Dyspnoea
Reading File
Finding Sources
Searching PubMed
"dyspnea"[MeSH Terms] AND "pathophysiology"
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive content. Let me compile a thorough, well-structured answer on dyspnoea.
Dyspnoea (Dyspnea)
Definition
The American Thoracic Society (ATS) defines dyspnoea as a "subjective experience of breathing discomfort that consists of qualitatively distinct sensations that vary in intensity." The experience arises from interactions among physiological, psychological, social, and environmental factors. Common synonyms include shortness of breath, breathlessness, and "air hunger." It is a symptom - it can only be perceived and self-reported by the patient - not to be confused with signs such as tachypnoea, accessory muscle use, or intercostal recession, which are observable by clinicians.
Patients describe it variably: "tightness," "choking," "unable to take a deep breath," "suffocating," "can't get enough air."
- Harrison's Principles of Internal Medicine, 22E, p. 311
Epidemiology
-
Reported in up to 50% of inpatients and 25% of ambulatory patients
-
Community prevalence: 9-13%, rising to ~37% in adults ≥70 years
-
Accounts for 3-4 million emergency room visits per year
-
The degree of dyspnoea may predict outcomes in COPD better than FEV1, and it is formally incorporated into the GOLD COPD severity guidelines
-
Post-COVID-19 syndrome has further increased its incidence
-
Harrison's Principles of Internal Medicine, 22E, p. 311
Mechanisms
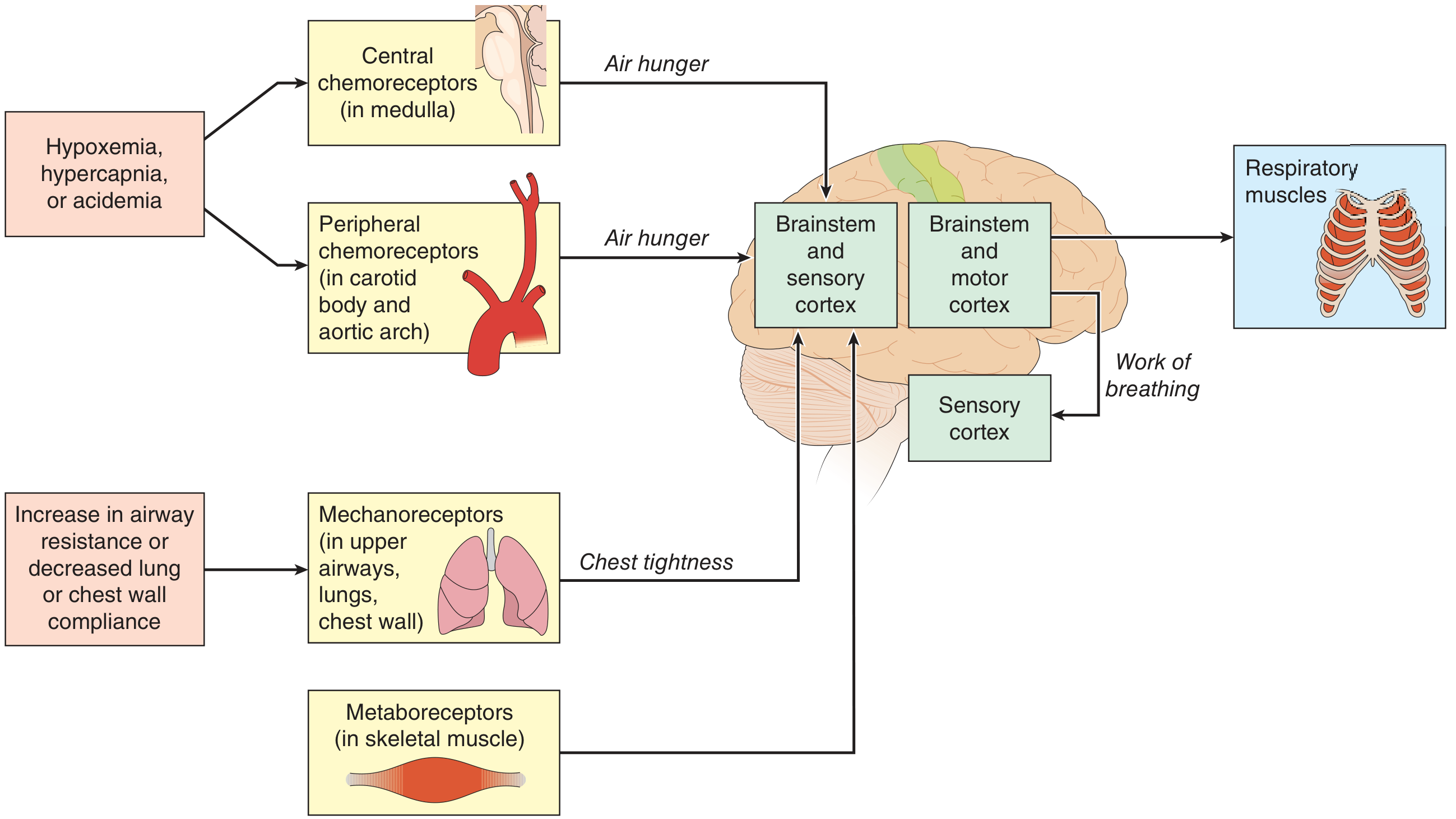
Figure: Neural pathways underlying dyspnoea (Harrison's, 22E)
Three broad factors contribute to dyspnoea (Guyton & Hall):
- Abnormal blood gases - especially hypercapnia (CO2 excess), and to a lesser degree hypoxaemia
- Increased work of breathing - excessive effort by respiratory muscles even when blood gases are normal
- State of mind / psychological factors - neurogenic or emotional dyspnoea
Neural Pathways (Harrison's 22E)
Dyspnoea arises from a complex interplay of:
| Pathway | Trigger | Sensation |
|---|---|---|
| Central chemoreceptors (medulla) | Hypercapnia, acidaemia | Air hunger |
| Peripheral chemoreceptors (carotid body, aortic arch) | Hypoxaemia, hypercapnia | Air hunger |
| Mechanoreceptors (upper airways, lungs, chest wall) | Increased airway resistance, decreased compliance | Chest tightness |
| Metaboreceptors (skeletal muscle) | Reduced cardiac output/lactic acidosis | Work of breathing sensation |
A key concept is efferent-reafferent mismatch: when the motor command from the brainstem/cortex to the respiratory muscles does not match the afferent feedback received - the brain perceives a mismatch between the drive to breathe and the mechanical response - producing the uncomfortable sensation of dyspnoea.
Special Descriptors / Clinical Patterns
| Term | Description | Implication |
|---|---|---|
| Orthopnoea | Dyspnoea worsening when supine | Left ventricular failure, chronic lung disease |
| Paroxysmal nocturnal dyspnoea (PND) | Episodes waking patient from sleep | Left ventricular failure (also COPD with secretion pooling) |
| Platypnea | Dyspnoea in the upright position | Pulmonary vascular shunting |
| Trepopnea | Dyspnoea in one lateral decubitus position | Pulmonary vascular shunting |
