how prolia helps with osteoprosis
Reading File
Finding Sources
Searching PubMed
denosumab osteoporosis fracture prevention
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Here is a complete, textbook-grounded explanation of how Prolia (denosumab) works in osteoporosis:
Prolia (Denosumab) in Osteoporosis
What Is It?
Prolia is the brand name for denosumab, a fully human monoclonal antibody. It is given as a 60 mg subcutaneous injection every 6 months.
Mechanism of Action
Bone mass is controlled by a balance between osteoblasts (bone builders) and osteoclasts (bone destroyers). In osteoporosis, especially after menopause, this balance tips toward destruction.
The key signaling molecule driving osteoclast activity is RANKL (Receptor Activator of Nuclear Factor Kappa-B Ligand). Denosumab works by binding to and blocking RANKL, which:
- Prevents osteoclast formation, activation, and survival
- Dramatically reduces bone resorption (CTX-1, a marker of osteoclast activity, is suppressed by nearly 90% within weeks of each injection)
- Allows osteoblasts to keep building bone relatively unopposed
This is different from bisphosphonates (like alendronate), which embed in bone and poison osteoclasts. Denosumab blocks the signal before osteoclasts even become active. - Firestein & Kelley's Textbook of Rheumatology, p. 3067
What Does It Actually Do to Bone?
Unlike bisphosphonates, where bone mineral density (BMD) plateaus after 4-5 years, denosumab continues to increase BMD for as long as treatment continues. In the long-term extension of the pivotal FREEDOM trial:
-
BMD at the spine increased by 21.7% after 10 years
-
BMD at the hip increased by 9.2% after 10 years
-
Fracture rates remained low throughout
-
Harrison's Principles of Internal Medicine 22E, p. 3349-3350
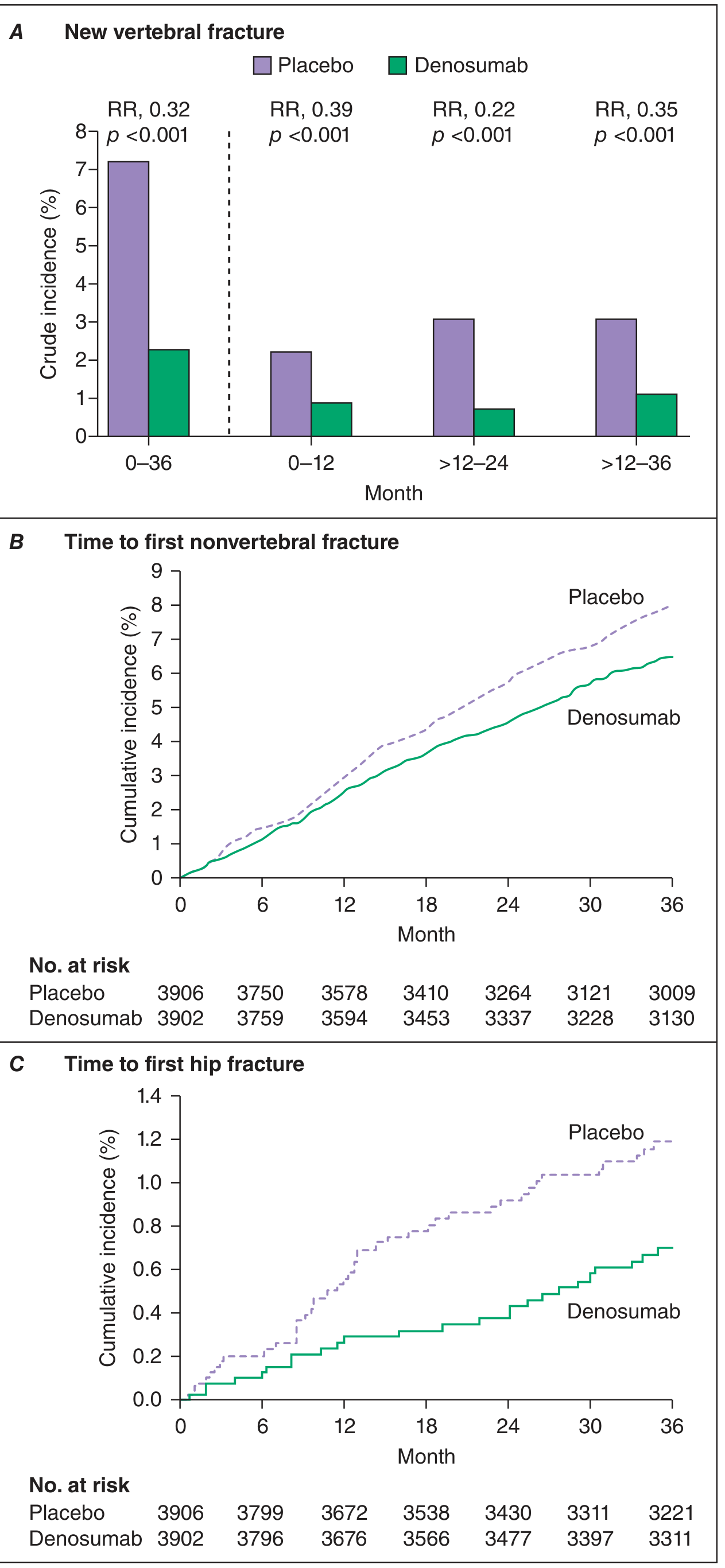
Fracture Reduction (The FREEDOM Trial Data)
In the landmark 3-year phase III trial in postmenopausal women with osteoporosis, denosumab 60 mg every 6 months reduced:
| Fracture Type | Relative Risk Reduction |
|---|---|
| Vertebral fractures | 68% |
| Hip fractures | 40% |
| Nonvertebral fractures | 20% |
Here is the actual trial data graph from Harrison's:
There is also evidence of a reduced risk of falls from an analysis of five placebo-controlled studies. - Harrison's, p. 3350
