Cardiac glycosides, mechanism of action, uses, adverse effect, drug interactions.
Reading File
Finding Sources
Finding Sources
Searching PubMed
"cardiac glycosides" OR "digoxin" AND "heart failure"
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Reading File
I now have all the content needed for a comprehensive answer. Let me compile the full response.
Cardiac Glycosides
Overview
Cardiac glycosides (CGs) are a class of compounds derived from the foxglove plant Digitalis purpurea (and D. lanata). The prototype in clinical use is digoxin; others include digitoxin, β-acetyl digoxin, and methyldigoxin. They have been used for over 200 years - William Withering first systematically described their effects on "dropsy" (heart failure) in 1775.
Mechanism of Action
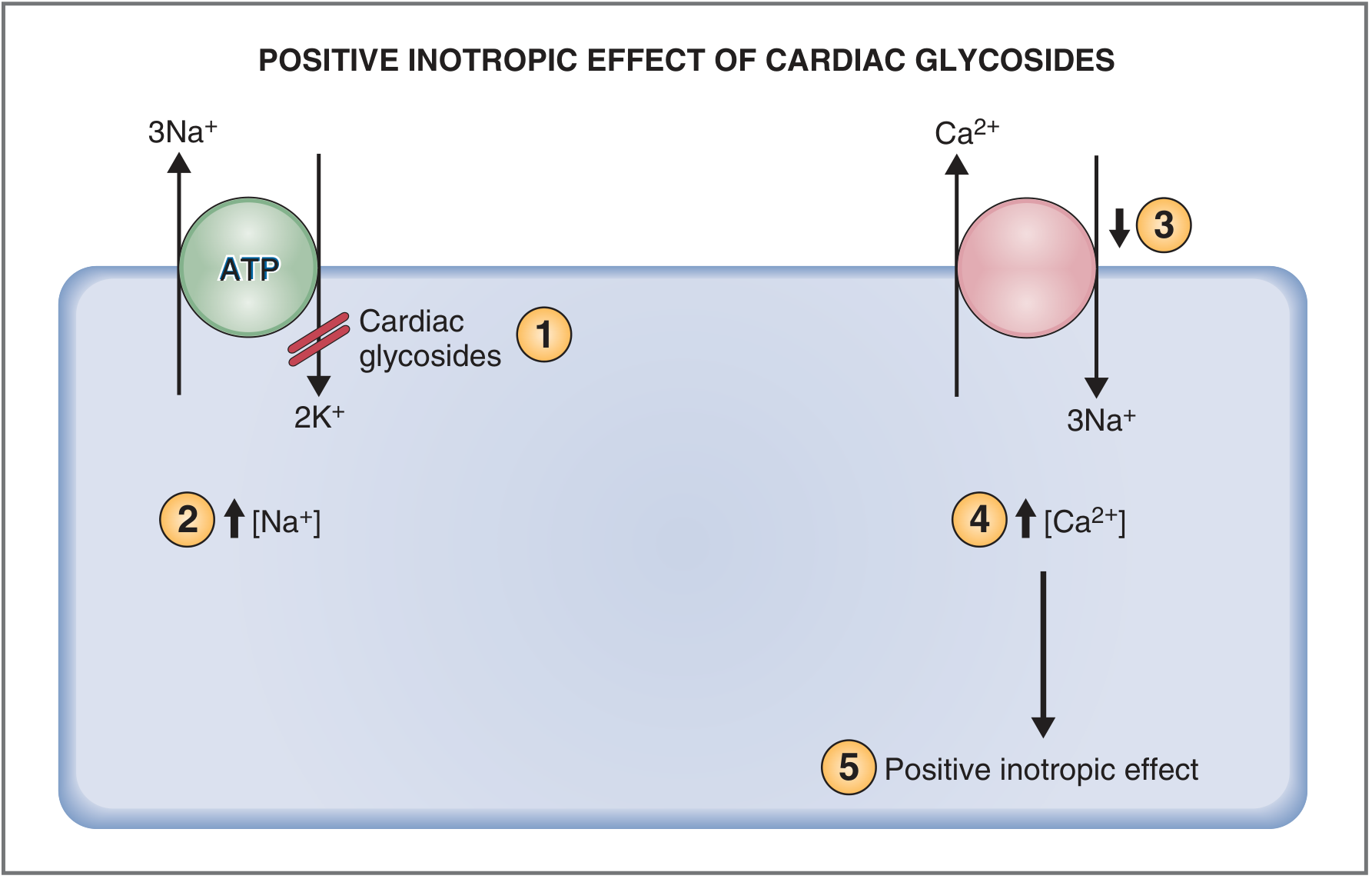
1. Na+/K+-ATPase Inhibition (Core Mechanism)
CGs bind to a specific high-affinity site on the extracytoplasmic face of the alpha subunit of the Na+/K+-ATPase pump (the "sodium pump"), inhibiting it. This inhibition is reversible and entropically driven. The drug preferentially binds to the E2P conformation (after phosphorylation of a beta-aspartate on the cytoplasmic face). Notably, elevated extracellular K+ promotes dephosphorylation, reducing CG binding - this is why raising K+ can reverse some toxicity manifestations.