| Instant orthopnoea | Inability to lie flat at all | Bilateral diaphragm paralysis |
| Hyperpnea | Increased minute ventilation | No implication about dyspnoea per se |
| Hyperventilation | Increased alveolar ventilation beyond CO2 production | Can be psychogenic |
- Murray & Nadel's Textbook of Respiratory Medicine, p. (block 4)
Differential Diagnosis
Pulmonary and cardiac causes account for ~85% of all dyspnoea. Up to one-third of patients have multifactorial aetiology.
Pulmonary Causes
- Airways disease: Asthma, COPD, upper airway obstruction
- Presents with: chest tightness, wheezing, accessory muscle use
- Parenchymal disease: Interstitial lung disease (IPF, collagen vascular disease, drug/occupational pneumonitis), hypersensitivity pneumonitis, BOOP
- Presents with: progressive exertional dyspnoea, fine crackles
- Chest wall / neuromuscular: Kyphoscoliosis, amyotrophic lateral sclerosis, myasthenia gravis, diaphragm paralysis
- Pulmonary vascular: Pulmonary hypertension, chronic thromboembolic disease (CTEPH), pulmonary embolism
Cardiac Causes
- Left heart failure (CAD, cardiomyopathy, diastolic dysfunction) - most common cardiac cause; produces raised pulmonary venous pressure
- Valvular heart disease
- Pericardial disease - constrictive pericarditis, cardiac tamponade
- Myocardial ischaemia (acute)
Other Causes
- Anaemia - reduces oxygen-carrying capacity; can cause dyspnoea at rest in severe cases
- Deconditioning - presents as "heavy breathing" or "rapid breathing" with minimal exertion
- Metabolic acidosis (e.g., DKA) - compensatory Kussmaul breathing
- Anxiety / panic disorder - psychogenic dyspnoea; may produce hyperventilation syndrome with lightheadedness, perioral tingling
- Post-COVID syndrome
- Drug overdoses (e.g., salicylates)
- Severe sepsis / systemic disease
Acute vs. Chronic
-
Acute: MI, acute heart failure, severe hypertension, pulmonary embolism, pneumothorax, upper airway obstruction, anaphylaxis, acute asthma
-
Subacute/Chronic (>1 month): COPD, ILD, heart failure, pulmonary hypertension, deconditioning, neuromuscular disease
-
Goldman-Cecil Medicine, p. 388; Harrison's 22E, p. 312
Assessment
History
- Character of sensation: Air hunger (heart failure), chest tightness (bronchoconstriction), increased work/effort (airway obstruction, neuromuscular disease), rapid/heavy breathing (deconditioning)
- Onset and course: Acute vs. subacute vs. chronic; episodic vs. continuous
- Precipitants: Exertion, posture, cold air, allergens, cigarette smoke, perfumes, moulds
- Relieving factors: Rest, leaning forward, inhaled bronchodilator, oxygen, diuresis
- Associated symptoms: Wheeze, productive cough, fever, ankle oedema, chest pain, haemoptysis, orthopnoea, PND
Grading: Modified MRC Dyspnoea Scale (mMRC)
| Grade | Description |
|---|---|
| 0 | Not troubled except with strenuous exercise |
| 1 | Breathless walking uphill or hurrying on level ground |
| 2 | Walks slower than peers on level ground due to breathlessness, or must stop to rest at own pace |
| 3 | Stops after ~100m or after a few minutes on level ground |
| 4 | Too breathless to leave the house; breathless dressing/undressing |
Integrated into GOLD COPD classification guidelines.
