
image.jpg
Prepare an laq for mbbs first year for fourth ventricle
Reading File
Finding Sources
Searching Images
fourth ventricle floor roof boundaries anatomy diagram
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Now I have all the material needed. Here is the complete, exam-ready LAQ for MBBS First Year:
FOURTH VENTRICLE — Long Answer Question (MBBS First Year Anatomy)
Introduction
The fourth ventricle is a diamond-shaped (rhomboid) cavity of the hindbrain, lined with ependyma and filled with cerebrospinal fluid (CSF). It is the most caudal ventricle of the brain, situated in the posterior cranial fossa between the brainstem anteriorly and the cerebellum posteriorly.
Location
The fourth ventricle lies in the posterior cranial fossa, situated:
- Anteriorly (floor): pons above and medulla oblongata below
- Posteriorly (roof): cerebellum
Boundaries / Extent
The ventricle extends from the cerebral aqueduct (of Sylvius) above to the central canal of the spinal cord below.
FLOOR (Rhomboid Fossa)
The floor is rhombus-shaped (hence the name rhomboid fossa) and is formed by:
- Upper triangular part → posterior surface of the pons
- Lower triangular part → posterior surface of the upper half of the medulla oblongata
The floor is divided into symmetric halves by a median sulcus.
Features of the Floor
A. Median Sulcus — runs craniocaudally along the midline.
B. Medial Eminence (Eminentia Medialis) — lies on each side of the median sulcus; contains:
- Facial colliculus (pontine part) — overlies the nucleus of abducens nerve (CN VI) looped around by the facial nerve (CN VII) fibres
- Hypoglossal triangle (trigonum hypoglossi) — overlies the nucleus of CN XII
- Vagal triangle (trigonum vagi) — overlies the dorsal nucleus of vagus (CN X)
C. Sulcus Limitans — lateral to medial eminence; separates sensory (lateral) from motor (medial) columns.
D. Superior Fovea — depression in the sulcus limitans at the pontine level.
E. Inferior Fovea — depression in the sulcus limitans at the medullary level.
F. Area Vestibularis (Acoustic Area) — lateral to the sulcus limitans in the pontine part; overlies the vestibular nuclei.
G. Area Postrema — paired triangular areas near the obex; chemoreceptor trigger zone (vomiting centre).
H. Striae Medullares — transverse fibre bundles crossing the floor from the median sulcus to the lateral recess; divide the floor into pontine and medullary parts.
I. Obex — a small tongue of tissue at the inferior angle of the rhomboid fossa; marks the transition to the central canal.
J. Calamus Scriptorius ("writing pen") — the inferior triangular part of the floor, so named because its shape resembles the tip of a quill pen.
ROOF
The roof is tent-shaped and has two parts:
Superior Part (Anterior Medullary Velum)
- Thin sheet of white matter
- Stretches between the two superior cerebellar peduncles
- The decussation of the trochlear nerve (CN IV) occurs within it
- Thin → pathological stretching here causes dorsal midbrain compression signs
Inferior Part (Posterior Medullary Velum)
- Formed by two thin sheets of white matter
- Completed by the tela choroidea (a double layer of pia) and the choroid plexus of the fourth ventricle
- The tela choroidea hangs down like a tent, and the choroid plexus projects into the ventricle as a T-shaped structure
LATERAL BOUNDARIES
The lateral boundaries of the fourth ventricle are formed on each side by the:
- Inferior cerebellar peduncle (restiform body) — upper part
- Gracile tubercle and cuneate tubercle — lower part
The lateral recesses are the wing-like lateral extensions that project toward the cerebellar flocculus. Each ends at the foramen of Luschka (lateral aperture).
COMMUNICATIONS / APERTURES (Foramina)
CSF escapes from the fourth ventricle into the subarachnoid space through three apertures:
| Foramen | Position | Opens into |
|---|---|---|
| Foramen of Magendie (median aperture) | Midline, in the inferior part of roof | Cerebellomedullary cistern (cisterna magna) |
| Foramen of Luschka (lateral aperture) × 2 | Tips of lateral recesses | Pontine cistern (subarachnoid space) |
- Above: communicates with the third ventricle via the cerebral aqueduct (of Sylvius)
- Below: continuous with the central canal of the spinal cord via the obex
CHOROID PLEXUS
The choroid plexus of the fourth ventricle lies in the roof (inferior medullary velum + tela choroidea). It produces CSF and is supplied by the posterior inferior cerebellar artery (PICA).