Who Is It Approved For?
The FDA approved denosumab in 2010 for:
- Postmenopausal women at high fracture risk (the primary indication)
- Men with osteoporosis at high fracture risk
- Glucocorticoid-induced osteoporosis
- Women with breast cancer on aromatase inhibitors
- Men with prostate cancer on androgen deprivation therapy
It is also considered a good alternative when patients are non-compliant with, or intolerant to, oral bisphosphonates. - Lippincott Illustrated Reviews: Pharmacology, p. 893
Advantages Over Bisphosphonates
- No daily pill to take - just one injection every 6 months
- Safe in renal impairment (unlike bisphosphonates, which are avoided in severe CKD)
- BMD keeps improving with continued use, rather than plateauing
- Can be used in patients who switched from bisphosphonates for additional BMD gains
Side Effects and Safety
| Side Effect | Details |
|---|---|
| Hypocalcemia | Most important - check serum calcium and vitamin D before starting. Severe in CKD patients (GFR <30 mL/min) |
| Skin reactions | Dermatitis, rash, eczema |
| Serious infections | Skin infections requiring hospitalization were slightly higher vs placebo |
| Osteonecrosis of the jaw (MRONJ) | ~5/10,000 patient-years, similar to bisphosphonates |
| Atypical femur fractures | ~1/10,000 patient-years, similar to bisphosphonates |
The Critical Discontinuation Problem
This is the most important clinical caveat with denosumab: unlike bisphosphonates, it is fully reversible.
When denosumab is stopped:
- Bone turnover rebounds rapidly (osteoclast precursors that accumulated in bone marrow during therapy all mature at once)
- BMD drops back toward baseline within months
- There is a specific risk of multiple vertebral fractures after stopping
How to stop safely: Transition to a bisphosphonate (oral for 12-24 months, or a single IV zoledronic acid infusion at the time of the missed dose) to prevent rebound bone loss. - Harrison's, p. 3350; Goldman-Cecil Medicine
Recent Evidence
Two recent meta-analyses (2024) support its use and safety profile:
- A 2024 meta-analysis (PMID 38733394) comparing denosumab vs bisphosphonates found a comparable overall safety profile in primary osteoporosis RCTs.
