Write a short note on hip joint
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a concise note on the hip joint, drawn from Gray's Anatomy for Students and S Das: A Manual on Clinical Surgery.
The Hip Joint
Type and Articulation
The hip joint is a multiaxial ball-and-socket synovial joint formed between the spherical head of the femur and the cup-shaped acetabulum of the pelvic bone. It is designed primarily for stability and weight-bearing, with some sacrifice of mobility compared to the shoulder joint.
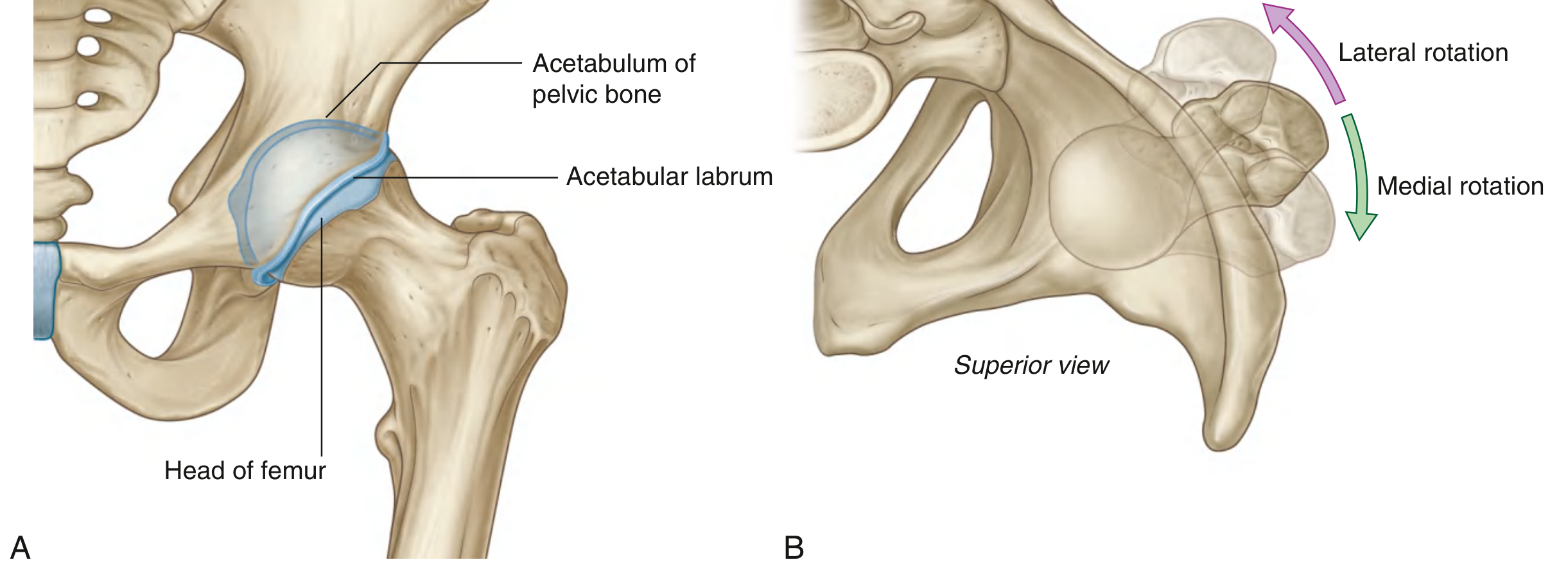
Articular Surfaces
- Head of femur - nearly spherical; covered by hyaline cartilage except at the fovea capitis (a small central pit).
- Lunate surface of the acetabulum - C-shaped, hyaline cartilage-covered, broadest superiorly where it bears the most weight.
- The acetabular fossa (central non-articular area) contains loose connective tissue and fat.
- The rim is deepened by the acetabular labrum - a fibrocartilaginous collar that increases socket depth and stability. Inferiorly, the labrum bridges the acetabular notch as the transverse acetabular ligament, converting the notch into a foramen.
Joint Capsule
The fibrous membrane (joint capsule) is strong and thick:
- Proximally attached to the margin of the acetabulum, transverse acetabular ligament, and adjacent obturator foramen margin.
- Distally attached to the intertrochanteric line anteriorly and just proximal to the intertrochanteric crest posteriorly.
The synovial membrane lines the fibrous capsule and forms a tubular sheath around the ligament of the head of the femur.