2. Rise in Intracellular Na+
With the Na+/K+-ATPase inhibited, less Na+ is pumped out of the myocyte, so intracellular [Na+] rises.
3. Ca2+-Na+ Exchanger (NCX) Slows
The NCX normally extrudes Ca2+ from the cell by using the inward Na+ gradient as energy. With intracellular [Na+] elevated, the Na+ gradient decreases, and less Ca2+ is pumped out. Ca2+ therefore accumulates inside the cell.
4. Increased Intracellular Ca2+ --> Positive Inotropy
Higher intracellular [Ca2+] during systole increases the velocity and extent of sarcomere shortening, shifting the Frank-Starling curve upward and leftward - a positive inotropic effect that is sustained without tolerance or desensitization.
5. Autonomic (Neurohumoral) Effects
At low plasma concentrations, CGs stimulate vagal efferents and sensitize baroreceptor reflexes, resulting in:
- Increased parasympathetic tone
- Decreased sympathetic tone
- Reduced heart rate and peripheral vascular resistance
This sympatholytic effect may actually be more therapeutically relevant than direct inotropy at the low doses used in modern heart failure management. Increased cardiac output also improves renal perfusion, lowering renin production and increasing diuresis, further reducing preload.
6. Electrophysiological Effects
At therapeutic concentrations, CGs:
- Prolong the effective refractory period of the AV node (increased vagal tone)
- Decrease AV nodal conduction velocity
- Shorten action potentials (by accelerating L-type Ca2+ channel inactivation due to higher [Ca2+])
At toxic concentrations:
- SR Ca2+ overload triggers spontaneous Ca2+ release waves, which via the NCX cause delayed afterdepolarizations and triggered activity
- Partial inactivation of Na+ channels impairs impulse propagation
- Increased automaticity + depressed conduction = substrate for re-entry arrhythmias
Uses
| Indication | Details |
|---|---|
| Heart failure with reduced EF (HFrEF) | Used as third-line (or not at all per some guidelines) when symptoms persist despite ACE-I/ARB, beta-blockers, diuretics. Reduces symptoms and hospitalizations but does not improve overall mortality. |
| Atrial fibrillation (AF) - rate control | Slows ventricular rate via AV nodal blockade. Less effective during exercise (sympathetically mediated conduction). |
| Atrial flutter | Rate control. |
| Paroxysmal SVT | Historically used; less common now. |
The landmark DIG trial showed digoxin reduced HF hospitalizations but had neutral effect on mortality. Serum concentrations of 0.5-0.8 ng/mL are associated with benefit; concentrations >1.0-1.2 ng/mL are associated with increased mortality.
Adverse Effects
CGs have a narrow therapeutic index. Toxicity may develop at concentrations >2 ng/mL in adults (children tolerate higher concentrations). Factors increasing sensitivity to toxicity: hypokalemia, hypomagnesemia, hypercalcemia, hypothyroidism, renal impairment.
Cardiac Toxicity (most dangerous)
- Bradyarrhythmias: Sinus bradycardia, sinoatrial block, AV block (1st, 2nd, or 3rd degree)
- Tachyarrhythmias: Multiform PVCs, ventricular bigeminy (classic sign), ventricular tachycardia, ventricular fibrillation
- Paroxysmal atrial tachycardia with AV block - a virtually pathognomonic finding
- Non-paroxysmal junctional tachycardia
GI Toxicity
- Anorexia, nausea, vomiting (mediated via chemosensors in the area postrema - earliest symptoms)
- Diarrhea
- Rarely: spastic contraction of the mesenteric artery causing intestinal necrosis
Neurological/CNS
- Headache, fatigue, sleeplessness (early symptoms)
- Confusion, delirium (especially in elderly)
Visual Disturbances (~10% of toxicity cases)
- Altered color perception - classic xanthopsia (yellow-green halo vision)
- Coronas/halos around objects
- Blurred vision, scotomas
- (Historically, van Gogh's famous yellow-tinted late paintings have been attributed to possible digitalis treatment by his physician.)
