
Treatment plan, cause
"communicating hydrocephalus" treatment
CT Report Summary
What is Communicating Hydrocephalus?
Causes of Communicating Hydrocephalus
| Cause | Details |
|---|---|
| Post-haemorrhagic | Following subarachnoid or intraventricular hemorrhage; blood products clog arachnoid villi |
| CSF infection (meningitis) | Inflammatory exudate impairs CSF reabsorption; most common cause in young adults in endemic regions |
| Raised CSF protein | Elevated protein viscosity hinders absorption at arachnoid granulations |
- Tuberculous meningitis (TBM) - common in South Asia (Jammu/Kashmir region context here), causes exudative arachnoiditis blocking reabsorption
- Bacterial/viral meningitis (post-infectious)
- Subarachnoid hemorrhage (though no bleed visible on this plain CT)
- Idiopathic - no underlying cause found
- Previous head trauma
- Choroid plexus papilloma (rare, but causes excess CSF production)
Treatment Plan
1. Immediate Investigations (to find the cause)
- Lumbar puncture - confirms raised opening pressure, sends CSF for culture, sensitivity, protein, glucose, cytology (safe in communicating hydrocephalus, unlike obstructive)
- MRI Brain with contrast - better than plain CT for identifying the underlying cause (arachnoiditis, meningeal enhancement, tumour)
- Bloods - CBC, ESR, CRP, blood cultures, TB workup (Mantoux/IGRA), ADA levels
- CSF ADA + AFB smear/culture - rule out TB
2. Emergency/Acute Management
- If raised intracranial pressure (ICP) is symptomatic:
- External ventricular drain (EVD) - first-line for acute CSF diversion
- Lumbar puncture can also relieve pressure temporarily (drain 10-30 mL CSF)
- Acetazolamide - carbonic anhydrase inhibitor, reduces CSF production; can be used as a temporizing measure
3. Definitive Surgical Treatment
- Ventriculoperitoneal (VP) shunt - the standard surgical treatment; diverts CSF from lateral ventricle to peritoneal cavity for absorption
- Ventriculoatrial (VA) shunt - alternative if VP shunt not feasible
- Lumboperitoneal shunt - alternative for communicating hydrocephalus specifically
- Endoscopic Third Ventriculostomy (ETV) - less effective in communicating hydrocephalus (works better in obstructive type), but may be tried
4. Treat the Underlying Cause
- If TB meningitis: Start anti-TB therapy (HRZE regimen x 2 months, then HR x 10 months) + dexamethasone (reduces meningeal inflammation and improves shunt outcomes)
- If bacterial meningitis: IV antibiotics per culture sensitivity
- If IIH-like: Acetazolamide + weight management
Key Clinical Points for This Patient
- Plain CT is the first-line investigation - confirmed here. Next step is MRI with contrast.
- Lumbar puncture is safe in communicating hydrocephalus (unlike obstructive) and is both diagnostic and temporarily therapeutic.
- Given the geographic context (Rajouri, J&K) and age group, tuberculous meningitis must be actively ruled out - it is a leading cause of communicating hydrocephalus in young adults in this region.
- The treating neurosurgeon (at GMCR - Government Medical College Rajouri) will decide between VP shunt insertion vs. temporizing measures based on ICP, clinical symptoms, and the underlying etiology.
Important: This analysis is for educational purposes only. The patient must be evaluated by the referring neurosurgeon and neurology team at GMCR for individualized management. Clinical symptoms (headache, vomiting, vision changes, gait) must guide urgency of intervention.
Create a management flowchart for communicating hydrocephalus
A clean, professional medical management flowchart for Communicating Hydrocephalus. The flowchart should follow a top-to-bottom flow with clearly labeled boxes and arrows. Include the following steps in order: 1. TOP BOX (teal/blue header): "COMMUNICATING HYDROCEPHALUS" subtitle "CT: Bilateral lateral + 3rd + 4th ventricle dilatation, No obstruction" 2. FIRST DECISION DIAMOND: "Symptomatic? (Headache, vomiting, papilledema, altered consciousness)" - YES arrow → Emergency Management box - NO arrow → Investigations box 3. EMERGENCY MANAGEMENT BOX (red/orange): - External Ventricular Drain (EVD) - Lumbar Puncture (drain 10–30 mL CSF) - Acetazolamide (reduce CSF production) → Arrow down to Investigations 4. INVESTIGATIONS BOX (blue): - MRI Brain with contrast - Lumbar Puncture: Opening pressure, CSF analysis (protein, glucose, cells) - CSF: AFB smear, ADA, culture & sensitivity - Blood: CBC, ESR, CRP, TB workup (IGRA/Mantoux) → Arrow to "Identify Underlying Cause" 5. IDENTIFY UNDERLYING CAUSE BOX (purple): Three branches side by side: - TB Meningitis → Anti-TB therapy (HRZE x2m + HR x10m) + Dexamethasone - Bacterial/Viral Meningitis → IV Antibiotics / Antivirals - Idiopathic / Post-hemorrhagic / High protein → Symptom management All three branches merge back down 6. DEFINITIVE SURGICAL TREATMENT BOX (green header): "Does hydrocephalus persist or ICP remain elevated?" - YES → Surgical Options (3 boxes side by side): * Ventriculoperitoneal (VP) Shunt — PREFERRED * Lumboperitoneal Shunt — alternative * Ventriculoatrial (VA) Shunt — if VP not feasible - NO → Conservative follow-up 7. FOLLOW-UP BOX (grey): - Regular clinical review - Repeat MRI/CT at 3 months - Monitor shunt function - Visual acuity checks (papilledema resolution) Use medical blue, teal, green, and soft red/orange color coding. Clean sans-serif font. Professional hospital-grade diagram style. White background. Clear arrows between all steps.