BLOOD SUPPLY
| Structure | Artery |
|---|---|
| Floor (pons part) | Basilar artery branches (AICA — anterior inferior cerebellar artery) |
| Floor (medullary part) | Vertebral artery branches (PICA — posterior inferior cerebellar artery) |
| Roof/Choroid plexus | PICA |
CSF CIRCULATION (Related to 4th Ventricle)
Lateral ventricles → (foramen of Monro) → Third ventricle → (aqueduct of Sylvius) → Fourth ventricle → (foramen of Magendie + foramina of Luschka) → Subarachnoid space → absorbed via arachnoid granulations into dural venous sinuses.
APPLIED ANATOMY (Clinical Correlations)
-
Hydrocephalus — Obstruction of the cerebral aqueduct or blockage of the foramina of Magendie/Luschka prevents CSF outflow from the fourth ventricle → non-communicating (obstructive) hydrocephalus → raised intracranial pressure.
-
Dandy-Walker Malformation — Developmental failure of the foramen of Magendie (and sometimes Luschka) to open → cystic dilatation of the fourth ventricle + cerebellar vermis hypoplasia + enlarged posterior fossa.
-
Medulloblastoma — Most common posterior fossa tumour in children; arises from undifferentiated neuroectodermal cells of the roof (superior/inferior medullary velum, vermis) of the fourth ventricle → compresses and fills the ventricle → obstructive hydrocephalus.
-
Ependymoma of the 4th Ventricle — Arises from the ependymal lining of the ventricular floor; tends to squeeze out through the foramen of Magendie ("plastic" ependymoma).
-
Area postrema lesions — The area postrema is outside the blood-brain barrier (a circumventricular organ). Damage or stimulation causes vomiting. It is a target for antiemetic drugs (e.g., ondansetron) and is affected in conditions like neuromyelitis optica spectrum disorder (NMOSD), causing intractable hiccups and vomiting.
-
PICA occlusion (Lateral medullary/Wallenberg syndrome) — The PICA supplies the lateral medulla and the inferior fourth ventricle. Occlusion causes ipsilateral cerebellar signs, crossed sensory loss, Horner syndrome, dysphagia, and nystagmus.
-