- A 2024 systematic review (PMID 39312040) confirmed denosumab superiority over bisphosphonates for BMD gains in bisphosphonate-naive patients.
Bottom line: Prolia is a highly effective, convenient anti-resorptive therapy for osteoporosis that blocks the RANKL signal driving bone destruction. It produces sustained, progressive BMD gains and significant fracture reduction across all major sites. Its main limitation is that it cannot simply be stopped - a follow-on bisphosphonate is always needed to prevent rebound bone loss when discontinuing.
compare with aclasta
Finding Sources
Finding Sources
Searching PubMed
denosumab zoledronic acid osteoporosis comparison
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
I now have comprehensive data from multiple textbooks. Here is the full comparison:
Prolia (Denosumab) vs. Aclasta (Zoledronic Acid) in Osteoporosis
At a Glance
| Feature | Prolia (Denosumab) | Aclasta (Zoledronic Acid) |
|---|---|---|
| Drug class | Monoclonal antibody (RANKL inhibitor) | Nitrogen-containing bisphosphonate |
| Route | Subcutaneous injection | IV infusion (30 min) |
| Frequency | Every 6 months | Once yearly (5 mg) |
| Mechanism | Blocks RANKL - prevents osteoclast formation | Inhibits farnesyl pyrophosphate synthase in osteoclasts - causes apoptosis |
| Reversibility | Fully reversible - effects disappear when stopped | Embeds in bone - effects persist for years after stopping |
| Drug holiday possible? | No - dangerous rebound if stopped | Yes - can pause after 3-5 years in low-risk patients |
| Renal impairment | Safe (not renally cleared) | Contraindicated if eGFR <35 mL/min |
Mechanism Comparison
Zoledronic acid (Aclasta) is taken up at sites of active bone remodeling and inhibits the enzyme farnesyl pyrophosphate synthase in the mevalonate pathway inside osteoclasts. This disrupts intracellular protein trafficking and leads to osteoclast apoptosis. Crucially, the drug binds avidly to hydroxyapatite in bone and stays there - even a single infusion has antiresorptive effects that last 2 years or more. - Harrison's Principles of Internal Medicine 22E
Denosumab (Prolia) never enters bone. It circulates and intercepts RANKL before it can bind its receptor (RANK) on osteoclast precursors. No RANKL signal = no osteoclast formation or activation. The CTX-1 resorption marker drops ~90% within weeks, but when the antibody clears (~6 months), the signal returns unless another dose is given. - Firestein & Kelley's Textbook of Rheumatology
Fracture Reduction - Side by Side
Both drugs have pivotal 3-year phase III trials (HORIZON-PFT for zoledronic acid; FREEDOM for denosumab), so the numbers are directly comparable:
| Fracture Type | Denosumab (FREEDOM) | Zoledronic Acid (HORIZON-PFT) |
|---|---|---|
| Vertebral | 68% reduction | 70% reduction |
| Hip | 40% reduction | 40% reduction |
| Nonvertebral | 20% reduction | 25% reduction |
| All-cause mortality | Not demonstrated | 28% reduction (post-hip fracture population, HORIZON-RFT) |
The fracture reduction efficacy is essentially equivalent for vertebral and hip fractures. Zoledronic acid has a modest edge on nonvertebral fractures and uniquely reduces all-cause mortality in the post-hip fracture setting. - Rheumatology 2-Volume Set (2022)
BMD Response Over Time
| Denosumab | Zoledronic Acid | |
|---|---|---|
| 3-year spine BMD gain | ~9% | 6.7% |
| Long-term | Keeps increasing - 21.7% at spine after 10 years | Plateaus after 4-5 years |
| After stopping | Rapid bone loss and rebound | BMD declines only ~1% after pausing for 3 years |
For patients who need long-term treatment, denosumab produces progressively greater BMD gains but with the trade-off of no safe stopping point.
