Features suggestive of ovulation after induction
Features Suggestive of Ovulation After Induction
1. Urinary LH Surge (LH Kit Testing)
- The LH surge is detectable in urine approximately 2 hours after the serum LH peak.
- Commercially available ELISA-based urinary LH kits use a threshold of 35–50 mIU/mL.
- When the LH surge is detected, ovulation may occur within the next 48 hours.
- Positive predictive value: 92%; negative predictive value: 95%.
- After clomiphene or letrozole (days 5–9), the LH surge typically occurs on cycle days 16–17.
- LH kit testing should begin when the largest ultrasound-measured follicle reaches 14 mm in diameter.
- Testing twice daily may improve detection (the surge may last <12 hours).
2. Midluteal Serum Progesterone
- Should be measured 7 days after the LH surge (or on days 21–23 of a 28-day cycle) to coincide with peak progesterone secretion.
- A level >3 ng/mL (>10 nmol/L) typically confirms ovulation.
- Ovulatory levels are often considerably higher than 3 ng/mL.
- Note: Low midluteal progesterone alone does not necessarily confirm anovulation, due to pulsatile secretion.
3. Ultrasound (US) Monitoring — Most Reliable
- Ovulation is characterized by:
- Decrease in follicle size (follicle collapse)
- Appearance of fluid in the cul-de-sac (peritoneal fluid post-rupture)
- Following ovulation induction, follicles typically reach a preovulatory diameter of 19–25 mm (may be as large as 30 mm), compared with 17–19 mm in spontaneous cycles.
- If a dominant follicle is present without a spontaneous LH surge, hCG can be administered to trigger final follicular maturation — ovulation occurs approximately 40 hours later.
- If large cysts are seen at baseline, the current treatment cycle should be withheld.
- A luteinized unruptured follicle (LUF) can occur in ~10% of normally fertile women and ~25% in unexplained infertility — progesterone rises normally without visible follicle rupture on US.
4. Combined LH + Ultrasound Monitoring
- Start LH kit testing when the largest US follicle reaches 14 mm.
- Confirm ovulation by midluteal progesterone 7 days after the LH surge.
- This combined approach is the most comprehensive monitoring strategy.
Summary Table
| Feature | Threshold / Finding | Timing |
|---|---|---|
| Urinary LH surge | ≥35–50 mIU/mL | Detectable ~2 hrs after serum surge |
| Ovulation post-LH surge | — | Within 48 hours of surge |
| Midluteal progesterone | >3 ng/mL | Day 21–23 (or LH surge +7) |
| Follicle size (US) | 19–25 mm (up to 30 mm) | Preovulatory |
| Follicle collapse + cul-de-sac fluid (US) | Visible change | Confirms rupture |
| hCG trigger → ovulation | — | ~40 hrs post-injection |
Clinical features of ovulation
Clinical Features of Ovulation
1. Mittelschmerz (Mid-cycle Pain)
- A variable amount of lower abdominal pain occurring at mid-cycle, around the time of ovulation.
- Caused by:
- Slight bleeding into the peritoneal cavity following follicle rupture
- Enlargement of the oocyte just before ovulation
- The pain is typically sudden and constant, felt in one iliac fossa.
- Considered a secondary indicator of ovulation — useful but not definitive.
- — The Developing Human: Clinically Oriented Embryology
2. Cervical Mucus Changes
- Under estrogen influence at mid-cycle, cervical mucus undergoes characteristic changes:
- Becomes thin, watery, copious, clear, and alkaline — favoring sperm penetration.
- Spinnbarkeit increases markedly: a drop can be stretched into a thin thread 8–12 cm or more in length.
- When spread on a slide and dried, produces an arborizing fern-like pattern (ferning/arborization).
- Channels form in the mucus, creating openings in the cervix through which sperm are propelled.
- After ovulation, under progesterone influence, mucus becomes thick, tenacious, cellular, and non-elastic, and no longer ferning.
- — Ganong's Review of Medical Physiology; Costanzo Physiology
3. Basal Body Temperature (BBT) Rise
- A rise in BBT of at least 0.1°C (about 0.2–0.5°F) indicates ovulation has occurred.
- The rise is due to the thermogenic effect of progesterone secreted by the newly formed corpus luteum.
- The temperature shift is sustained through the luteal phase and drops with menstruation.