Tumours of the 4th ventricle — Can present with cerebellar dysfunction (ataxia, nystagmus, dysmetria) due to compression of the cerebellar peduncles, along with features of raised ICP (headache, vomiting, papilloedema).
-
Nystagmus — The vestibular nuclei lying in the floor → tumours/inflammation in the floor cause nystagmus, vertigo, and disequilibrium.
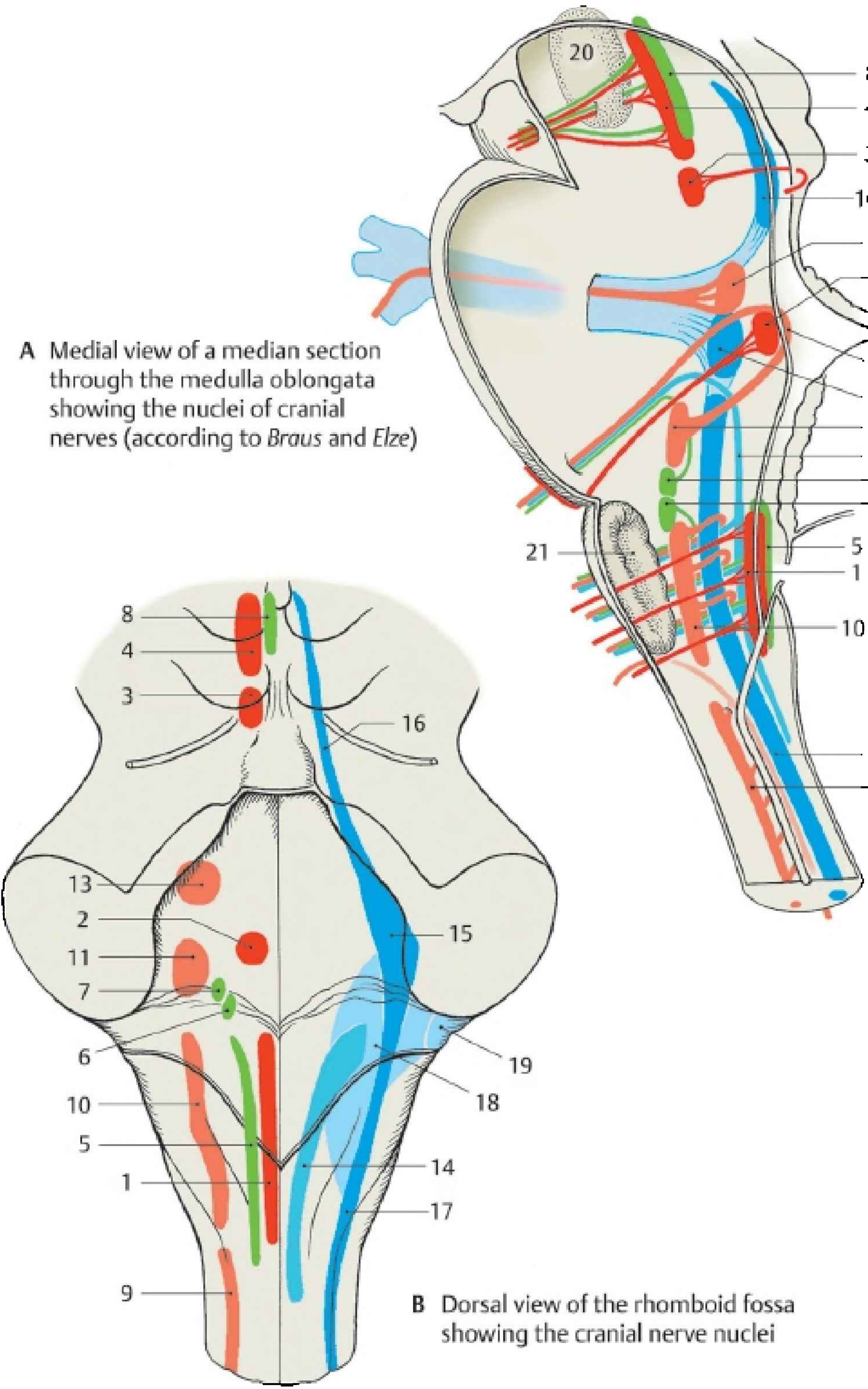
DIAGRAM
Key landmarks: (1) Obex, (2) Area postrema, (3) Trigonum hypoglossi, (4) Area acustica, (5) Trigonum vagi, (6) Striae medullares, (7) Taenia of the 4th ventricle
SUMMARY TABLE
| Feature | Detail |
|---|---|
| Shape | Diamond / rhomboid |
| Location | Posterior cranial fossa |
| Floor | Rhomboid fossa (pons + medulla) |
| Roof | Ant. medullary velum (sup.) + Post. medullary velum + tela choroidea (inf.) |
| Lateral boundary | Inferior & superior cerebellar peduncles |
| Median aperture | Foramen of Magendie → cisterna magna |
| Lateral aperture | Foramen of Luschka (×2) → pontine cistern |
| CSF production | Choroid plexus (supplied by PICA) |
| Lined by | Ependyma |
| Key landmark | Facial colliculus, striae medullares, obex, calamus scriptorius, area postrema |
Sources: Gray's Anatomy for Students; Medical Physiology (Boron & Boulpaep); Color Atlas of Human Anatomy Vol. 3 (Brain Stem & Cranial Nerves); Neuroanatomy through Clinical Cases 3rd Ed.
The question comes as decribe parts boundaries of 4th ventricle
The question comes as describe parts boundaries of fourth ventricle or describe the flow of the fourth ventricle, which is basically the ovoid. Please make it in such a way easy way that I can cover all the points and score code marks prepare answer in that way, this is for anatomy.
Here is a focused, mark-scoring LAQ answer tailored exactly for "Describe the parts and boundaries of the Fourth Ventricle" — structured the way anatomy examiners expect.
FOURTH VENTRICLE — Parts and Boundaries
(MBBS First Year Anatomy — LAQ)
1. INTRODUCTION (2–3 lines — always write this)
The fourth ventricle is a diamond-shaped (rhomboid) cavity situated in the posterior cranial fossa. It is lined by ependyma and filled with cerebrospinal fluid (CSF). It lies between the brainstem anteriorly and the cerebellum posteriorly.
