Gout
Reading File
Finding Sources
Searching PubMed
gout management treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Searching Images
gout tophi monosodium urate crystals joint pathology
Here is a comprehensive overview of Gout:
Gout
Definition & Epidemiology
Gout is a crystal-induced arthropathy caused by the deposition of monosodium urate (MSU) crystals in joints and periarticular tissues, resulting from sustained hyperuricemia. It affects approximately 4% of adults in the US — ~5% of males and ~3% of females — and is more prevalent in older adults.
Risk factors:
- Obesity, hypertension, diabetes
- Thiazide diuretics, cyclosporin
- Purine-rich diet: red meats, beer, legumes, shellfish, anchovies
- Chronic kidney disease
Pathophysiology
Hyperuricemia (plasma urate >6.8 mg/dL) is necessary but not sufficient for gout — only ~10% of hyperuricemic patients develop gout.
Uric acid is the end product of purine catabolism. It accumulates via:
| Mechanism | Examples |
|---|---|
| Reduced excretion (90% of primary gout) | Unknown basis; CKD |
| Overproduction | HGPRT deficiency (Lesch-Nyhan syndrome), tumor lysis syndrome |
Inflammatory cascade:
- MSU crystals precipitate in supersaturated joint fluid
- Synovial macrophages phagocytose crystals → activate the inflammasome → caspase-1 → active IL-1β
- IL-1β recruits neutrophils → cytokines, free radicals, proteases, lysosomal enzyme release
- Acute arthritis (self-limiting over days–weeks)
- Repeated attacks → tophi (aggregates of urate crystals + inflammatory tissue) → cartilage destruction
Clinical Stages
| Stage | Features |
|---|---|
| Asymptomatic hyperuricemia | Elevated urate, no symptoms; may persist 20–30 years |
| Acute gout flare | Sudden severe monoarthritis; peaks in 1–2 days; resolves in ~1 week |
| Intercritical gout | Symptom-free intervals between attacks |
| Chronic tophaceous gout | Persistent tophi, polyarticular involvement, bony erosions |
Most common joint: First metatarsophalangeal (MTP) joint — podagra. Knee, ankle, tarsal joints, and hands also affected. Up to 20% have polyarticular involvement. Systemic symptoms (fever) can mimic septic arthritis.
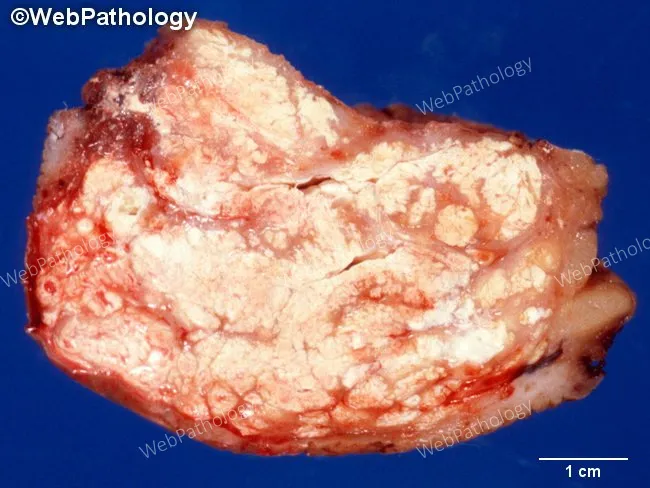
Tophi are gritty, chalk-white nodules of MSU crystals found in subcutaneous tissue, bursae, or joint spaces — generally painless until they erode bone.

Diagnosis
- Arthrocentesis (gold standard): Synovial fluid shows negatively birefringent needle-shaped MSU crystals under polarizing microscopy.
- Serum uric acid: Unreliable — attacks can occur with normal uric acid; many hyperuricemic patients are asymptomatic.
- WBC: May be elevated (non-specific).
- Renal function: Important — gout is associated with renal insufficiency and many treatments are nephrotoxic.
- Imaging:
- Plain X-ray (acute): soft-tissue swelling only; (chronic): asymmetric, sclerotic "overhanging edge" erosions outside the joint capsule.