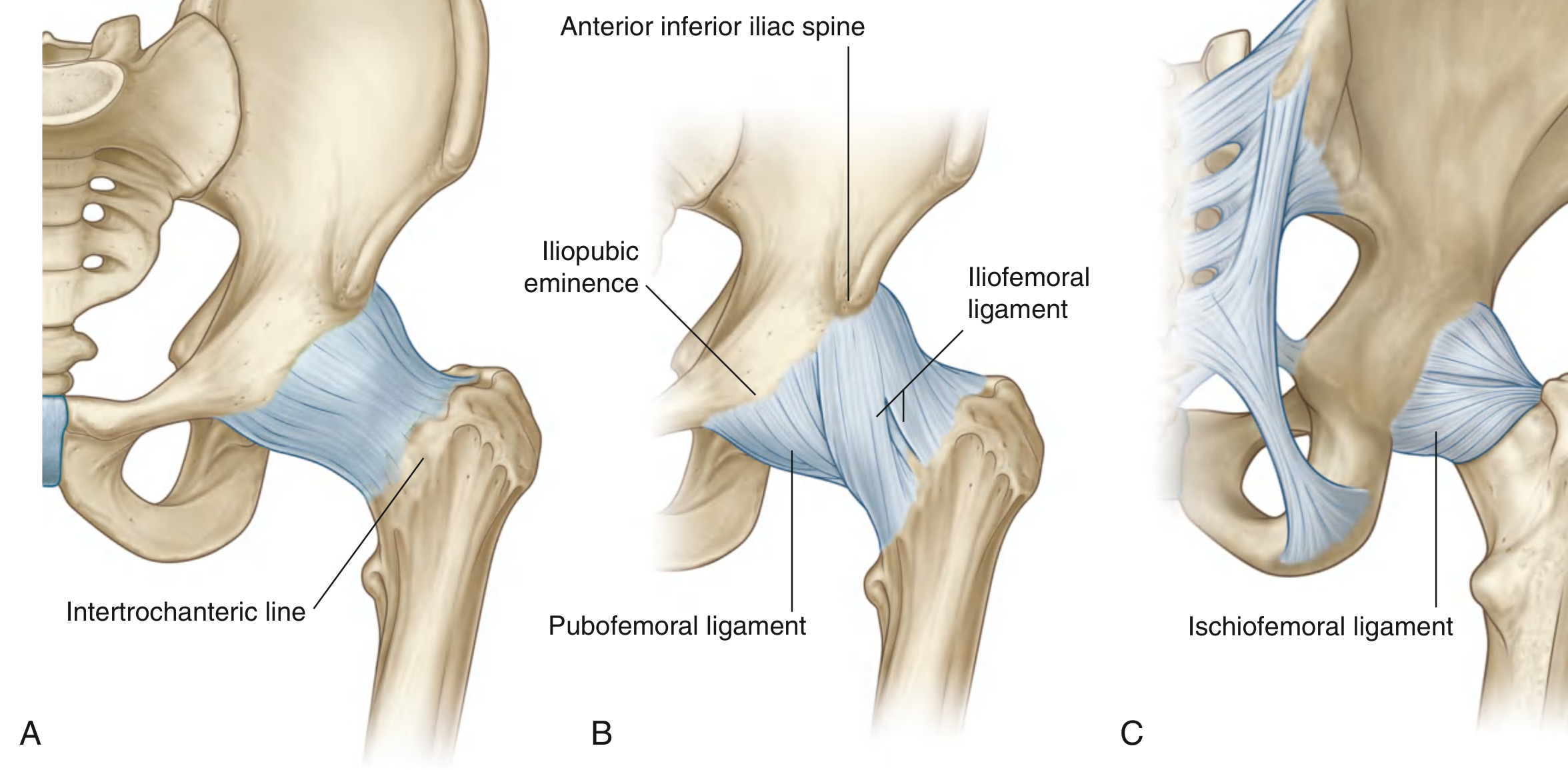
Ligaments
Three extracapsular ligaments spiral around the capsule and become taut in extension, stabilizing the standing posture with minimal muscle effort:
| Ligament | Location | Attachments |
|---|---|---|
| Iliofemoral (Y-ligament of Bigelow) | Anterior | AIIS to intertrochanteric line; strongest ligament in the body |
| Pubofemoral | Anteroinferior | Iliopubic eminence to fibrous capsule |
| Ischiofemoral | Posterior | Ischium (posterior to acetabulum) to greater trochanter |
One intracapsular ligament, the ligament of the head of the femur, runs from the fovea capitis to the acetabular fossa. It carries a small branch of the obturator artery that contributes to the blood supply of the femoral head.
Movements and Muscles
| Movement | Range | Primary Muscles |
|---|---|---|
| Flexion | 120-140° | Iliopsoas, rectus femoris, sartorius |
| Extension | ~20° | Gluteus maximus, hamstrings |
| Abduction | 50-80° | Gluteus medius and minimus |
| Adduction | ~30° | Adductors (longus, brevis, magnus), gracilis |
| Medial rotation | ~40° | Gluteus medius/minimus (anterior fibers), TFL |
| Lateral rotation | ~40° | Piriformis, obturator internus/externus, gemelli, quadratus femoris |
| Circumduction | - | Combination of above |
Blood Supply
The joint receives branches from:
- Medial and lateral circumflex femoral arteries (primary supply to femoral head via retinacular vessels)
- Obturator artery (via ligament of the head of the femur - minor contribution)
- Superior and inferior gluteal arteries
- First perforating branch of the deep femoral artery
Clinical note: Fracture of the femoral neck can disrupt the retinacular blood supply, leading to avascular necrosis of the femoral head.
Nerve Supply
The joint is innervated by articular branches from the femoral, obturator, and superior gluteal nerves, and the nerve to quadratus femoris (Hilton's law applies). This explains why hip joint pain frequently radiates to the knee (shared femoral and obturator nerve supply).
Clinical Relevance
- Osteoarthritis is the most common disorder, presenting with pain (often felt anteriorly or referred to the knee), stiffness, and limp. Pain worsening at night signals cartilage destruction.
- Trendelenburg's sign - positive when abductors are weak or the lever arm is lost (congenital dislocation, coxa vara, fracture neck of femur), causing the pelvis to drop on the contralateral side.
- Congenital hip dislocation presents from birth; Perthes' disease from 5-10 years; slipped upper femoral epiphysis from 10-15 years.
- The resting (loose-pack) position is slight flexion, abduction, and lateral rotation; the close-pack (most stable) position is full extension with medial rotation.
Sources: Gray's Anatomy for Students, pp. 661-663 | S Das: A Manual on Clinical Surgery, 13th Ed., pp. 239+ | THIEME Atlas of Anatomy - General Anatomy and Musculoskeletal System
This is a shared conversation. Sign in to Orris to start your own chat.