace iron-containing breast milk/formula |
Important Distinction: Curd ≠ Cow's Milk as Main Drink
- ✅ Curd/yogurt as a food from 6 months — safe and recommended
- ❌ Cow's milk as a main drink/feed — not before 12 months
How to Give Curd at 6 Months
- Type: Plain, whole-fat, pasteurized curd (home-made dahi is fine in India if made from pasteurized full-cream milk)
- Quantity: Start with 1–2 teaspoons, gradually increase to 2–3 tablespoons per serving
- Texture: Plain, unsweetened — no added sugar, salt, honey, or flavoring
- Frequency: Once daily initially, watching for any allergy signs
- Temperature: At room temperature or slightly warm — avoid very cold straight from fridge
Watch for Milk Protein Allergy
- Hives, rash, eczema flare
- Vomiting, diarrhea, blood in stool
- Refusal to feed, excessive crying
Summary
Curd is a recommended complementary food from 6 months. It is easier to digest than raw cow's milk, nutritious, and supports gut health. Give small amounts of plain, full-fat, pasteurized curd — not as a milk replacement, but as a food alongside breast milk or formula.
What are 8 food groups
WHO/UNICEF 8 Key Food Groups for Infants & Young Children (6–23 months)
| # | Food Group | Examples |
|---|---|---|
| 1 | Breast milk | Continued breastfeeding |
| 2 | Flesh foods | Meat, fish, poultry, liver, organ meats |
| 3 | Dairy | Milk, yogurt/curd, cheese |
| 4 | Eggs | Hen's egg, duck egg |
| 5 | Legumes and nuts | Lentils (dal), beans, chickpeas, peanut paste |
| 6 | Vitamin A–rich fruits & vegetables | Carrot, pumpkin, mango, papaya, spinach, sweet potato |
| 7 | Other fruits and vegetables | Banana, apple, potato, tomato, cucumber |
| 8 | Grains, roots, and tubers | Rice, wheat (roti/porridge), oats, potato, suji |
Minimum Dietary Diversity (MDD)
Why This Matters at 6 Months
- Breast milk alone is no longer sufficient after 6 months for energy and micronutrients (especially iron and zinc)
- Iron and zinc are primarily found in groups 2 (flesh foods), 4 (eggs), and 5 (legumes) — these are the most critical groups to introduce early
- Group 6 (Vitamin A–rich foods) protects against deficiency, which is common in South Asian infants
- The goal is to gradually expand across all 8 groups by 12 months
How to introduce flesh food at 6 months how to cook and what
how to introduce meat fish to 6 month old infant complementary feeding preparation texture WHO guidelines
Introducing Flesh Foods at 6 Months
Why It's a Priority
Which Flesh Foods to Start With
Best First Choices (easiest to prepare, digest, and accept)
| Food | Why Start Here |
|---|---|
| Fish (rohu, katla, pomfret, salmon) | Soft texture, easy to puree, rich in zinc, iron, omega-3 |
| Chicken (breast or thigh) | Mild flavor, soft when pressure-cooked, high protein |
| Liver (chicken liver) | Exceptionally rich in iron, zinc, B12, Vitamin A — best single food for micronutrient density |
| Egg yolk | Technically flesh-food group — easy to start, iron + choline-rich |
| Mutton/goat (soft pieces) | Good iron source, familiar in Indian households |
Start with fish or chicken liver — both are soft, nutrient-dense, and easy to puree at 6 months.
How to Cook at 6 Months (Step-by-Step)
General Rules
- Cook thoroughly — fully cooked, no pink center
- No salt, sugar, spices, or honey before 12 months
- No whole pieces — must be pureed or mashed smooth at 6 months
- Remove all bones, skin, and fat before blending
- Add a little cooking water or breast milk to get the right puree consistency
🐟 Fish Puree (Best First Flesh Food)
- Take 1–2 tablespoons of boneless fish (rohu, pomfret, or salmon)
- Pressure cook or steam with a little water for 5–7 minutes until very soft
- Remove all bones carefully — run fingers through to check
- Blend/mash with cooking water into a smooth, lump-free paste
- Mix into dal water, rice porridge (khichdi), or give alone
🍗 Chicken Puree
- Take 1 small piece of boneless chicken (breast or thigh)
- Pressure cook with water for 3–4 whistles until very tender
- Shred finely, then blend with cooking stock into a smooth paste
- Mix into rice porridge or vegetable puree
🫀 Chicken Liver Puree (Iron Powerhouse)
- Take 1–2 small chicken livers
- Boil/simmer in water for 10–12 minutes until fully cooked through (no pink)
- Blend smooth with cooking water
- Mix into khichdi or rice porridge — liver has a strong taste, so mixing helps acceptance
🥚 Egg Yolk (Easiest Start)
- Hard boil an egg — cook until yolk is completely firm (not soft/runny)
- Scoop out yolk only (white can be introduced at 6 months too — current evidence supports this)
- Mash yolk with a little breast milk or boiled water to smooth paste
- Serve alone or mixed with porridge
Practical Combination: Iron-Rich Khichdi
Rice + Moong Dal + Chicken/Fish puree + A drop of ghee Pressure cook, blend smooth, add flesh food puree — complete meal with iron, protein, and energy
Introduction Schedule
| Age | Texture | Frequency | Amount per meal |
|---|---|---|---|
| 6–7 months | Smooth puree, lump-free | 2–3 times/day | 2–3 tablespoons |
| 7–8 months | Mashed, soft lumps okay | 3 times/day | 3–4 tablespoons |
| 9–11 months | Minced, soft pieces | 3–4 times/day | 4–5 tablespoons |
| 12 months+ | Family food texture | 3–4 times/day | As appetite allows |
Key Safety Points
- ✅ One new food every 3 days — watch for allergy reactions (rash, vomiting, diarrhea)
- ✅ Always fully cooked — no raw/rare meat or fish for infants
- ✅ No honey before 12 months (botulism risk)
- ✅ No whole fish — even tiny bones are a choking/injury hazard
- ❌ No salt or seasoning — infant kidneys cannot handle sodium
- ❌ Avoid shark, swordfish, king mackerel — high mercury content
If I want my child to be Vegetarian what food group can I give for iron i am ok with egg and milk
vegetarian infant iron sources 6 months complementary feeding non-heme iron absorption vitamin C WHO AAP
Iron for Your Vegetarian Baby (Eggs + Milk Accepted)
First, the Most Important Fact
The NIH recommends vegetarian infants target ~1.8× more iron from food than meat-eating babies, because non-heme iron has lower absorption. This makes food pairing and variety critical.