Other validated scales: Borg Scale (exercise intensity rating), British MRC Questionnaire, Pulmonary Functional Status and Dyspnoea Questionnaire (PFSDQ).
Physical Examination
Look for:
- Tachypnoea, use of accessory muscles, intercostal retractions
- Cyanosis, clubbing, wheeze, crackles, reduced breath sounds
- Signs of heart failure: raised JVP, S3 gallop, peripheral oedema, displaced apex
- Signs of anaemia, thyrotoxicosis
Investigations (Stepwise)
| Step | Tests |
|---|---|
| First line | Chest X-ray, ECG, spirometry, FBC, pulse oximetry, BNP/NT-proBNP |
| Second line | Echocardiogram, HRCT chest, DLCO, ABG, exercise oximetry |
| Further | CT pulmonary angiography (PE/CTEPH), V/Q scan, right/left heart catheterisation, cardiopulmonary exercise testing (CPET) |
Management
General Principles
- Treat the underlying cause - this is the cornerstone
- In many chronic conditions, dyspnoea persists despite optimal treatment of the underlying disease
Disease-Specific
| Condition | Treatment |
|---|---|
| Asthma/COPD | Bronchodilators, inhaled corticosteroids, pulmonary rehabilitation |
| Heart failure | Diuretics (often dramatically relieve dyspnoea; though relief is not always proportional to diuresis), ACE inhibitors, beta-blockers, device therapy |
| Pulmonary embolism | Anticoagulation, thrombolysis in massive PE |
| ILD | Antifibrotics (pirfenidone, nintedanib for IPF), immunosuppression for others |
| Pulmonary hypertension | Pulmonary vasodilators, diuretics |
| Anaemia | Treat underlying cause; transfusion if severe |
Symptomatic Relief
- Opioids (low-dose oral morphine) - reduce the sensation of dyspnoea in palliative and severe chronic settings
- Oxygen - beneficial when hypoxaemia is present; evidence for benefit in normoxaemic patients is limited
- Fan to the face - stimulates facial mechanoreceptors (V2 branch of trigeminal nerve), can reduce the perception of dyspnoea
- Pulmonary rehabilitation - improves exercise tolerance and reduces dyspnoea in COPD and ILD
- Anxiolytics/antidepressants - when anxiety is a significant contributor
- Positioning - sitting upright or leaning forward reduces work of breathing
Key Points Summary
- Dyspnoea is purely subjective - always self-reported; tachypnoea and accessory muscle use are the observable correlates
- Underlying mechanism involves chemoreceptor activation (air hunger), mechanoreceptor activation (chest tightness), and efferent-reafferent mismatch
- Pulmonary + cardiac diseases account for 85% of cases
- Character of sensation helps narrow the diagnosis
- Orthopnoea/PND strongly suggest left heart failure but also occur in COPD
- mMRC scale grades functional severity and feeds into GOLD COPD staging
- A stepwise diagnostic approach (history → CXR/ECG/spirometry → advanced imaging) nearly always identifies the cause
Sources: Harrison's Principles of Internal Medicine 22E | Murray & Nadel's Textbook of Respiratory Medicine | Goldman-Cecil Medicine | Guyton & Hall Medical Physiology | Fishman's Pulmonary Diseases and Disorders
Find recent clinical guidelines on dyspnoea management
Reading File
Searching PubMed
"dyspnea"[MeSH Terms] AND "guideline"[pt]
Searching PubMed
"dyspnea"[MeSH Terms] AND management
Searching the Web
clinical guidelines dyspnoea management 2024 2025 ATS ERS
Reading Article
PMID: 39052451
Reading Article
PMID: 40409875
Reading Article
PMID: 39384304
Reading Article
PMID: 39477355
Searching the Web
ATS ERS dyspnea breathlessness guidelines statement 2023 2024 2025
Reading Article
PMID: 35118499
Reading Article
PMID: 35550804
Searching PubMed
"pulmonary rehabilitation"[MeSH Terms] AND dyspnea
Searching the Web
GOLD COPD 2025 guidelines dyspnoea management recommendations
I now have comprehensive material. Let me compile the full response.