Other
- Gynecomastia (with chronic use - due to steroidal structure)
Pharmacokinetics (Digoxin)
- Oral bioavailability: 60-80% (variable depending on formulation)
- Protein binding: ~25%
- Volume of distribution: Large (4-7 L/kg) - concentrated in cardiac tissue 15-30x plasma levels
- Elimination: Primarily renal (glomerular filtration + tubular secretion via P-glycoprotein); excretes ~1/3 of body stores/day
- Half-life: 36-48 hours (normal renal function); longer in renal failure
- Specimen timing: Must be drawn 8+ hours after dose to avoid falsely elevated "peak" levels
- Therapeutic range: 0.5-1.0 ng/mL (optimal); >2 ng/mL = toxicity
- Dosing: Maintenance 0.0625-0.25 mg/day orally; reduced in elderly, renal impairment, low lean body mass
Drug Interactions
Digoxin has numerous clinically significant drug interactions, primarily affecting serum levels via P-glycoprotein modulation or altered renal clearance:
Drugs that INCREASE Digoxin Levels (toxicity risk)
| Drug | Mechanism |
|---|---|
| Amiodarone | Reduced renal clearance (inhibits P-gp) - dose digoxin by 50% |
| Verapamil | Reduced renal clearance; additive AV block |
| Diltiazem | Reduced renal clearance; additive AV block |
| Nifedipine | Reduced renal clearance |
| Quinidine | Displaces protein binding + reduces renal clearance - classic interaction, doubles level |
| Propafenone | Reduced renal clearance |
| Spironolactone, amiloride, triamterene | Reduced renal clearance |
| Carvedilol | Increases oral bioavailability |
| Macrolide antibiotics (clarithromycin, erythromycin) | Altered gut flora, reduces P-gp-mediated intestinal efflux |
| Tetracycline | Altered gut flora (eliminates bacteria that inactivate digoxin in gut) |
| Indomethacin, itraconazole, cyclosporine, alprazolam | Reduced renal clearance |
| Captopril | Possible reduced renal clearance |
Drugs that DECREASE Digoxin Levels (loss of efficacy)
| Drug | Mechanism |
|---|---|
| Rifampin | Induces intestinal P-glycoprotein, reducing absorption |
| Cholestyramine | Binds digoxin in gut, reduces absorption |
| Antacids, sucralfate | Reduced gut absorption |
| Salbutamol (albuterol) | Unknown mechanism |
| St. John's Wort | Induces P-gp (reduces absorption) |
Pharmacodynamic Interactions (no change in levels, but altered toxicity risk)
| Drug | Effect |
|---|---|
| Loop diuretics, thiazides | Cause hypokalemia/hypomagnesemia - sensitizes myocardium to glycoside toxicity |
| Succinylcholine | Transient hyperkalemia can cause arrhythmias |
| Beta-blockers | Additive bradycardia/AV block |
| Calcium IV | Hypercalcemia dramatically increases glycoside sensitivity |
| Sympathomimetics | Increase risk of ventricular arrhythmias |
Management of Toxicity
- Stop the drug - often sufficient for mild toxicity
- Bradyarrhythmias / AV block: Atropine 0.5-1 mg IV; temporary pacemaker if unresponsive
- Ventricular arrhythmias + hypokalemia: IV K+ infusion (40-60 mmol/day); monitor for worsening AV block with high K+
- Severe/life-threatening toxicity: Digoxin-specific Fab fragments (DigiFab, Digibind) - ovine anti-digoxin antibody fragments that rapidly neutralize free digoxin; dosed based on estimated total body load
- Lidocaine or phenytoin for ventricular arrhythmias
- Avoid cardioversion in digoxin toxicity (risk of fatal VF) unless absolutely necessary
Key Clinical Pearls
- Hypokalemia is the most important precipitating factor for digoxin toxicity - always check electrolytes
- Dose digoxin for lean body weight, not total body weight
- Renal function must be monitored and dose adjusted accordingly
- The classic ECG "scooped" ST depression (Salvador Dali mustache sign) is a digitalis effect, not toxicity - it does not indicate toxic levels
- Target serum level in modern practice: 0.5-0.8 ng/mL; avoid >1.0 ng/mL
Recent Evidence Note: A 2025 expert consensus systematic review (PMID: 39265879) on digoxin toxicity diagnosis and management is available, which may refine current management thresholds.
Sources: Goodman & Gilman's Pharmacological Basis of Therapeutics; Braunwald's Heart Disease, 2 Vol Set; Costanzo Physiology, 7th Ed.; Tietz Textbook of Laboratory Medicine, 7th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.