- Considered a primary indicator of ovulation.
- — The Developing Human; Swanson's Family Medicine Review
4. LH Surge (Biochemical-Clinical Correlate)
- A mid-cycle LH surge triggers ovulation within ~36–48 hours.
- Detectable in urine ~2 hours after the serum peak using commercially available kits.
- Clear, stretchy cervical mucus and mild pelvic discomfort often coincide with this surge.
5. Vaginal Cytology Changes
- Under estrogen influence (follicular phase / around ovulation): vaginal epithelium becomes cornified; cornified cells are identifiable on vaginal smear.
- After ovulation, under progesterone: thick mucus is secreted, epithelium proliferates, and becomes infiltrated with leukocytes.
- — Ganong's Review of Medical Physiology
6. Breast Changes
- Many women experience breast swelling, tenderness, and pain premenstrually, reflecting estrogen (ductal proliferation) and progesterone (lobular/alveolar growth) effects that peak around ovulation and the luteal phase.
- — Ganong's Review of Medical Physiology
7. Ultrasound Features (Objective Confirmation)
- Pre-ovulatory follicle reaches 17–19 mm in spontaneous cycles (19–25 mm in induced cycles).
- Ovulation is confirmed by:
- Sudden decrease in follicle size (collapse)
- Free fluid in the pouch of Douglas (cul-de-sac)
Summary
| Feature | Timing | Nature |
|---|---|---|
| Mittelschmerz | Mid-cycle | Secondary indicator |
| Cervical mucus — thin, clear, spinnbarkeit, ferning | Periovulatory | Primary indicator |
| BBT rise (≥0.1°C) | After ovulation | Primary indicator |
| LH surge | ~36–48 hrs pre-ovulation | Biochemical correlate |
| Vaginal cornification | Follicular/periovulatory | Supporting sign |
| Follicle collapse + cul-de-sac fluid on US | At ovulation | Objective confirmation |
Pt with bmi of 16 and other features are normal presenting with subfertility, her husband's SFA is normal what is the best advice for the couple
Clinical Scenario
Diagnosis: Hypogonadotropic Hypogonadism / Functional Hypothalamic Anovulation
- Nutritional deficits and caloric restriction → decreased GnRH pulsatility
- → ↓ FSH and LH → anovulation/oligovulation
- This is classified as WHO Group I anovulation (hypogonadotropic hypoestrogenic)
Best Advice for the Couple
First-line and Most Important: Weight Gain
"Lifestyle modifications should be recommended in patients with low BMI." — Harrison's Principles of Internal Medicine, 22e
"Being underweight (BMI < 19) increases time to conception 4-fold." — Kaplan & Sadock's Comprehensive Textbook of Psychiatry
- Weight gain to a BMI ≥ 18.5 is the single most important and first-line intervention.
- Correcting the energy deficit often restores spontaneous GnRH pulsatility and spontaneous ovulation without any pharmacological treatment.
- The term "functional" in functional hypothalamic anovulation specifically implies that correcting the underlying behavioral/nutritional cause reverses the ovulatory dysfunction.
- Conception after weight restoration is associated with better pregnancy outcomes — ovulation induction in low-weight women carries risks of premature labour and intrauterine growth retardation (IUGR).
Why NOT to Jump to Ovulation Induction First
- It does not correct the underlying metabolic derangement.
- It does not restore bone mineral density (these women are also at risk of osteoporosis).
- Pregnancy in a severely underweight woman risks preterm labour, IUGR, and fetal neuropsychological compromise (due to concomitant euthyroid sick syndrome/hypercortisolaemia).
- It may mask ongoing psychological/nutritional dysfunction.
Evaluate for Underlying Cause of Low Weight
- Screen for anorexia nervosa / eating disorder (amenorrhea occurs in 66–84% of anorexia patients).
- Screen for female athlete triad (relative energy deficiency in sport).
- Screen for psychosocial stressors.
- If an eating disorder is identified → specialized psychiatric/nutritional treatment is indicated first.
Additional General Preconception Advice
- Time intercourse every 1–2 days during the fertile window (5–6 days prior to ovulation).
- Folic acid supplementation.
- Avoid smoking (increases infertility risk by 60%) and limit caffeine (≤2 cups/day).