Adverse Effects Compared
| Side Effect | Denosumab | Zoledronic Acid |
|---|---|---|
| Flu-like reaction | Not seen | Very common - 20-42% after first infusion (fever, myalgia, arthralgia, headache), peaks at day 1, resolves within 3 days; milder with repeat doses |
| Hypocalcemia | Yes (especially in CKD) | Yes - check vitamin D before infusion |
| Renal toxicity | None - safe in CKD | Yes - contraindicated if eGFR <35 mL/min; check creatinine before each dose |
| Atrial fibrillation | Not significantly elevated | Reported (rare) |
| Osteonecrosis of jaw (MRONJ) | ~5/10,000 patient-years | Similar (rare) |
| Atypical femur fracture | ~1/10,000 patient-years | Similar (rare) |
| Rebound fractures on stopping | High risk - ~10.3% incidence; median 5 contiguous vertebrae; occurs ~11 months after last dose | Not seen - safe drug holiday |
| Skin reactions | Dermatitis, rash, eczema | Not seen |
| Uveitis | Not reported | Rare |
Stopping Treatment - The Key Practical Difference
This is where the two drugs diverge most clinically:
Zoledronic acid: You can stop after 3-5 years (a "drug holiday") in lower-risk patients because the drug remains embedded in bone and continues to suppress resorption for years. BMD declines only ~1% over 3 years off treatment. Patients at the highest vertebral fracture risk should continue beyond 3 years. - Rheumatology 2-Volume Set
Denosumab: A drug holiday is not recommended. When stopped, osteoclast precursors that accumulated during treatment all mature simultaneously, causing:
- Rapid surge in bone resorption
- BMD returning to baseline within months
- Risk of multiple contiguous vertebral fractures (~10.3% incidence, ~11 months after last dose)
How to stop denosumab safely: Transition to a bisphosphonate - either a single IV zoledronic acid infusion at the time of the missed Prolia dose, or oral bisphosphonates for 12-24 months. The required duration is not firmly established and varies between patients. - Harrison's 22E
Who Gets Which Drug?
| Clinical Scenario | Preferred Choice |
|---|---|
| Renal impairment (eGFR <35) | Denosumab (not renally cleared) |
| Can't tolerate/absorb oral bisphosphonates | Either (both are non-oral) |
| Patient unlikely to adhere to 6-monthly injections | Zoledronic acid (once yearly) |
| Patient wants eventual drug holiday | Zoledronic acid |
| Previously on bisphosphonates, still losing BMD | Denosumab (shown to give further BMD gains on switch) |
| Post-hip fracture (mortality benefit needed) | Zoledronic acid (28% mortality reduction proven) |
| Breast cancer on aromatase inhibitors / Prostate cancer on ADT | Denosumab (approved for both) |
| Glucocorticoid-induced osteoporosis | Both are approved |
Recent Evidence
- A 2024 meta-analysis (PMID 38733394) comparing denosumab vs bisphosphonates in RCTs found comparable overall safety, though denosumab had somewhat fewer GI adverse events while zoledronic acid had more flu-like reactions.
- A 2022 meta-analysis of cohort studies (PMID 35715524) in older adults found zoledronic acid was associated with lower risks of serious infections compared to denosumab, reinforcing the clinical concern about immunosuppressive effects of RANKL blockade.
- A 2022 network meta-analysis (PMID 35058055) across osteoporosis treatments confirmed equivalent fracture reduction between the two agents at all time points studied.
Bottom line: Both drugs are highly effective and have near-identical fracture reduction. The choice comes down to patient profile - denosumab wins for renal impairment and long-term BMD gains; zoledronic acid wins when a drug holiday is planned, when mortality reduction post-hip fracture matters, and when the flu-like reaction risk is acceptable. The inability to simply stop denosumab is its single biggest clinical limitation.
This is a shared conversation. Sign in to Orris to start your own chat.