Recent Clinical Guidelines on Dyspnoea Management
Here is a structured synthesis of the most current (2022-2025) evidence-based guidelines and systematic reviews across the major clinical contexts in which dyspnoea arises.
1. GOLD 2025 Report - COPD (the most common cause of chronic dyspnoea)
Global Initiative for Chronic Obstructive Lung Disease (GOLD), November 2024
2025 GOLD Report
Dyspnoea management in COPD remains the primary treatment target in the GOLD 2025 update. Key recommendations:
Assessment:
- Use the mMRC Dyspnoea Scale or CAT score to grade symptoms and assign GOLD groups A/B/E
- Follow-up pharmacological management is driven by two "treatable traits": persistence of dyspnoea AND exacerbation frequency
Pharmacological treatment (follow-up):
- Persistent dyspnoea on a single LABA or LAMA: escalate to LABA + LAMA combination
- If dyspnoea persists on LABA+LAMA: consider adding ICS if eosinophil count >300/μL
- New 2025 additions: Ensifentrine (a dual PDE3/PDE4 inhibitor) added as a bronchodilator option; dupilumab added for patients with type 2 inflammation
Non-pharmacological:
- Patients should receive self-management guidance for breathlessness, stress management, and a written action plan
- Pulmonary rehabilitation recommended for all symptomatic patients
2. ACR Appropriateness Criteria: Chronic Dyspnoea - Noncardiovascular Origin (2024 Update)
American College of Radiology Expert Panel, published 2025
PMID: 40409875 - Practice Guideline
Key imaging recommendations for chronic dyspnoea of non-cardiac aetiology:
| Clinical Scenario | Recommended Imaging |
|---|---|
| Initial evaluation (all patients) | Chest X-ray - first line (usually appropriate) |
| Unclear aetiology / suspected COPD / small airways disease | Chest CT without contrast - second line |
| Post-COVID-19 complications | Chest CT without contrast |
| Pleural/chest wall disease or diaphragm dysfunction | Chest CT with contrast |
| Specific functional assessment | Inspiratory/expiratory CT; hyperpolarized xenon gas MRI (specialist settings) |
| Limited roles | MRI, fluoroscopy, FDG-PET/CT |
3. ACR Appropriateness Criteria: Dyspnoea - Suspected Cardiac Origin (2021 Update, published 2022)
American College of Radiology Expert Panel | PMID: 35550804 - Practice Guideline
For suspected cardiac dyspnoea (ischaemia excluded), based on suspected aetiology:
| Suspected Condition | Usually Appropriate Imaging |
|---|---|
| Valvular heart disease | Resting transthoracic echocardiogram (TTE) + chest radiograph |
| Arrhythmia | TTE + MRI heart (function and morphology) |
| Pericardial disease | TTE + chest radiograph + MRI heart + CT heart with IV contrast |
4. 2023 Canadian Thoracic Society (CTS) Guideline on Pharmacotherapy in Stable COPD
Bourbeau J et al., Chest, Nov 2023 | PMID: 37690008
Systematic Review + Meta-Analysis + Practice Guideline
Evidence-based pharmacotherapy recommendations with focus on reducing dyspnoea and exacerbation rate in stable COPD. Strongly supports LAMA monotherapy or LABA+LAMA for symptomatic patients as the backbone of dyspnoea management.