- Monitor BBT or use urinary LH kits once menstrual cycles resume after weight restoration.
If Weight Restoration Fails to Restore Ovulation
- Ovulation induction with letrozole or clomiphene citrate (first-line oral agents)
- Followed by injectable gonadotropins if oral agents fail
- Pulsatile GnRH therapy is the most physiological option for hypogonadotropic anovulation
Summary Answer
The best advice is weight gain to a BMI ≥ 18.5. This is the primary, first-line treatment. Pharmacological ovulation induction should only be considered after weight restoration, and even then, the risks of pregnancy at low weight must be discussed. Screening for an eating disorder is mandatory.
Indication to give lentrozole and clomiphiene in ovulation induction
Indications for Clomiphene Citrate and Letrozole in Ovulation Induction
Shared Indication: Anovulatory / Oligo-ovulatory Infertility (WHO Group II)
Clomiphene Citrate (Selective Estrogen Receptor Modulator — SERM)
Indications:
- Anovulatory infertility — primary first-line oral agent, especially where:
- Patient has adequate endogenous oestrogen levels
- Normal FSH and prolactin levels
- Intact hypothalamic-pituitary axis capable of releasing LH and FSH
- PCOS-associated anovulation — historically the first-line drug of choice
- Normogonadotropic, normoestrogenic anovulation in general (WHO Group II)
- Can be combined with metformin in PCOS to increase ovulation rates
NOT indicated / Less effective in:
- Hypogonadotropic (WHO Group I) patients — already have poor oestrogen supply; clomiphene is ineffective as it depends on an intact pituitary response
- Hyperprolactinaemia — treat the prolactin excess first
- Ovarian failure (WHO Group III) — unresponsive to any ovulation induction
Mechanism:
Letrozole (Aromatase Inhibitor)
Indications:
- PCOS-associated anovulatory infertility — now preferred first-line over clomiphene based on:
- Higher ovulation, pregnancy, and live birth rates (cumulative live birth: 27.5% vs 19.1% for clomiphene in PCOS)
- Lower multiple pregnancy rate (3.4% vs 7.4%)
- Better outcomes in obese women with PCOS (BMI >30)
- Clomiphene-resistant cases — where clomiphene fails to induce ovulation
- Where endometrial thinning is a concern with clomiphene (letrozole does not have the anti-oestrogenic effect on the endometrium)
- Women with thin endometrium on clomiphene — switch to letrozole
Note: Letrozole is FDA-approved for breast cancer only — its use for ovulation induction is off-label and patients must be counselled accordingly.
Mechanism:
Comparative Summary
| Feature | Clomiphene | Letrozole |
|---|---|---|
| Class | SERM | Aromatase inhibitor |
| FDA approval for OI | Yes | Off-label |
| First-line in PCOS | Historically yes | Currently preferred |
| Live birth rate (PCOS) | ~19% | ~28% |
| Multiple pregnancy rate | ~8% (mostly twins) | ~3–4% |
| Endometrial effect | Thinning (anti-oestrogenic) | Neutral / better |
| Effective in hypo-oestrogenic | No | No |
| Obese PCOS | Less effective | Superior |
| Starting dose | 50 mg/day × 5 days (days 3–7) | 2.5 mg/day × 5 days (days 3–7) |
| Max dose | 200–250 mg/day | 7.5 mg/day |
| Max cycles | 6 ovulatory / 12 total | Same |
Contraindications (Both Agents)
- Pregnancy (Pregnancy Category X)
- Liver disease
- Pre-existing large ovarian cysts
- Ovarian failure
When to Move Beyond Oral Agents
- Failure to ovulate after adequate trials of both agents
- Endometrial thinning persists despite adequate oestradiol
- Hypogonadotropic hypoestrogenic anovulation (WHO Group I) — these patients need exogenous gonadotropins or pulsatile GnRH
43 year old mother with 2 children and done LRT in last pregnancy coming to sub fertility clinic for another pregnancy,what is the best advice to give to this patient
Clinical Scenario Analysis
| Factor | Significance |
|---|---|
| Age: 43 years | Advanced maternal age — declining ovarian reserve, ↑ aneuploidy risk |
| LRT (Laparoscopic Reversal of Tubal ligation) done in last pregnancy | Both tubes have already been ligated AND reversed once — very limited residual tubal length expected |
| Parity: 2 children | Proven fertility in the past |
| Presenting to subfertility clinic | Seeking further conception |
Key Question: Tubal Reversal Again vs. IVF?
