Nitroglycerin - therapeutic uses, routes of administration, adverse effects moa,precaution 2. Coronary Steal Phenomenon - explain, clinical significance precaution 3. Nifedipine and Verapamil - compare and contrast 4. Nitrates - MOA theraputic uses adverse effect precautions
2mbbs pharmacology refer kd t
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have all the content I need for a thorough 2nd MBBS pharmacology answer. Let me compile the comprehensive response.
2nd MBBS Pharmacology - Cardiovascular Drugs
Sources: Goodman & Gilman's Pharmacological Basis of Therapeutics, Lippincott Illustrated Reviews: Pharmacology, Katzung's Basic & Clinical Pharmacology, Braunwald's Heart Disease
1. Nitroglycerin (Glyceryl Trinitrate / GTN)
Mechanism of Action
Nitroglycerin is an organic nitrate that acts as a nitric oxide (NO) donor. The key steps are:
- GTN enters vascular smooth muscle and is converted to NO (bioactivation requires mitochondrial aldehyde dehydrogenase, ALDH2).
- NO activates soluble guanylyl cyclase (sGC), which converts GTP to cGMP.
- Elevated cGMP activates protein kinase G (PKG), which:
- Reduces myosin light chain kinase (MLCK) activity
- Increases myosin light chain phosphatase activity
- Reduces intracellular Ca²⁺
- Result: vascular smooth muscle relaxation and vasodilation
Selectivity: At low/therapeutic doses, GTN preferentially dilates venous capacitance vessels (preload reduction) and large conductance coronary arteries. At higher doses, arteriolar dilation also occurs (afterload reduction).
Antianginal MOA - Reduction of O₂ Demand
The dominant antianginal effect is NOT increased O₂ delivery - it is reduced O₂ demand:
| Effect | Mechanism | Benefit |
|---|---|---|
| Venodilation | Reduced venous return → decreased preload (↓LVEDP, ↓wall tension - Law of Laplace) | ↓ O₂ consumption |
| Arteriodilation (higher doses) | Decreased peripheral resistance → ↓afterload | ↓ Cardiac work |
| Coronary dilation | Dilates large epicardial arteries, relieves coronary vasospasm | ↑ O₂ delivery in Prinzmetal's angina |
| Subendocardial perfusion | Reduced LVEDP increases transmural perfusion pressure gradient | Favors subendocardial blood flow |
Key fact: When GTN is injected directly into the coronary artery, it does NOT abort anginal pain, confirming that its major effect is preload reduction, not direct coronary dilation. - Goodman & Gilman
Therapeutic Uses
- Stable angina (exertional) - sublingual GTN for acute relief
- Unstable angina (ACS) - IV nitroglycerin for ongoing ischemia
- Vasospastic (Prinzmetal's) angina - directly relieves coronary spasm
- Acute left ventricular failure / pulmonary edema - venodilation reduces preload and pulmonary congestion; IV dose 20-400 µg/min
- Hypertensive emergencies - IV nitroglyerin for BP control
- Acute MI - reduces preload and myocardial O₂ demand
- Esophageal spasm - smooth muscle relaxation (diagnostic/therapeutic)
Routes of Administration
| Route | Form | Onset | Duration | Use |
|---|---|---|---|---|
| Sublingual | Tablet / spray | 1-3 min | 15-30 min | Acute angina attack |
| Buccal/transmucosal | Tablet | 2-3 min | 3-5 hours | Short-term prophylaxis |
| Oral | Sustained release | 30-60 min | 8-12 hours | Prophylaxis |
| Transdermal patch | Patch | 30-60 min | 24 hours (apply 12h/day) | Prophylaxis |
| Topical ointment | 2% ointment | 15-30 min | 4-8 hours | Prophylaxis |
| Intravenous | Infusion | Immediate | Infusion-dependent | Acute HF, ACS, hypertensive emergency |
Note: The sublingual spray may act even faster than the sublingual tablet.
Adverse Effects
- Headache - most common; due to meningeal arterial dilation. Usually decreases after a few days of continued use.