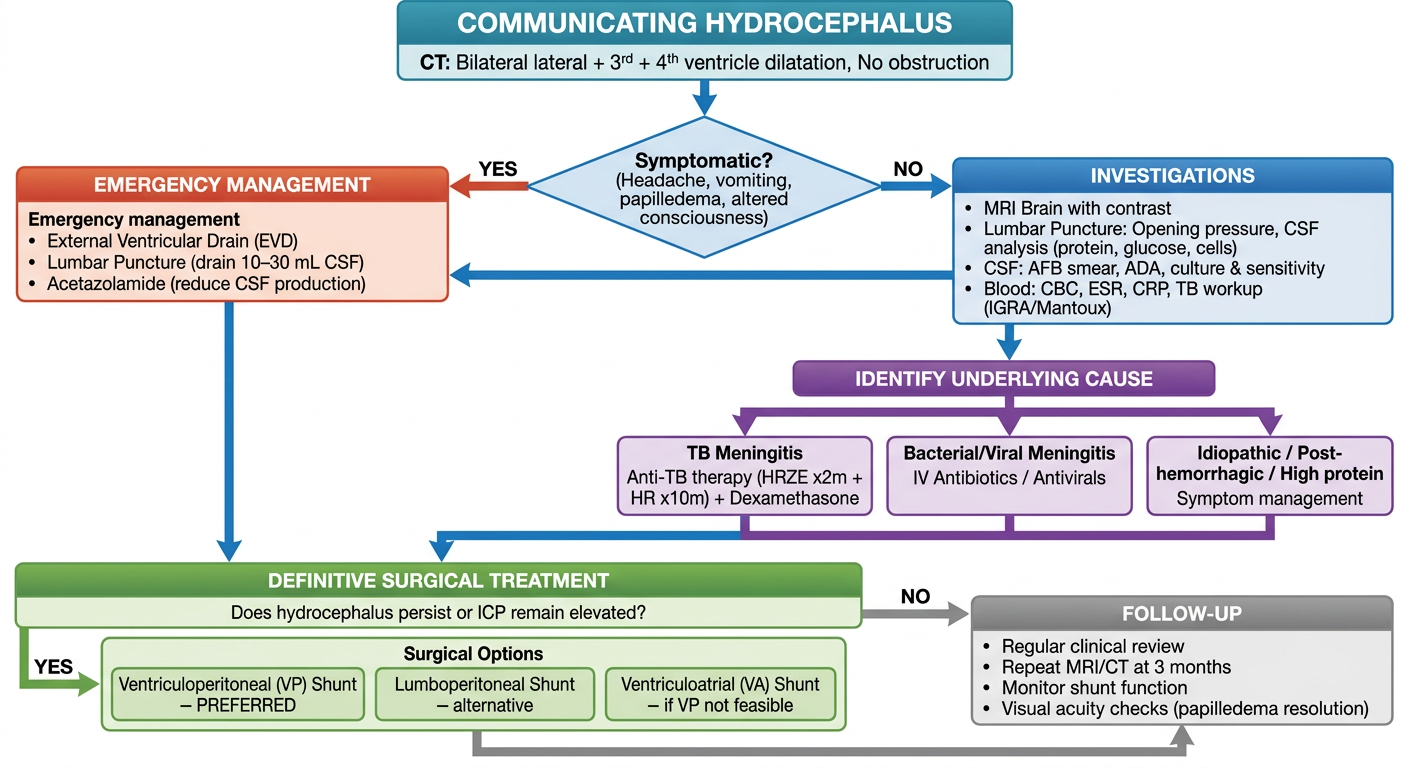
- Initial Assessment - Symptom triage (is the patient in acute distress?)
- Emergency Management - EVD, LP drainage, Acetazolamide if symptomatic
- Investigations - MRI, LP analysis, TB workup, bloods
- Cause Identification - TB meningitis, bacterial/viral meningitis, or idiopathic/post-hemorrhagic
- Cause-Specific Treatment - Anti-TB therapy with steroids, antibiotics, or supportive care
- Definitive Surgery - VP shunt (preferred), lumboperitoneal shunt, or VA shunt based on persistence of hydrocephalus
- Follow-up - Repeat imaging, shunt monitoring, visual checks