Best Advice: IVF (In Vitro Fertilization) is the preferred option — NOT repeat tubal reversal
"IVF should be considered in lieu of sterilization reversal for older patients or those with diminished ovarian reserve, severe pelvic adhesions, additional infertility factors, or prior unsuccessful reanastomosis." — Berek & Novak's Gynecology
- Age >35 years (she is 43) — the single strongest predictor of poor reversal outcome; success rates are best when age <35
- Prior reanastomosis already performed — a second reversal is extremely unlikely to succeed and residual tubal length will be critically short
- Diminished ovarian reserve expected at 43 — needs formal assessment before any intervention
Full Counselling Framework
1. Assess Ovarian Reserve First
- AMH (Anti-Müllerian Hormone)
- Antral follicle count (AFC) on transvaginal ultrasound
- Day 3 FSH and Oestradiol
At age 43, ovarian reserve is typically significantly reduced. Poor reserve may render even IVF futile without donor eggs.
2. Counsel on Age-Related Risks
- Advanced maternal age (>35) carries higher risk of aneuploidy (chromosomally abnormal embryos)
- At age 40, the risk of aneuploidy is approximately 9× higher than younger women
- Preimplantation Genetic Testing for Aneuploidy (PGT-A) with IVF can screen embryos and improve implantation rates at this age
- Higher risk of miscarriage, gestational diabetes, hypertension, placental complications, and caesarean section
3. IVF is the Treatment of Choice — Reasons
| Against Repeat Reversal | For IVF |
|---|---|
| Age 43 — poor predictor for reversal success | Bypasses tubes entirely |
| Prior reanastomosis already done — minimal residual tubal length | Higher success rates at this age |
| Success rates of reversal: best age <35 and tubal length >4 cm | Can combine with PGT-A for aneuploidy screening |
| Ectopic pregnancy risk following reversal approaches 10–18% | Lower ectopic risk |
| Diminished ovarian reserve likely at 43 | Allows embryo selection |
Pregnancy rates following microsurgical tubal reanastomosis are 55–81%, but success is predicted by age <35, isthmic anastomosis, and residual tubal length >4 cm. None of these are likely to be met here. — Berek & Novak's Gynecology
4. Discuss Realistic IVF Success Rates at 43
- IVF success rates decline sharply with age — live birth rates per cycle at 43 are generally <5–10% with own eggs
- Multiple cycles may be needed
- Donor egg IVF offers significantly higher success rates if own ovarian reserve is poor — this should be openly discussed
- Counsel on financial, psychological, and time burden
5. General Preconception Advice (If She Proceeds)
- Folic acid supplementation (5 mg/day given advanced maternal age)
- Optimise BMI, stop smoking, limit caffeine (<2 cups/day)
- Intercourse frequency counselling
- Screen for hypertension, diabetes, thyroid disease
- Counsel about increased obstetric risks at 43
Summary Answer
The best advice is IVF — not repeat tubal reversal. At age 43 with a prior tubal reanastomosis already performed, repeat reversal is not appropriate. Ovarian reserve must be assessed first. If reserve is adequate, IVF ± PGT-A gives the best chance of a successful pregnancy. If reserve is poor, donor egg IVF should be discussed. The couple must be counselled realistically about the significantly reduced success rates at this age and the increased obstetric risks.