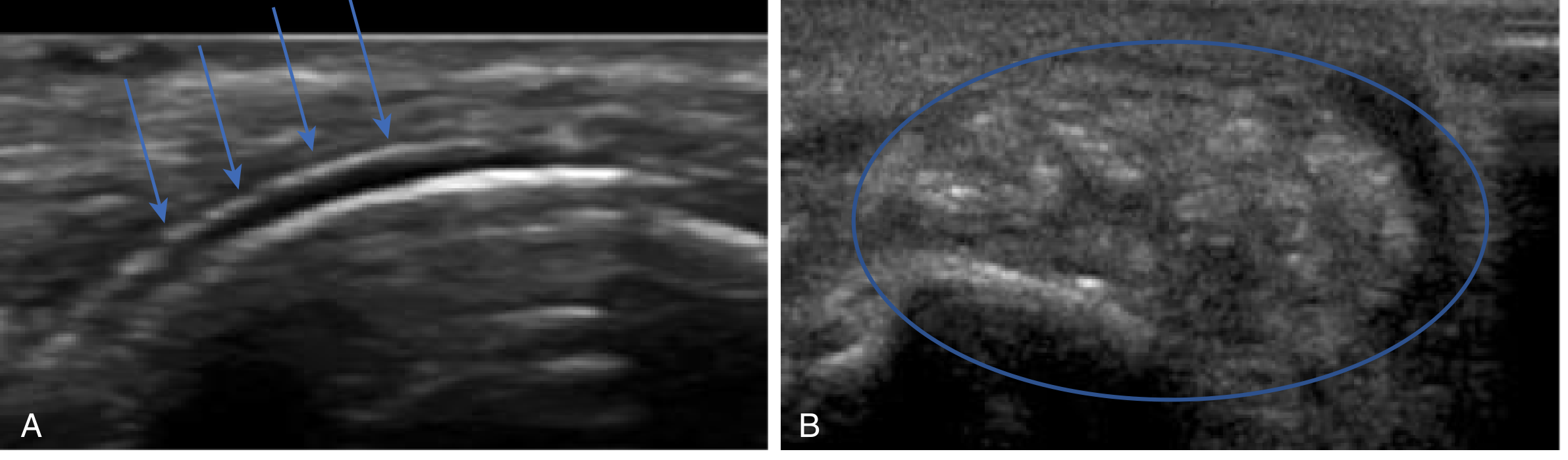
- Ultrasound: "Double contour sign" (urate coating cartilage); tophi appear as a "lump of sugar."
- Dual-energy CT (DECT): highly specific for urate deposits.
Management
Acute Flare
All three options (NSAIDs, colchicine, corticosteroids) are effective; choose based on comorbidities:
| Drug | Notes |
|---|---|
| NSAIDs (indomethacin, naproxen, ibuprofen) | First-line; start promptly; relief in ~24h; avoid in peptic ulcer, GI bleeding, renal insufficiency |
| Colchicine | Inhibits microtubule formation → blocks crystal-driven inflammation; contraindicated in renal/hepatic insufficiency; narrow therapeutic window; GI side effects common |
| Corticosteroids (oral or intra-articular) | Prednisone 40 mg/day × 5–7 days; intra-articular most effective for single joint; avoid if septic arthritis cannot be excluded |
- Do not start urate-lowering therapy during an acute flare, but continue existing therapy if already prescribed.
- Non-pharmacologic: ice, elevation, oral hydration, rest of inflamed joint.
Long-Term Urate-Lowering Therapy (ULT)
Target: serum urate <6 mg/dL (symptomatic patients).
| Drug | Mechanism | Key Points |
|---|---|---|
| Allopurinol | Xanthine oxidase inhibitor (purine analog) | Start 100–200 mg/day; titrate slowly (q4 weeks); dose-adjust for eGFR; risk of severe allopurinol hypersensitivity syndrome (DRESS) — higher in HLA-B*5801 carriers |
| Febuxostat | Xanthine oxidase inhibitor (non-purine analog) | 40–80 mg/day; no renal dose adjustment; higher CV mortality vs. allopurinol in high-CV-risk patients (CARES trial); use for allopurinol-intolerant patients |
| Probenecid | Uricosuric (increases renal urate excretion) | Avoid in underexcretors with renal impairment or urolithiasis |
| Pegloticase | Recombinant pegylated uricase; converts urate → allantoin | FDA-approved for refractory gout (2010); risk of infusion reactions and antibody-mediated loss of efficacy |
Note: Allopurinol and febuxostat both inhibit azathioprine metabolism — if co-prescribed, reduce azathioprine dose by ~25% and monitor CBC closely (or switch to mycophenolate, which doesn't interact).
Prophylaxis During ULT Initiation
Starting ULT can trigger acute flares by mobilizing urate deposits. Cover with low-dose colchicine (0.5–0.6 mg/day) or low-dose NSAIDs for 3–6 months.
Secondary Causes to Consider
- Lesch-Nyhan syndrome: Complete HGPRT deficiency → severe hyperuricemia + neurologic features (self-mutilation, choreoathetosis, intellectual disability)
- Tumor lysis syndrome: Rapid cell lysis from chemotherapy → urate overproduction
- Medications: Thiazide diuretics, loop diuretics, cyclosporin, low-dose aspirin
- CKD: Impaired urate excretion
Gout vs. Pseudogout (CPPD)
| Feature | Gout | Pseudogout (CPPD) |
|---|---|---|
| Crystal type | Monosodium urate | Calcium pyrophosphate |
| Crystal appearance | Needle-shaped, negatively birefringent | Rhomboid, positively birefringent |
| Most common joint | First MTP (podagra) | Knee |
| X-ray finding | Erosions, tophi | Chondrocalcinosis |
| Associations | Hyperuricemia, diet, CKD | Hemochromatosis, hypothyroidism, hyperparathyroidism |
Sources: Robbins & Kumar Basic Pathology; Rosen's Emergency Medicine; Comprehensive Clinical Nephrology, 7th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.