Your Iron Sources (Ovo-Lacto Vegetarian)
⭐ Tier 1 — Best Iron Sources Available to You
| Food | Iron Content | Notes |
|---|---|---|
| Egg yolk | Good | Hard-boil, mash — introduce from 6 months |
| Moong dal / masoor dal / toor dal | High | Pressure-cook very soft, puree |
| Rajma (kidney beans) | High | Mash well, introduce after 7–8 months |
| Chickpeas (chana) | High | Well-cooked, pureed |
| Iron-fortified infant cereal (ragi, oats) | Very high | Best single plant iron source — easy to add daily |
| Ragi (finger millet) | High | Excellent iron + calcium — ideal for Indian vegetarian babies |
| Tofu | High | Soft, easy to mash — introduce from 6–7 months |
⭐ Tier 2 — Moderate Iron Sources
| Food | Notes |
|---|---|
| Spinach / palak | Good iron, but contains oxalates that reduce absorption — still useful |
| Pumpkin seeds (powdered) | Mix into porridge |
| Sesame seeds (til) | Mix as paste into khichdi |
| Beetroot | Moderate iron, sweet taste — good puree |
| Sweet potato + peas | Add to khichdi |
| Fortified roti flour | If using commercially fortified atta |
The Most Important Rule: Always Pair Iron with Vitamin C
| Iron Food | Pair With (Vitamin C) |
|---|---|
| Dal khichdi | Squeeze of tomato puree in the khichdi |
| Ragi porridge | Mashed strawberry / kiwi / orange juice (a few drops) |
| Spinach puree | Tomato puree mixed in |
| Egg yolk | Mashed soft tomato alongside |
| Rajma mash | Amla (gooseberry) puree or capsicum puree |
Amla (Indian gooseberry) is one of the richest Vitamin C sources — a tiny amount mixed into any iron-rich food significantly boosts absorption. From 7–8 months, a small amount of strained amla juice or puree can be added.
What BLOCKS Iron Absorption — Avoid at the Same Meal
| Avoid pairing with iron foods | Why |
|---|---|
| Cow's milk / curd | Calcium blocks iron absorption |
| Tea / coffee | Tannins — not for infants anyway |
| Spinach + dal together | Oxalates from spinach reduce dal iron — give spinach separately |
Give dairy (curd, milk in food) at a different meal from iron-rich meals. This is key for vegetarian babies.
Daily Iron-Rich Meal Plan (6–8 Months, Vegetarian)
| Meal | Food | Iron Source |
|---|---|---|
| Morning | Ragi porridge + mashed strawberry | Ragi (iron) + Vit C |
| Midday | Moong dal + rice khichdi + tomato puree + ghee | Dal iron + Vit C |
| Evening | Egg yolk mashed with soft tomato | Heme-adjacent + Vit C |
| Breast milk / formula | On demand | (Give separately from iron meals) |
Should You Give an Iron Supplement?
- Exclusively breastfed infants who do not get adequate iron from food — 1 mg/kg/day iron drops until dietary iron is established
- Vegetarian infants are at higher risk and may need supplementation even with a well-planned diet
- Hemoglobin screening at 12 months is standard — do not skip this
Signs of Iron Deficiency to Watch For
- Pale skin (check inner eyelids and nail beds)
- Unusual tiredness, low energy
- Poor appetite
- Irritability
- Delayed milestones (iron is critical for brain development)
Summary
Your best iron strategy: Egg yolk daily + dal at every meal + ragi regularly + always pair with Vitamin C + give dairy at separate meals from iron foods + discuss iron drops with your pediatrician.
Can dates be used to sweeten infant foods ?
dates as sweetener for infant baby food 6 months safety WHO AAP sugar guidelines