43 year old mother with 2 children and done LRT in last pregnancy coming to sub fertility clinic for another pregnancy,what is the best advice to give to this patient, she also has mild endometriosis
Clinical Problem Summary
| Factor | Impact |
|---|---|
| Age 43 | Advanced maternal age — ↓ ovarian reserve, ↑ aneuploidy |
| Laparoscopic Tubal ligation (LRT) at last delivery | Tubal factor — tubes are occluded |
| Mild endometriosis (Stage I–II) | Additional infertility factor |
Best Advice: IVF is the treatment of choice
Rationale — Factor by Factor
1. Tubal Ligation → IVF over Reversal
"IVF should be considered in lieu of sterilization reversal for older patients or those with diminished ovarian reserve, severe pelvic adhesions, additional infertility factors, or prior unsuccessful reanastomosis." — Berek & Novak's Gynecology
- She is 43 (age <35 is the key predictor of good reversal outcome)
- She has mild endometriosis — an additional infertility factor, which by itself is an indication to prefer IVF over reversal
- Reversal success requires residual tubal length >4 cm — unpredictable here
- Ectopic pregnancy risk post-reversal: 10–18%
- IVF completely bypasses the tubes, removing tubal and endometriosis-related barriers simultaneously
2. Mild Endometriosis → IVF is Reasonable First-Line
"IVF is considered a reasonable first-line therapy for endometriosis-associated infertility because of the short time to pregnancy and avoidance of surgery." — Berek & Novak's Gynecology
- Mild endometriosis reduces monthly fecundity rates (MFR) and cumulative pregnancy rates
- It causes: anovulatory dysfunction, luteinized unruptured follicle syndrome, impaired follicle growth, altered pelvic immunity
- Laparoscopic ablation of mild endometriosis improves spontaneous pregnancy rates (31% treated vs 17% untreated), BUT:
- This benefit applies to younger women with patent tubes aiming for spontaneous conception
- At 43 with occluded tubes, there is no route for spontaneous conception — laparoscopic treatment of endometriosis alone would not help
- Surgery would only add risk and delay at this age
- Hormonal suppression of endometriosis has minimal benefit for fertility — should NOT be used while trying to conceive
3. Age 43 — Time is Critical
- At 43, ovarian reserve is declining rapidly — every month of delay reduces chances
- IVF offers the shortest time to pregnancy
- Aneuploidy risk is high → Preimplantation Genetic Testing for Aneuploidy (PGT-A) should be discussed to improve implantation rates and reduce miscarriage
- Live birth rates per IVF cycle at 43 with own eggs are low (~5–10%) — realistic counselling is essential
- If ovarian reserve is severely diminished → donor egg IVF offers significantly higher success rates
Step-by-Step Management Plan
Step 1: Assess Ovarian Reserve
- AMH (Anti-Müllerian Hormone)
- Day 3 FSH + Oestradiol
- Antral Follicle Count (AFC) on transvaginal ultrasound → This determines whether own-egg IVF is viable or donor egg should be recommended
Step 2: Uterine Assessment
- Saline infusion sonography or hysteroscopy — ensure uterine cavity is normal before proceeding to IVF
- Endometriosis can cause endometrial receptivity issues
Step 3: IVF ± PGT-A
- Proceed with IVF using controlled ovarian hyperstimulation
- Consider PGT-A on embryos to select euploid embryos — reduces miscarriage and improves live birth rate at this age
- Note: Endometriosis reduces implantation rates per embryo in IVF compared to tubal factor infertility — counsel accordingly
Step 4: Endometrioma Management (if present)
- If ovarian endometrioma is found: weigh risks carefully
- Surgical removal of endometriomas reduces ovarian reserve (decreased follicle numbers, fewer retrieved oocytes in up to 13% of cases)
- Generally, avoid surgery on endometriomas just before IVF unless they interfere with oocyte retrieval
Step 5: General Preconception Counselling
- Folic acid 5 mg/day (high-dose given age >35)
- Optimise BMI, stop smoking, limit caffeine
- Counsel on obstetric risks at 43: gestational hypertension, GDM, placenta praevia, caesarean section, IUGR
- Counsel on risk of fetal aneuploidy and offer prenatal testing (NIPT/amniocentesis) if pregnancy is achieved
Summary Answer
The best advice is IVF — not tubal reversal surgery and not laparoscopic treatment of endometriosis alone.At 43, with occluded tubes from prior tubal ligation AND mild endometriosis as an additional infertility factor, IVF is the most appropriate, time-efficient, and evidence-based strategy. Ovarian reserve must be assessed first to determine feasibility of own-egg IVF versus donor egg IVF. PGT-A should be discussed to improve outcomes at this age. Laparoscopic treatment of mild endometriosis or tubal reversal surgery would both delay treatment, carry surgical risk, and are unlikely to result in natural conception given the combined barriers present.