- Postural hypotension / dizziness / weakness - reflex tachycardia may occur
- Flushing - facial/neck vasodilation (low doses can cause facial flush without systemic hypotension)
- Reflex tachycardia - baroreceptor-mediated compensatory response to hypotension
- Methemoglobinemia - at very high doses (more clinically relevant with sodium nitroprusside/amyl nitrite)
- Bezold-Jarisch reflex - paradoxical bradycardia and hypotension with sublingual GTN (vagally mediated)
- Nitrate tolerance - with continuous use (see below)
- Nitrate dependence - withdrawal angina in industrial workers exposed chronically
Nitrate Tolerance
- Develops with repeated high-dose/continuous exposure
- Mechanisms: depletion of sulfhydryl groups, free radical generation, neurohumoral activation (RAAS, sympathetics), plasma volume expansion, ALDH2 inactivation
- Prevention: Nitrate-free interval of 8-12 hours daily (usually at night for exertional angina)
- Eccentric twice-daily dosing for ISDN maintains efficacy
Precautions and Contraindications
- Sildenafil (and PDE5 inhibitors) - ABSOLUTE CONTRAINDICATION. Both increase cGMP; combined use causes severe, potentially fatal hypotension.
- Hypovolemia - preload-dependent states; GTN worsens hypotension
- Hypotension (SBP <90 mmHg) - contraindicated
- Right ventricular infarction - RV depends on preload; GTN can cause severe hypotension
- Hypertrophic obstructive cardiomyopathy (HOCM) - reduces preload, worsens outflow obstruction
- Increased intracranial pressure / head injury - meningeal vasodilation worsens ICP
- Closed-angle glaucoma - increases intraocular pressure
- Autonomic dysfunction (e.g., diabetic autonomic neuropathy) - compensatory sympathetic response impaired; severe hypotension/syncope possible
- Abrupt withdrawal - can precipitate rebound angina after chronic use
2. Coronary Steal Phenomenon
Definition
"Coronary steal" refers to the paradoxical diversion of blood flow away from ischemic myocardium toward well-perfused regions when a non-selective coronary arteriolar dilator is administered.
Pathophysiology
In a patient with partial coronary artery obstruction:
- In ischemic zones: arterioles are already maximally dilated due to local autoregulatory factors (adenosine, CO₂, reduced O₂). They cannot dilate further.
- In normal zones: arterioles are not maximally dilated and retain vasodilatory reserve.
When a potent arteriolar vasodilator (e.g., dipyridamole, adenosine, isoflurane) is given:
- Only the normal-zone vessels respond and dilate further
- Blood is preferentially redirected to the normal zones
- The ischemic zone loses flow → worsening ischemia
Normal zone: vasodilatory reserve present → DILATES → receives MORE blood
Ischemic zone: already maximally dilated → CANNOT dilate → receives LESS blood ("stolen")
Agents That Can Cause Coronary Steal
- Dipyridamole - major clinical example; inhibits adenosine uptake, causing widespread arteriolar dilation. Used in pharmacological stress testing precisely because it causes steal.
- Adenosine and regadenoson - both carry FDA black-box warnings for this effect
- Sodium nitroprusside - non-selective arteriolar/venous dilator; may cause steal in active MI
- Isoflurane - historic controversy in anesthetic practice (largely resolved; steal is possible but uncommon at clinical doses)
Clinical Significance
- Dipyridamole stress test (pharmacologic stress echo/nuclear scan) exploits coronary steal to provoke ischemia in CAD patients - deliberately induces steal to detect vulnerable myocardium.
- In unstable angina, inadvertent coronary steal from dipyridamole can precipitate MI.
- In coronary artery fistulas, the fistula creates a steal by diverting blood away from the myocardium, causing angina.
- Sodium nitroprusside is not recommended in acute MI patients because its non-selective vasodilation may induce steal.