5. Japanese Society for Palliative Medicine - Dyspnoea in Advanced Disease (2024)
Yamaguchi T et al., J Palliat Med, Oct 2024 | PMID: 39052451 - Practice Guideline
Revised clinical guidelines for managing dyspnoea in patients with advanced cancer and non-cancer diseases (e.g., COPD, heart failure, ILD). Key points:
- Guideline recommendations based on systematic reviews for each clinical question plus expert consensus
- Acknowledges a paucity of evidence for many interventions - calls for more real-world observational studies alongside RCTs
- Supports pharmacological (opioids) and non-pharmacological approaches in palliative context
6. ASCO Guideline: Management of Dyspnoea in Advanced Cancer (2022)
Jackson CD et al., South Med J, 2022 | PMID: 35118499 - Practice Guideline
A review of the American Society of Clinical Oncology (ASCO) guideline on dyspnoea in advanced cancer, covering:
- Screening and regular formal assessment
- Opioids as the primary pharmacological option
- Oxygen therapy (only beneficial if hypoxaemic)
- Non-pharmacological: fan therapy, breathing techniques, psychosocial support
7. ERS Systematic Review: Opioids for Breathlessness in Serious Respiratory Illness (2024)
Smallwood NE et al., Eur Respir Rev, Oct 2024 | PMID: 39384304
Systematic Review + Meta-Analysis - Tier 1 Evidence
This is the most important recent evidence update on opioid use for dyspnoea:
| Outcome | Finding |
|---|---|
| Exertional breathlessness (lab testing) | Opioids significantly reduced breathlessness (SMD -0.37) |
| Breathlessness in daily life at home | No significant benefit (SMD -0.10) |
| Health-related quality of life | No significant effect detected |
| Adverse events | Significantly increased nausea/vomiting (OR 3.32), constipation (OR 3.08), drowsiness (OR 1.37); serious events including hospitalisation and death noted |
Clinical implication: The evidence for routine opioid use for chronic breathlessness at home is weaker than previously assumed, and risks may outweigh benefits outside of the palliative/end-of-life setting. Overall certainty of evidence was "very low" to "low".
8. ERS Systematic Review: Breathing Techniques for Serious Respiratory Illness (2024)
Burge AT et al., Eur Respir Rev, Oct 2024 | PMID: 39477355
Systematic Review - Tier 1 Evidence, 73 RCTs, n=5479
| Technique | Effect on Breathlessness (mMRC) | Effect on HRQoL |
|---|---|---|
| Pursed lip / diaphragmatic breathing | MD -0.40 (statistically significant, but below MID) | Consistently improved (exceeded MID) |
| Yoga breathing | MD -1.05 (direction of benefit) | Improved |
| All techniques combined | Modest breathlessness benefit | Consistently improved in COPD and asthma |
| Adverse events | None reported | - |
Clinical implication: Breathing exercises are safe and consistently improve quality of life. Recommended for inclusion in the care of people with serious respiratory illness, despite modest direct effects on breathlessness scores.
9. ATS 2023 Pulmonary Rehabilitation Guidelines
Published in 2023, the American Thoracic Society updated its clinical practice guidelines for pulmonary rehabilitation, developed using GRADE methodology with multidisciplinary input (including a patient with COPD). Key positions:
- Pulmonary rehabilitation is safe and effective for reducing dyspnoea across multiple lung diseases
- Formal evidence base provided to support policy changes improving access
- Dyspnoea, health status, and exercise capacity should all be formally measured as outcomes
10. ERS Guideline on Bronchiectasis (2025)
ERS Executive Committee, September 2025
Incorporates dyspnoea assessment (using MRC breathlessness score, with grade 4-5 reflecting severe functional impairment) as part of the Bronchiectasis Severity Index and mandates formal dyspnoea measurement as part of rehabilitation monitoring.
Summary Table: Guidelines at a Glance
| Guideline | Year | Body | Focus |
|---|---|---|---|
| GOLD 2025 Report | 2025 | GOLD | COPD - dyspnoea as primary treatable trait |
| ACR Appropriateness Criteria (Non-CV) | 2024/25 | ACR | Imaging for non-cardiac chronic dyspnoea |
| ACR Appropriateness Criteria (Cardiac) | 2021/22 | ACR | Imaging for cardiac dyspnoea |
| CTS Pharmacotherapy Guideline | 2023 | CTS | COPD pharmacotherapy |
| JSPM Dyspnoea in Advanced Disease | 2024 | JSPM | Palliative dyspnoea (cancer + non-cancer) |
| ASCO Advanced Cancer Dyspnoea | 2022 | ASCO | Palliative dyspnoea in cancer |
| ATS Pulmonary Rehabilitation | 2023 | ATS | Rehab - reduces dyspnoea, improves QoL |
| ERS Opioids Meta-analysis | 2024 | ERS | Opioids - weaker evidence than assumed |
| ERS Breathing Techniques SR | 2024 | ERS | Breathing exercises - safe, improve QoL |
| ERS Bronchiectasis Guideline | 2025 | ERS | Dyspnoea grading, rehabilitation outcomes |
Bottom line from 2024-2025 evidence:
- The strongest evidence for chronic dyspnoea management remains treating the underlying disease (LABA/LAMA for COPD, diuretics for heart failure, antifibrotics for IPF)
- Pulmonary rehabilitation and breathing exercises have good evidence for symptom reduction and quality of life, with no adverse effects
- Opioids for chronic at-home breathlessness are now under greater scrutiny - benefit in daily life is not well established and adverse events are significant; use should be carefully weighed, particularly outside end-of-life care
- Fan therapy (facial airflow) is a simple, safe non-pharmacological adjunct
- Imaging guidance (ACR 2024): start with chest X-ray, use non-contrast CT as second line for most non-cardiac causes
Puerperium
Reading File
Finding Sources
Searching PubMed
"puerperium"[MeSH Terms] AND complications
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Searching PubMed
"postpartum"[MeSH Terms] AND "hemorrhage OR depression OR thromboembolism"
I now have comprehensive material from multiple authoritative textbooks. Let me compose the full, structured answer.