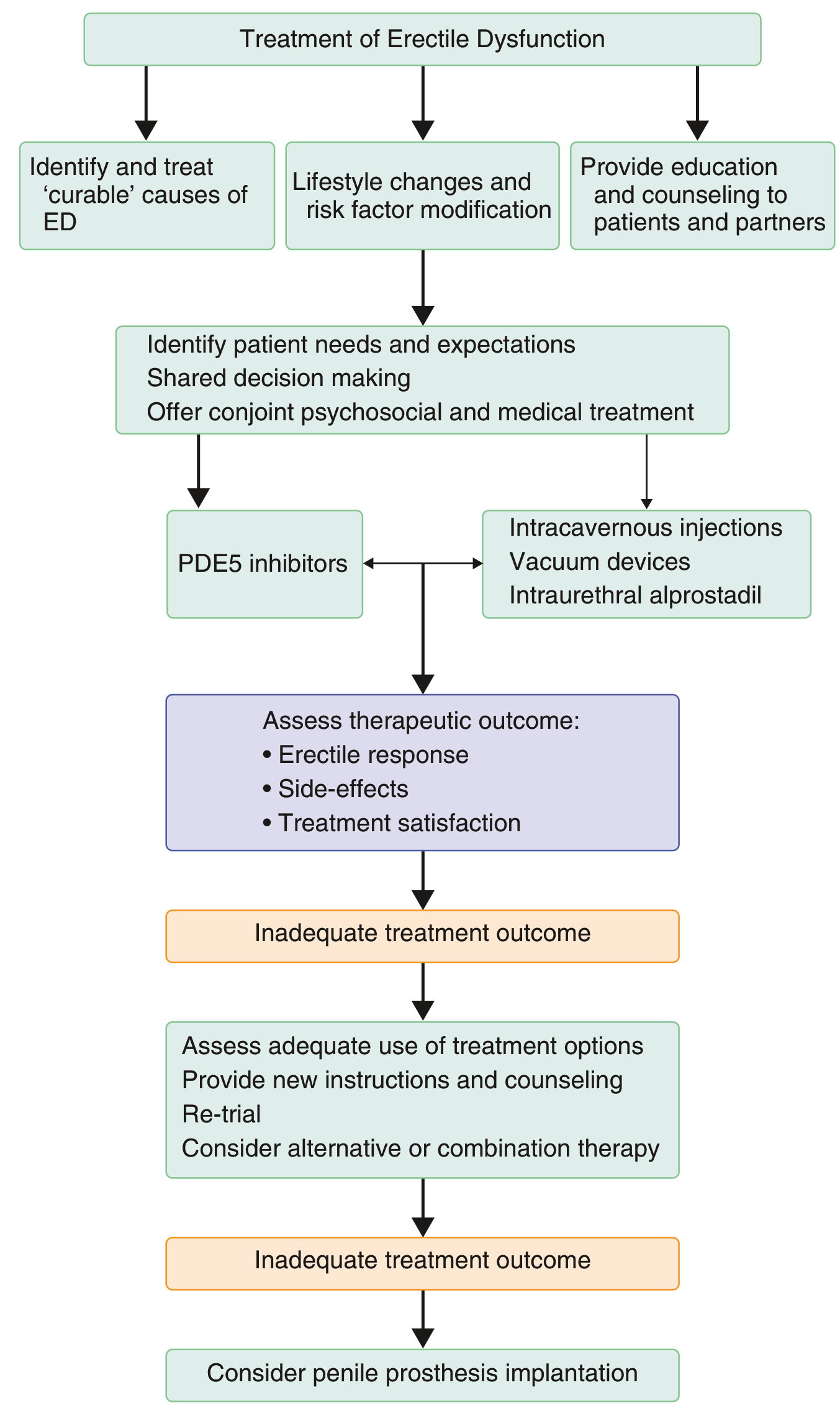
Management and escalation of impotence
Treatment Algorithm
Step 0: Initial Assessment
- Full sexual and medical history including partner history
- Identify reversible/curable causes: medication side effects, hormonal disorders, vascular disease, neurological disease, psychogenic causes
- Examination: genitourinary, cardiovascular, endocrine, neurological systems
- Investigations:
- Morning serum testosterone
- Fasting glucose / HbA1c
- Lipid profile
- Prolactin, LH (if hypogonadism suspected)
- PSA (if prostate disease suspected)
- Use validated tools: Sexual Health Inventory for Men (SHIM)
Simultaneous First Steps (All Patients)
| Action | Details |
|---|---|
| Identify & treat curable causes | Stop offending drugs (β-blockers, thiazides, SSRIs, spironolactone, cimetidine, antiandrogens); treat hypogonadism, hyperprolactinaemia, diabetes |
| Lifestyle modification | Weight loss (especially obesity), control diabetes and hypertension, stop smoking, reduce alcohol — all improve erectile function |
| Education & psychosexual counselling | Patient AND partner; cognitive-behavioural therapy; manage performance anxiety |
Line 1: Oral PDE5 Inhibitors (First-Line Pharmacotherapy)
| Drug | Dose | Duration of action | Timing |
|---|---|---|---|
| Sildenafil (Viagra) | 25–100 mg (start 50 mg) | 4–6 hours | 20–60 min before intercourse (on demand) |
| Vardenafil (Levitra) | 5–20 mg | 4–6 hours | On demand |
| Tadalafil (Cialis) | 10–20 mg (on demand) or 2.5–5 mg daily | Up to 36 hours | On demand or daily dosing |
| Avanafil | Available option | Shorter onset | On demand |
Key Contraindication:
- Absolutely contraindicated with nitrates — risk of severe hypotension
- Caution with α-blockers (orthostatic hypotension)
Special populations:
- Post-radical prostatectomy: Early rehabilitation with PDE5 inhibitors promotes recovery of erectile function
- Antidepressant-induced ED (SSRIs): Add PDE5 inhibitor OR switch to bupropion OR drug holiday
- Androgen deficiency (testosterone <275 ng/dL + symptoms): Testosterone replacement first — improves response to PDE5 inhibitors
Line 2: Second-Line Options
A. Intracavernosal Injection (ICI)
- Alprostadil (PGE1) 2.5–25 mcg — alone or combined with:
- Papaverine (non-selective PDE inhibitor)
- Phentolamine (α-blocker)
- "Trimix" = alprostadil + papaverine + phentolamine
- Injected with 27–30 gauge needle into corpus cavernosum
- Side effects: pain, cavernosal fibrosis (stop if fibrosis develops — may indicate early Peyronie's disease)
- Botulinum toxin injection: improves ED in ~40–50% with early Peyronie's
B. Intraurethral Alprostadil (MUSE)
- Suppository 125–1000 mcg inserted into urethra
- Works via local absorption into corpora cavernosa
- Success rate: 30–66%
- Less invasive alternative to injection