Precautions
- Avoid dipyridamole in patients with unstable angina or severe CAD outside of controlled diagnostic settings
- Dipyridamole stress testing should be performed with resuscitation facilities available; aminophylline (adenosine receptor antagonist) is the antidote to reverse the effect
- Avoid drugs with non-selective arteriolar dilation in active MI
3. Nifedipine vs. Verapamil - Compare and Contrast
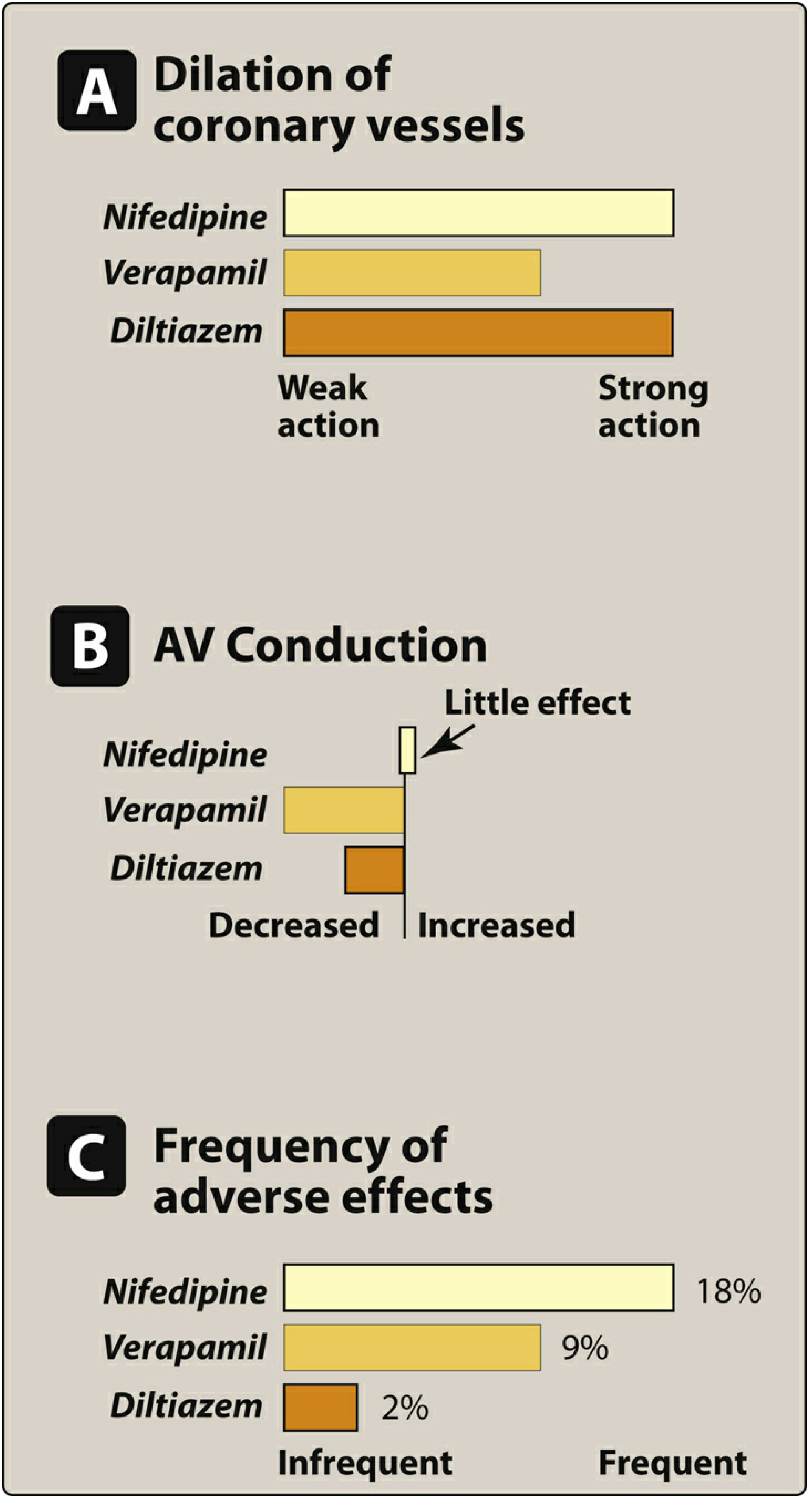
From Lippincott Illustrated Reviews: Pharmacology - Actions of CCBs
Basic MOA (Common)
All CCBs block voltage-gated L-type Ca²⁺ channels (bind to the α₁ subunit):
- Nifedipine binds to transmembrane segments of domains III and IV
- Verapamil binds to transmembrane segment 6 of domain IV (IVS6)
- Calcium influx blocked → smooth muscle relaxation (vasodilation) + decreased cardiac contractility/conduction
Comparison Table
| Feature | Nifedipine (Dihydropyridine) | Verapamil (Phenylalkylamine) |
|---|---|---|
| Drug class | Dihydropyridine (DHP) | Phenylalkylamine |
| Primary selectivity | Vascular smooth muscle >> cardiac | Cardiac > vascular |
| Vasodilation | Potent (especially peripheral arterioles) | Moderate |
| Heart rate | ↑ (reflex tachycardia due to hypotension) | ↓ (direct negative chronotropy on SA node) |
| AV conduction | Minimal effect | Strongly slows AV conduction (↑ PR interval) |
| Cardiac contractility | Minimal negative inotropy | Significant negative inotropy |
| SA node | Minimal effect | Slows automaticity |
| Antiarrhythmic use | NOT used (no AV node effect) | YES - SVT, AF rate control |
| Angina | YES - vasospastic and stable | YES - vasospastic, stable, and unstable |
| Hypertension | Preferred (potent arteriolar dilation) | Used but less preferred |
| Heart failure | Avoid (reflex tachycardia worsens demand; negative inotropy) | Avoid (negative inotropy) |
| Adverse effects | Headache, flushing, dizziness, reflex tachycardia, peripheral edema, gingival hyperplasia (18% adverse effect rate) | Constipation, bradycardia, AV block, lassitude, peripheral edema (9% adverse effect rate) |
