Causes of hypotension
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Loading Image
Excellent - I now have comprehensive textbook content. Here is the complete, well-organized answer:
Causes of Hypotension
Hypotension is traditionally classified into four mechanistic categories. In patients presenting with shock, distributive causes account for ~65% of cases, hypovolemic and cardiogenic ~15% each, and obstructive <5%.
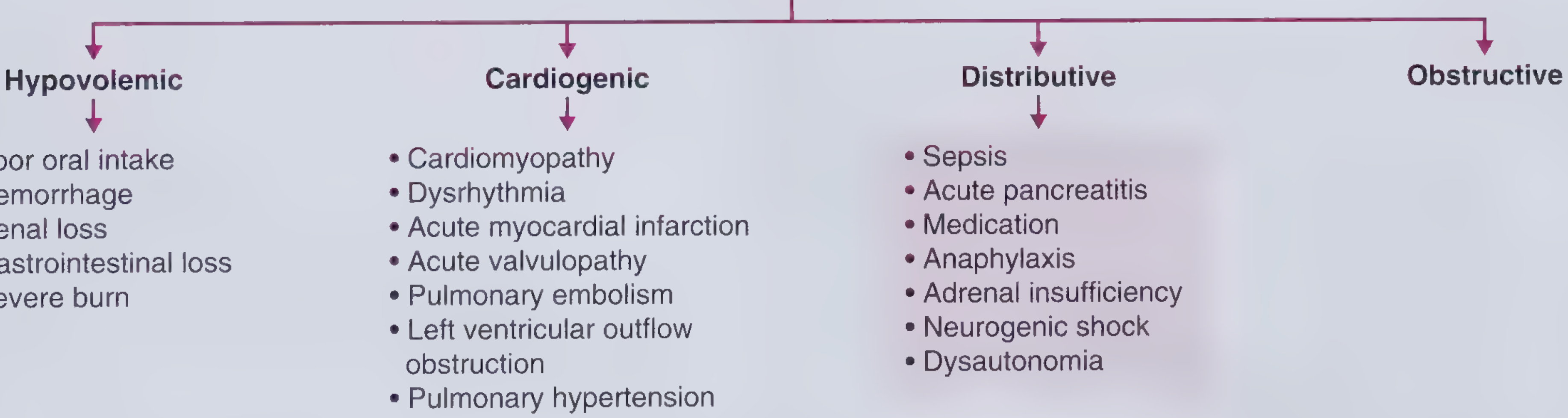
1. Hypovolemic Hypotension
Mechanism: Decreased intravascular volume → reduced cardiac preload → reduced cardiac output. Characteristically presents with low JVP, low CO, high SVR, and cool extremities (compensatory vasoconstriction).
| Cause | Examples |
|---|---|
| Poor oral intake | Anorexia, delirium, obstruction, socioeconomic factors |
| Hemorrhage | Trauma; occult bleeding in retroperitoneum, pelvis, thigh |
| Renal salt wasting | Diuretic use, primary adrenal insufficiency (urine Na >20-30 mEq/L) |
| GI losses | Vomiting, diarrhea |
| Severe burns | Massive fluid loss through skin |
2. Cardiogenic Hypotension
Mechanism: Pump failure - the heart cannot generate adequate cardiac output despite normal or elevated filling pressures.
- Cardiomyopathy (dilated, hypertrophic, restrictive)
- Dysrhythmia (tachyarrhythmia or bradyarrhythmia)
- Acute Myocardial Infarction - especially inferior STEMI (RV involvement)
- Acute Valvulopathy - e.g., acute aortic regurgitation (wide pulse pressure, diastolic murmur)
- Left Ventricular Outflow Tract Obstruction - e.g., severe aortic stenosis, HOCM
- Pulmonary Hypertension - right heart failure, loud P2, RV heave
- Pulmonary Embolism - acute right heart strain (also listed under obstructive)
3. Distributive Hypotension
Mechanism: Pathological vasodilation causing a decrease in systemic vascular resistance (SVR). Presents with warm extremities (vasodilation), high CO early, and low SVR - in contrast to the other categories.
- Sepsis - by far the most common cause of shock overall (~65% of all shock)
- Anaphylaxis - accompanied by bronchoconstriction and urticaria
- Acute pancreatitis - cytokine-mediated vasodilation
- Medications - antihypertensives (especially in patients with restarted home meds after poor adherence), vasodilators
- Primary adrenal insufficiency (Addison's disease) - hyperpigmentation + hyponatremia + hyperkalemia
- Neurogenic shock - sudden loss of autonomic tone after spinal cord injury
- Dysautonomia - e.g., Parkinson's disease, orthostatic hypotension with no compensatory HR rise
4. Obstructive Hypotension
Mechanism: Physical obstruction to blood flow prevents adequate cardiac output despite normal pump function and volume.
| Cause | Key Findings |
|---|---|
| Cardiac tamponade | Beck's triad: tachycardia + hypotension + elevated JVP + muffled heart sounds; pulsus paradoxus >10 mmHg; enlarged cardiac silhouette on CXR |
| Tension pneumothorax | Tracheal deviation on CXR; absent breath sounds; requires emergency needle thoracostomy |
| Constrictive pericarditis | Kussmaul's sign + pericardial knock (high-pitched, closer to S2 than S3) |
| Massive pulmonary embolism | Acute RV strain, elevated JVP |
Additional/Special Causes
- Orthostatic hypotension - defined as a drop of ≥20 mmHg systolic or ≥10 mmHg diastolic within 3 minutes of standing. Causes include dehydration, autonomic neuropathy (diabetes, Parkinson's), prolonged bed rest, age-related changes.
- Toxicologic - drugs causing bradycardia and hypotension include beta-blockers, calcium channel blockers, digoxin, opioids, alpha-2 agonists.
- Endocrine - hypothyroidism (myxedema coma), pheochromocytoma crisis.
- Intradialytic hypotension - seen in patients on hemodialysis due to rapid volume removal.
Source: Frameworks for Internal Medicine (Wolters Kluwer); Miller's Anesthesia 10e; Tintinalli's Emergency Medicine; Rosen's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.