C. Vacuum Erection Device (VED)
- Mechanical, non-pharmacological
- Useful in men who failed oral therapy and decline injections
- Can combine with PDE5 inhibitors (especially post-prostatectomy)
D. Other agents
- Yohimbine: Modest evidence, α2-blocker
- Korean red ginseng: Stronger evidence among herbal options
- L-arginine + low-intensity shock wave therapy + PDE5 inhibitors: Emerging combination evidence
- Apomorphine (sublingual dopamine agonist): Second-line option
Assess Therapeutic Outcome After Each Line
- Erectile response
- Side effects
- Patient and partner satisfaction
- Reassess whether treatment was used correctly
- Provide new instructions and counselling
- Re-trial at optimal dose/timing
- Consider combination therapy (e.g., PDE5 + VED, or PDE5 + ICI)
Line 3: Surgical — Penile Prosthesis (Third-Line / Definitive)
- Fail or cannot use oral and second-line therapies
- Prefer a permanent solution
Types:
| Type | Description |
|---|---|
| Semi-rigid (malleable) | Always partially erect; simpler, fewer mechanical failures |
| Inflatable (2- or 3-piece) | More natural erection/flaccidity; higher patient satisfaction |
- Mechanical failure in 10–20% of inflatable devices by 10 years
- High long-term patient and partner satisfaction with proper selection
- Complications: corporal perforation, urethral injury, infection, haematoma, implant failure
Summary: Escalation Ladder
Step 0: Treat reversible causes + Lifestyle changes + Counselling
↓
Line 1: PDE5 Inhibitors (oral) ± Testosterone replacement if hypogonadal
↓ (if inadequate)
Line 2: Intracavernosal injection / Intraurethral alprostadil / Vacuum device
↓ (if inadequate — reassess, re-trial, combination therapy)
Line 3: Penile prosthesis implantation (surgical)
Management and escalation for fibroids depending on categories
Management and escalation for fibroids depending on categories
Fibroid Management & Escalation by Category
FIGO Classification (Location-Based Categories)
| Type | Location |
|---|---|
| Type 0 | Submucosal — pedunculated (entirely intracavitary) |
| Type 1 | Submucosal — <50% intramural |
| Type 2 | Submucosal — ≥50% intramural |
| Type 3–5 | Intramural (no cavity distortion → cavity distortion) |
| Type 6–7 | Subserosal — sessile → pedunculated |
| Type 8 | Cervical / parasitic / broad ligament |
Management by Clinical Category
Category A: Asymptomatic Fibroids (Any Type)
- No treatment needed
- Reassure: benign, not premalignant (~1:1,000–1,500 risk of concurrent uterine sarcoma)
- Fibroids shrink naturally after menopause
- Periodic clinical ± ultrasound review
Category B: Heavy Menstrual Bleeding (HMB)
Step 1 — Medical (Non-hormonal / Hormonal Control)
| Drug | Role |
|---|---|
| Tranexamic acid | Antifibrinolytic; reduces blood loss |