2. PARTS OF THE FOURTH VENTRICLE
The fourth ventricle has 4 parts:
| Part | Description |
|---|---|
| Floor | Rhomboid fossa |
| Roof | Tent-shaped; superior + inferior parts |
| Lateral boundaries | Two sides of the diamond |
| Lateral recesses | Wing-like projections |
3. FLOOR (Rhomboid Fossa) — Most Important Part ⭐
The floor is rhombus-shaped and is formed by:
- Upper triangular part → posterior surface of pons
- Lower triangular part → posterior surface of upper medulla oblongata
Features of the Floor (Learn these — high yield):
Median sulcus — runs along the midline, top to bottom
Medial eminence — on each side of median sulcus:
- Facial colliculus (pontine part) → nucleus of CN VI + fibres of CN VII loop around it
- Hypoglossal triangle → nucleus of CN XII below
- Vagal triangle → dorsal nucleus of CN X
Sulcus limitans — lateral groove separating motor (medial) from sensory (lateral) areas:
- Superior fovea — depression at pontine level
- Inferior fovea — depression at medullary level
Area vestibularis — lateral to sulcus limitans; overlies vestibular nuclei
Striae medullares — transverse fibres crossing the floor; divide it into pontine and medullary parts
Area postrema — near the obex; chemoreceptor trigger zone (vomiting centre); outside BBB
Obex — small tissue tag at the inferior angle; marks transition to central canal
Calamus scriptorius — inferior triangular part; shaped like tip of a writing pen
4. ROOF (Tent-shaped) ⭐
Superior part — Anterior Medullary Velum
- Thin sheet of white matter
- Bridges the two superior cerebellar peduncles
- Trochlear nerve (CN IV) decussates within it
Inferior part — Posterior Medullary Velum + Tela Choroidea
- Two thin crescentic sheets of white matter
- Completed by tela choroidea (double fold of pia mater)
- Choroid plexus hangs from here → produces CSF
- Has a central opening = Foramen of Magendie (median aperture)
5. LATERAL BOUNDARIES
Each lateral boundary is formed (from above downward) by:
- Superior cerebellar peduncle (upper part)
- Inferior cerebellar peduncle (restiform body) (middle part)
- Gracile tubercle + Cuneate tubercle (lower part)
6. LATERAL RECESSES
- The ventricle extends laterally as two lateral recesses
- They curve around the brainstem toward the cerebellar flocculus
- Each lateral recess opens at its tip as the Foramen of Luschka (lateral aperture)
7. COMMUNICATIONS / APERTURES (Floor of CSF Flow) ⭐
This is the "describe the floor of the 4th ventricle / CSF flow" part examiners ask:
| Opening | Location | Opens Into |
|---|---|---|
| Foramen of Magendie (1) | Midline inferior roof | Cisterna magna (cerebellomedullary cistern) |
| Foramen of Luschka (×2) | Tips of lateral recesses | Pontine cistern (subarachnoid space) |
| Cerebral aqueduct | Superior apex | Third ventricle (above) |
| Central canal | Inferior apex via obex | Spinal cord (below) |
8. CSF FLOW THROUGH THE 4TH VENTRICLE
(For the question "describe the floor/flow of the 4th ventricle")
Lateral ventricles → Foramen of Monro → Third ventricle → Aqueduct of Sylvius → Fourth ventricle → Foramen of Magendie (midline) + Foramina of Luschka (×2) → Subarachnoid space → Arachnoid granulations → Dural venous sinuses → Blood
9. APPLIED ANATOMY (Write 2–3 — gives extra marks)
1. Hydrocephalus — Obstruction of the aqueduct or foramina of Magendie/Luschka → CSF accumulates → raised ICP (non-communicating hydrocephalus)
2. Medulloblastoma — Most common posterior fossa tumour in children; arises from the roof → fills the 4th ventricle → obstructive hydrocephalus
3. Dandy-Walker malformation — Failure of foramen of Magendie to open → cystic dilation of 4th ventricle + cerebellar hypoplasia
4. Area postrema — Outside the BBB; stimulated by toxins/drugs → vomiting (target of antiemetics like ondansetron)
10. DIAGRAM (Draw in exam — easy, earns marks)
Cerebral aqueduct (above)
↓
┌─────────────────────────────┐
│ Superior cerebellar peduncle│ ← Lateral boundary (upper)
│ │
│ FLOOR (Rhomboid Fossa) │
│ ┌─────────────────────┐ │
│ │ Facial colliculus │ │
│ │ Striae medullares │ │
│ │ Vagal/XII triangle │ │
│ │ Area postrema/Obex │ │
│ └─────────────────────┘ │
│ Inferior cerebellar ped. │ ← Lateral boundary (lower)
└─────────────────────────────┘
↓
Central canal (below)
ROOF: Ant. medullary velum (sup.) + Post. medullary velum + Tela choroidea (inf.)