The Puerperium
Definition and Duration
The puerperium (from Latin puer = child + parere = to bring forth) is the 6-week period beginning immediately after delivery of the placenta (end of the third stage of labour) during which the mother's anatomy, physiology, and biochemistry return to the non-pregnant state. It is sometimes called the postpartum period.
- Gray's Anatomy for Students defines it as: "a 6-week period that begins after the delivery of the placenta, during which the body undergoes changes that revert it to its non-pregnant state."
- Textbook of Family Medicine, 9e: "These changes are normal and should not be confused with a pathologic condition."
Physiological Changes
Uterine Involution
| Time Postpartum | Uterine Position / State |
|---|---|
| Immediately after delivery | Near level of umbilicus (~1000 g) |
| 5-7 days | Firm, nontender, midway between symphysis and umbilicus |
| 2 weeks | No longer palpable abdominally; returned to the true pelvis |
| 6 weeks | Returns to normal non-pregnant mass (~50 g); involution complete |
- Uterine contractions ("afterpains") during involution are often painful and may require analgesics
- Breastfeeding promotes uterine contraction and involution by stimulating oxytocin release
- The gravid uterus increases from ~50 g to ~1000 g during pregnancy due to hypertrophy of myometrial smooth muscle, increased blood vessels, and tissue fluid
Lochia (Vaginal Discharge)
| Phase | Timing | Character |
|---|---|---|
| Lochia rubra | Days 1-4 | Grossly bloody (red) |
| Lochia serosa | Days 4-10 | Serous, pinkish-brown, decreasing amount |
| Lochia alba | Days 7-10 onwards | Pale yellow-white, minimal volume |
Haematological Changes
- Leukocytosis up to 20,000/μL within the first 24 hours (normal physiological response - do not confuse with infection)
- Diuresis: marked urinary output as the 6-8 L of extra fluid acquired in pregnancy is mobilised; may transiently elevate haematocrit
- Pulse rate drops within the first 24 hours
- Temperature may be mildly elevated in the first 24 hours (but fever must prompt search for infection)
Lactation and Breasts
- Milk "let-down" begins in the first days; breasts may become engorged early
- In non-breastfeeding mothers: earliest ovulation at ~4 weeks postpartum, first menses typically 6-8 weeks; lactation suppressed by firm breast support and fluid restriction (symptoms last 3-5 days)
- In breastfeeding mothers: anovulation (lactational amenorrhoea) continues for approximately 10-12 weeks on average; influenced by frequency, duration, and supplemental feeding
- Contraception is needed as ovulation can occur as early as 2 weeks postpartum and conception has been reported at this time
Bladder
- Urine retention and bladder overdistension must be avoided
- Rapid diuresis occurs when oxytocin is discontinued after delivery
- Women must be monitored to prevent asymptomatic bladder overfilling
Menstruation
- Non-breastfeeding: first menses typically returns at 6-8 weeks
- Breastfeeding: typically 10-12 weeks, but highly variable
Management of the Normal Puerperium
Immediate (First Hour)
- Observe for 1 hour post-delivery of placenta
- Uterine massage every 15 minutes to ensure maintained contraction and prevent excess bleeding
- Active management of the third stage: early oxytocin administration (10 units IM or IV infusion), early cord clamping/cutting, and controlled cord traction - reduces PPH by two-thirds
- Initiate breastfeeding if desired
First 24 Hours
- Regular diet as soon as patient desires (after normal vaginal delivery)
- Full ambulation as soon as possible (reduces DVT risk)
- Showers encouraged; vaginal douching prohibited
- Episiotomy pain: hot sitz baths, analgesia (avoid meperidine/pethidine in breastfeeding due to long half-life of active metabolite in infants)
- Bladder monitoring; encourage voiding
- Laxatives if needed; bowel movement ideally before discharge
Discharge
- Rubella immunisation if non-immune (mandates delaying pregnancy 3 months)
- Rhesus immunisation: anti-D immunoglobulin if Rh-negative with Rh-positive infant
- Contraception counselling (see below)
6-Week Postnatal Check
- Assess uterine involution (should be complete)
- Screen for postpartum depression (Edinburgh Postnatal Depression Scale)
- Blood pressure, anaemia, breastfeeding, family planning