| Constipation | No | Yes (common dose-dependent ADR) |
| Bioavailability | Low (first-pass); short-acting short t½ | ~20% oral bioavailability; t½ 4-7 hours |
| Interaction with digoxin | Minimal | Increases digoxin plasma levels (↑ toxicity risk) |
| Interaction with β-blockers | Can combine (heart rate control) | Dangerous combination - AV block and severe bradycardia |
| Use in AV block | Safer (no AV nodal effect) | CONTRAINDICATED |
| Use in WPW + AF | Not used | Contraindicated (enhances accessory pathway) |
| Use if VT misdiagnosed as SVT | Relatively safer | DANGEROUS - can cause hemodynamic collapse |
| Migraine prevention | Not used | Yes |
| Raynaud's phenomenon | YES (peripheral vasodilation) | Less effective |
| Tocolysis | Yes (relaxes uterine smooth muscle) | Not used for this |
| HOCM | Contraindicated | Can be used (reduces outflow obstruction via negative inotropy) |
Key Distinguishing Points (Exam Focused)
- Nifedipine = "vascular selective" → treats HTN and angina; causes reflex tachycardia; NO antiarrhythmic use
- Verapamil = "cardiac selective" → antiarrhythmic; constipation is hallmark ADR; DO NOT combine with β-blockers or use in AV block
- Verapamil is the prototype Phenylalkylamine; Nifedipine is the prototype Dihydropyridine
- Verapamil blocks both activated and inactivated T-type Ca²⁺ channels - frequency/use-dependent block
- Amlodipine (another DHP) is preferred over short-acting nifedipine in hypertension due to longer t½ (30-50 hours)
4. Nitrates (as a Class)
Members
| Drug | Route | Onset | Duration | Key Use |
|---|---|---|---|---|
| Nitroglycerin (GTN) | SL, transdermal, IV, oral SR | 1-3 min (SL) | 15-30 min (SL) | Acute angina, ACS |
| Isosorbide dinitrate (ISDN) | SL, oral | 3-6 min (SL) | 4-6 hours (oral) | Angina prophylaxis |
| Isosorbide-5-mononitrate (ISMN) | Oral only | ~30-60 min | 8-12 hours | Prophylaxis (no first-pass) |
| Amyl nitrite | Inhaled | 30 sec | 3-5 min | Cyanide poisoning (antidote), formerly acute angina |
ISMN has high oral bioavailability because it does not undergo significant first-pass hepatic metabolism.