OPENINGS: Foramen of Magendie (midline) + Foramina of Luschka (×2 lateral)
HOW TO SCORE FULL MARKS — Quick Checklist
- Introduction (shape, location, lining) — 2 marks
- Floor + named features (facial colliculus, striae, obex, area postrema) — 4 marks
- Roof (ant. + post. medullary velum, tela choroidea) — 3 marks
- Lateral boundaries (3 structures each side) — 2 marks
- Apertures/communications (Magendie, Luschka, aqueduct, central canal) — 3 marks
- CSF flow — 2 marks
- Applied anatomy (2–3 points) — 2 marks
- Diagram — 2 marks
Total: ~20 marks
Tip: Examiners love when you mention the facial colliculus and explain why it matters (CN VI nucleus + CN VII fibres loop around it) — it shows conceptual clarity, not just rote learning. Similarly, explaining area postrema = outside BBB = vomiting centre gets you extra marks every time.
But the answer you gave here is not the way it’s there in my textbook
Loading Image
I can now read your textbook clearly. This is Textbook of Anatomy, Head, Neck and Brain (the standard BV Datta / Vishram Singh style). Let me now give you the answer exactly in the sequence and language your textbook uses.
FOURTH VENTRICLE
(As per your Textbook — Anatomy LAQ)
INTRODUCTION
The 4th ventricle is a diamond-shaped cavity of the hindbrain, lined with ependyma and filled with cerebrospinal fluid (CSF). It is situated in the posterior cranial fossa, between the brainstem anteriorly and the cerebellum posteriorly.
BOUNDARIES
Your textbook divides the boundaries as:
1. ROOF (Posterior Wall) ⭐
The roof is tent-shaped and has:
A. Superior part:
- Formed by the superior medullary velum (anterior medullary velum)
- It is a thin sheet of white matter stretching between the two superior cerebellar peduncles
B. Inferior part:
- Formed by the inferior medullary velum — a thin sheet of nervous tissue
- Completed by the tela choroidea — a double layer of pia mater
- The choroid plexus of the 4th ventricle is carried by the tela choroidea
- The cavity of the 4th ventricle communicates with the subarachnoid space through the foramen of Magendie (median aperture) in the midline, and through the foramina of Luschka (lateral apertures) on each side
- The choroid plexus receives blood supply from the posterior inferior cerebellar artery (PICA)
2. LATERAL BOUNDARIES ⭐
On each side, the lateral boundaries are formed by:
- Superior cerebellar peduncle — upper part
- Inferior cerebellar peduncle — lower part (restiform body)
The horizontal limb of the lateral recess (where the superior and inferior cerebellar peduncles meet) is T-shaped. The lateral recess extends laterally and opens as the foramen of Luschka into the subarachnoid space.
3. FLOOR (Rhomboid Fossa) ⭐⭐ Most Important
The floor is rhombus-shaped (hence "rhomboid fossa"). It is formed by:
- Upper part → posterior surface of pons
- Lower part → posterior surface of upper medulla oblongata
FLOOR OF THE 4TH VENTRICLE — FEATURES
(Your textbook lists these features of the rhomboid fossa)
Features of the floor from above downward:
Sulcus Limitans
- Runs along each side of the floor
- Divides the floor into medial (motor) and lateral (sensory) parts
Medial Eminence
- Lies medial to the sulcus limitans
- In the pontine part: contains the facial colliculus — a rounded elevation produced by fibres of CN VII looping over the nucleus of CN VI (abducens nucleus)
- In the medullary part: contains the hypoglossal triangle (overlies CN XII nucleus) and vagal triangle (overlies dorsal nucleus of CN X)
Striae Medullares