- Cervical smear if due
Contraception in the Puerperium
| Method | Timing / Notes |
|---|---|
| Combined oral contraceptive pill | Can start at discharge; low-dose oestrogen preferred; not recommended <21 days postpartum (increased VTE risk); use with caution in breastfeeding (may suppress lactation) - defer to >6 weeks |
| Progestogen-only pill / implant / injectable | Safe in breastfeeding; can start immediately postpartum |
| Diaphragm/cap | Fit only after complete involution at 6-8 weeks |
| Barrier methods (condoms, foams, jellies) | Use until diaphragm fitting or OCP started |
| IUD/IUS | Can be inserted immediately postpartum or deferred to 4-6 weeks |
| Lactational Amenorrhoea Method (LAM) | Effective only if exclusive breastfeeding + amenorrhoea + <6 months postpartum |
- Medroxyprogesterone acetate (DMPA) injectable: effective but may theoretically reduce milk supply if given immediately postpartum - communicate risk and support autonomous decision-making
Complications of the Puerperium
1. Postpartum Haemorrhage (PPH)
Definition:
- Primary PPH: blood loss >500 mL vaginal delivery or >1000 mL caesarean section within 24 hours (clinical definition: any bleeding causing/risking haemodynamic instability)
- Secondary PPH: excessive bleeding from 24 hours to 6 weeks after delivery
Causes - "4 Ts":
| Cause | Details |
|---|---|
| Tone (uterine atony - most common) | Overdistension (hydramnios, macrosomia, multiple pregnancy), prolonged/rapid labour, infection, high parity, uterine relaxants |
| Tissue | Retained placenta/membranes, placenta accreta |
| Trauma | Vaginal/cervical lacerations, uterine rupture (1 in 2000 deliveries), uterine inversion |
| Thrombin | Hereditary coagulopathy, DIC |
Management of uterine atony:
- Bimanual uterine massage + compression
- Oxytocin IV (10-30 units in 1L fluid) or IM (10 units) - first line
- Methylergonovine 0.2 mg IM every 2-4 hours - second line (contraindicated in hypertension - causes vasoconstriction)
- 15-methyl PGF2α (Hemabate) 0.25 mg IM every 15-90 minutes (max 8 doses) - prostaglandin, can cause bronchospasm
- Misoprostol (PGE1) - rectal/sublingual
- Balloon tamponade, surgical haemostasis, hysterectomy if refractory
2. Puerperal Sepsis
Definition: Infection of the genital tract within 3 weeks after delivery, accompanied by:
- Rise in temperature (>38°C on 2 of days 2-10 postpartum in classic definition)
- Tachycardia
- Foul-smelling lochia
- Lower abdominal pain and tenderness
Causes: Group A Streptococcus (S. pyogenes - most virulent, can cause rapidly progressive sepsis), E. coli, anaerobes, mixed flora
Types:
- Endometritis (most common)
- Pelvic peritonitis
- Septicaemia
Prevention: Strict asepsis before and during delivery, especially in domiciliary settings
3. Thrombophlebitis and Venous Thromboembolism (VTE)
- The puerperium is a high-risk period for VTE - hypercoagulable state persists up to 6 weeks postpartum
- Thrombophlebitis: infection of leg veins, often associated with varicose veins; leg becomes tender, pale, and swollen
- DVT / Pulmonary embolism: prophylactic anticoagulation indicated in high-risk women
- Combined hormonal contraceptives should be avoided <21 days postpartum and used with caution 21-42 days postpartum if VTE risk factors are present (WHO MEC Category 3-4)
4. Puerperal Mastitis and Breast Abscess
| Feature | Mastitis | Breast Abscess |
|---|---|---|
| Onset | Most commonly second postpartum week (milk stasis + retrograde infection) | Complicates ~3% of mastitis cases |
| Pathogens | Staphylococcus aureus (40%), E. coli, Streptococcus spp.; consider CA-MRSA | Same |
| Symptoms | Severe pain, swelling, redness, fever, chills, myalgias | Fluctuant, well-defined tender mass |
| Ultrasound | Hypoechoic fluid surrounding fat lobules - no discrete collection | Hypoechoic discrete fluid collection with absent vascular flow |
| Treatment | Analgesia + continued breastfeeding + anti-staphylococcal antibiotics (antistaphylococcal penicillin or cephalosporin) | US-guided drainage (first line); surgical drainage reserved for last resort; IV vancomycin if septic |
Note: Breastfeeding should continue through mastitis and abscess treatment unless antibiotic is contraindicated in newborns. Interrupting breastfeeding is not necessary.