MOA (Class)
All organic nitrates → release NO → activate sGC → ↑ cGMP → activate PKG → ↓ MLCK activity + ↓ intracellular Ca²⁺ → smooth muscle relaxation and vasodilation
The key signaling sequence: Nitrate → NO → sGC → cGMP → PKG → Vasodilation
Therapeutic Uses (Class)
- Stable angina - acute relief (SL GTN) and prophylaxis (ISDN, ISMN, transdermal GTN)
- Unstable angina - IV GTN reduces ischemia and preload
- Prinzmetal's (variant) angina - directly relieves coronary arterial spasm; drug of choice
- Acute MI - IV GTN in first 24-48 hours reduces preload, wall stress, infarct size
- Acute decompensated heart failure - venodilation rapidly reduces pulmonary congestion
- Hypertensive urgency/emergency - IV GTN or ISDN
- Esophageal spasm - smooth muscle relaxation
- Pulmonary hypertension - inhaled NO in neonates
- Anal fissures - topical GTN relaxes internal anal sphincter
Adverse Effects (Class)
| ADR | Mechanism |
|---|---|
| Throbbing headache | Meningeal arterial dilation (most common; decreases with continued use) |
| Postural hypotension | Venodilation → reduced venous return → ↓ BP |
| Reflex tachycardia | Baroreceptor response to hypotension |
| Flushing | Facial/neck vasodilation |
| Dizziness / syncope | Hypotension ("nitrate syncope") |
| Methemoglobinemia | High doses; amyl nitrite and nitroprusside are more relevant |
| Tolerance | Continuous high-dose exposure depletes SH groups, activates RAAS |
| Withdrawal angina | Rebound after chronic use; especially in industrial workers (Monday Disease) |
| Bezold-Jarisch reflex | Paradoxical bradycardia + hypotension with SL GTN |
Precautions (Class)
| Situation | Reason | Action |
|---|---|---|
| PDE5 inhibitors (sildenafil, tadalafil, vardenafil) | Both ↑ cGMP → severe synergistic hypotension | ABSOLUTE CONTRAINDICATION (at least 24-48h gap) |
| Right ventricular MI | RV preload dependent; venodilation → severe ↓ BP | Avoid nitrates |
| Hypovolemia | Worsens hypotension | Correct volume first |
| Severe aortic stenosis / HOCM | Fixed outflow obstruction; venodilation reduces CO severely | Avoid or use cautiously |
| Hypotension (SBP <90 mmHg) | Further BP drop dangerous | Contraindicated |
| ↑ ICP / head trauma | Cerebral vasodilation worsens ICP | Contraindicated |
| Autonomic dysfunction | Cannot compensate for BP drop | Use with extreme caution |
| Glaucoma (closed-angle) | May raise IOP | Avoid |
| Tolerance prevention | Continuous use → loss of efficacy | Maintain 8-12 hour nitrate-free interval |
| Abrupt withdrawal | Rebound angina / vasospasm | Taper gradually |
Nitrate-Free Interval Strategy
- Exertional angina: remove patch/omit night dose (patient sleeps without nitrate)
- Nocturnal / rest angina: omit daytime dose instead
- Always add another antianginal agent (β-blocker or CCB) to cover the nitrate-free period
Summary for Exams:
- Nitrates/GTN: NO donor → cGMP → vasodilation (mainly venous); key contraindication = PDE5 inhibitors + RV MI
- Coronary steal: maximum arteriolar dilation in normal zones diverts blood from ischemic zones; caused by dipyridamole, adenosine; used in stress testing; dangerous in unstable angina
- Nifedipine: vascular-selective DHP; reflex tachycardia; no AV node effect; gingival hyperplasia; 18% ADR rate
- Verapamil: cardiac-selective; antiarrhythmic; constipation; AV block risk; dangerous with β-blockers + digoxin; 9% ADR rate
This is a shared conversation. Sign in to Orris to start your own chat.