- Transverse fibres that cross the floor from the median sulcus to the lateral recesses
- Divide the floor into pontine (upper) and medullary (lower) parts
Area Vestibularis
- Lateral to the sulcus limitans in the pontine part
- Overlies the vestibular nuclei
Area Postrema
- Triangular area at the lower end of the floor, near the obex
- Chemoreceptor trigger zone — outside the blood-brain barrier
Obex
- Small plate of nervous tissue at the inferior angle of the rhomboid fossa
- Marks the junction of the 4th ventricle with the central canal of the spinal cord
Calamus Scriptorius
- The inferior triangular part of the floor
- Resembles the tip of a writing pen ("calamus" = pen)
- Bounded below by the obex
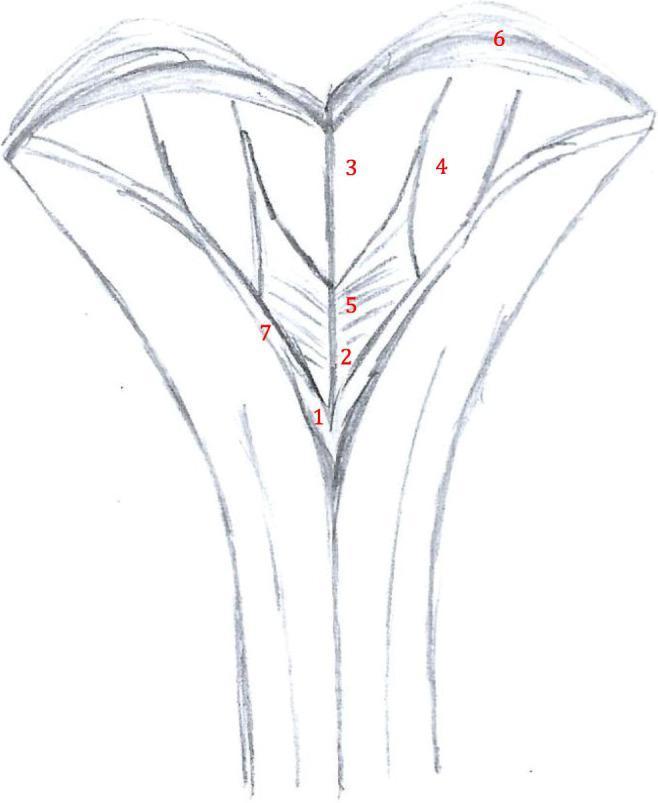
FIGURE FROM YOUR TEXTBOOK
(Fig 25.5 as shown in your book — Rhomboid fossa floor of the 4th ventricle)
Labels from your book's diagram:
- Median sulcus
- Facial colliculus — Superior fovea
- Striae medullares
- Sulcus limitans
- Hypoglossal triangle — Inferior fovea
- Vagal triangle
- Area postrema
- Obex
- Taenia
- Funiculus separans
CHOROID PLEXUS OF THE 4TH VENTRICLE
(Your textbook has a dedicated section on this)
- The choroid plexus is a tuft of capillaries that project into the cavity of the 4th ventricle
- It enters the 4th ventricle through the roof (tela choroidea)
- Through these three apertures (Magendie + 2× Luschka), the plexus opens the subarachnoid space of the lateral aperture (foramen of Luschka) into the subarachnoid space and the foramen of Magendie around the arachnoid space
- The entire plexus of the 4th ventricle is T-shaped, where the horizontal limb of T is double — one on each side entering the lateral recess and protruding through the foramen of Luschka into the subarachnoid space
APPLIED ANATOMY / CLINICAL CORRELATIONS
(from your textbook's Clinical Correlation box)
Tumours of the 4th Ventricle:
- Tumours in this region are not gliomas
- The glioma which occurs rarely in this region is ependymoma
- More common tumours are poorly differentiated primitive neuroectodermal tumours (medulloblastoma)
- The glioma in this region is a hazard, strongly associated with hydrocephalus because tumours can obstruct CSF flow
- The glioma which forms in this region may cause obstructions, leading to disorders of respiration and vasomotor disturbances
- Upon the ventricular floor (rhomboid fossa), tumours become tightly bound there secondarily
- This may lead to formation of internal hydrocephalus
COMMUNICATIONS OF THE 4TH VENTRICLE
| Opening | Where | Opens Into |
|---|---|---|
| Aqueduct of Sylvius | Superior apex (above) | 3rd ventricle |
| Foramen of Magendie | Midline of roof (inferior) | Cisterna magna |
| Foramina of Luschka ×2 | Tips of lateral recesses | Pontine cistern (subarachnoid space) |
| Central canal | Inferior apex via obex | Spinal cord |
HOW TO WRITE IN EXAM — SEQUENCE TO FOLLOW
Follow this exact order — same as your textbook:
- Introduction (diamond-shaped, posterior cranial fossa)
- Boundaries — heading first:
- Roof (superior part + inferior part)
- Lateral boundaries
- Floor (rhomboid fossa)
- Features of the floor (sulcus limitans → medial eminence → striae medullares → area vestibularis → area postrema → obex → calamus scriptorius)
- Choroid plexus (T-shaped, PICA supply, apertures)
- Communications (table or list)
- Applied anatomy (2–3 points from clinical correlation box)
- Diagram of rhomboid fossa
This sequence mirrors your textbook exactly and will get you full marks.
This is a shared conversation. Sign in to Orris to start your own chat.