5. Urinary Tract Infection
- Catheterisation during labour, bladder overdistension, and urinary stasis predispose
- Screen for and treat promptly
6. Sub-involution of the Uterus
- Failure of the uterus to involute at the expected rate
- Causes: infection, retained placental fragments
- Presents with prolonged lochia, uterine tenderness, uterus larger than expected for gestational age
- Treatment: antibiotics, surgical evacuation if retained products
Psychiatric Complications of the Puerperium
Postpartum Blues ("Baby Blues")
- Incidence: 40-80% of postpartum women
- Onset: Typically peaks at 4-5 days after delivery
- Features: Mild mood swings, tearfulness, irritability, anxiety, emotional lability, insomnia
- Duration: Self-limiting; usually resolves by day 10-14
- Management: Reassurance, support; no pharmacotherapy required
Postpartum Depression (PPD)
- Incidence: ~10% of childbearing women
- Onset: 24 hours to several months after delivery; can be abrupt
- Features: Persistent low mood, loss of interest, fatigue, poor concentration, guilt, lack of interest in or fear of harming the infant, suicidal/homicidal ideation
- Screening tool: Edinburgh Postnatal Depression Scale (EPDS) - 10-item self-report; score ≥13 likely indicates depression; Question 10 (self-harm intent) must be scrutinised regardless of total score
- Management: Psychotherapy, SSRIs (note: SSRIs used with caution in pregnancy given possible cardiac teratogenicity, but postpartum use is generally considered acceptable); referral to specialist
Postpartum Psychosis
- Incidence: ~0.1-0.25% of deliveries (Maudsley Guidelines)
- Onset: 48-72 hours (or longer) after delivery
- Features:
- Alternating noisy hyperactivity and mutism/inactivity
- Disorientation, thought disorder
- Perceptual abnormalities, hallucinations
- Rejection of infant ("this is not my baby")
- Suicidal and infanticidal thoughts - the most dangerous features
- Classification: ~40% predominantly affective, ~20% schizophreniform, remainder self-limited confusional psychoses
- Differential diagnosis: Eclampsia, Sheehan syndrome (pituitary infarction), cerebral venous thrombosis, arterial stroke, ergot-induced psychosis, hypoxic/hypotensive cerebral injury
- Management: Urgent psychiatric assessment; antipsychotics, mood stabilisers; ergotamine must be excluded; hospitalisation usually required - never leave mother alone with infant
Puerperal Care Summary (Public Health / Postnatal Visits)
Objectives of postnatal care (Park's Preventive Medicine):
- Prevent complications (puerperal sepsis, thrombophlebitis, secondary haemorrhage)
- Restore mother to optimum health (physical and emotional recuperation)
- Establish and support breastfeeding
- Provide family planning services
- Health education
Postnatal examination schedule:
- Twice daily for first 3 days, then daily until cord drops off (neonatal)
- Maternal: at each visit - temperature, pulse, respiration, breast examination, uterine involution, lochia assessment, urinary/bowel function, perineal/episiotomy care
- 6-week check: Complete involution, haemoglobin, blood pressure, family planning, depression screening
- Monthly thereafter for 6 months, then 2-3 monthly to 1 year in high-risk settings
Key Points at a Glance
| Feature | Key Fact |
|---|---|
| Duration | 6 weeks (third stage of labour to complete involution) |
| Leukocytosis | Up to 20,000/μL in first 24 h - physiological, not infective |
| Lochia sequence | Rubra → Serosa → Alba |
| Uterine involution | Completed at 6 weeks; not palpable abdominally at 2 weeks |
| First ovulation (non-BF) | ~4 weeks; conception possible as early as 2 weeks |
| PPH (most common cause) | Uterine atony |
| First-line PPH treatment | Bimanual compression + oxytocin |
| Most common infection | Endometritis / puerperal sepsis (Group A Strep most virulent) |
| Mastitis causative organism | S. aureus (40%) |
| Baby blues | 40-80%; resolves by day 10 |
| PPD screening tool | Edinburgh Postnatal Depression Scale (EPDS) |
| Postpartum psychosis | ~0.1-0.25%; onset 48-72h; infanticidal risk - psychiatric emergency |
Sources: Textbook of Family Medicine 9e | Gray's Anatomy for Students | Park's Textbook of Preventive & Social Medicine | Tintinalli's Emergency Medicine | Adams & Victor's Principles of Neurology 12E | Creasy & Resnik's Maternal-Fetal Medicine | Maudsley Prescribing Guidelines in Psychiatry 15e
This is a shared conversation. Sign in to Orris to start your own chat.