| NSAIDs (mefenamic acid, naproxen) | Reduce blood loss + dysmenorrhoea |
| Combined OCP | Cycle regulation; reduces HMB |
| LNG-IUS (Mirena) | Highly effective for HMB; limited if cavity distorted |
| Oral progestogens | Short-term endometrial suppression |
Step 2 — Medical (Fibroid Shrinkage / Pre-operative Optimisation)
| Drug | Details |
|---|---|
| GnRH agonists (leuprolide, goserelin) | Shrink fibroids 30–50%; correct anaemia; use ≤6 months + add-back HRT |
| GnRH antagonists (elagolix + E2/NETA; relugolix + E2/NETA) | Oral; reduce HMB + preserve bone density; newer long-term option |
| Mifepristone 5–10 mg/day | Anti-progesterone; reduces size + symptoms (transient) |
| Ulipristal acetate 5 mg × 13 weeks | SPRM; effective but hepatotoxicity concerns limit use |
Step 3 — Minimally Invasive / Surgical
| Procedure | Best for | Fertility |
|---|---|---|
| Hysteroscopic myomectomy | Type 0, 1, 2 — submucosal | ✅ Preserved |
| Endometrial ablation | HMB; no desire for fertility; cavity not severely distorted | ❌ Not preserved |
| UAE (Uterine Artery Embolization) | Symptomatic fibroids; not seeking fertility | Relative — ovarian reserve risk |
| HIFU / MR-guided focused ultrasound | Non-invasive fibroid ablation; emerging | Relative |
| Radiofrequency ablation (Acessa/Sonata) | Laparoscopic or transcervical; targeted | Relative |
Step 4 — Surgery
| Procedure | Indication | Fertility |
|---|---|---|
| Laparoscopic myomectomy | Intramural/subserosal; fertility desired; ≤4–5 fibroids | ✅ |
| Open (abdominal) myomectomy | Large, multiple, or complex fibroids | ✅ |
| Hysterectomy | Definitive; completed family; failed all other options | ❌ Permanent |
Category C: Bulk Symptoms (Pressure, Urinary frequency, Constipation)
- GnRH agonist/antagonist → temporary shrinkage + symptom relief
- UAE → effective for volume reduction; 28% require hysterectomy within 5 years
- HIFU / Radiofrequency ablation
- Laparoscopic or open myomectomy (if fertility desired)
- Hysterectomy (definitive)
Category D: Infertility / Subfertility
| Fibroid Type | Effect | Management |
|---|---|---|
| Submucosal (Type 0–2) | Strong negative impact — distorts cavity, impairs implantation | Hysteroscopic myomectomy — first-line |
| Intramural with cavity distortion | Impairs implantation | Laparoscopic/open myomectomy |
| Intramural without cavity distortion | Modest/controversial effect | Individualise; may proceed to IVF |
| Subserosal (Type 6–7) | Minimal impact on fertility | No intervention needed for fertility |
- GnRH agonists: not used during active attempts to conceive (only pre-operative)
- UAE: avoid if fertility is desired — risk of reduced ovarian reserve, uterine ischaemia
- After myomectomy: wait 3–6 months before attempting conception
Category E: Fibroids in Pregnancy
| Complication | Management |
|---|---|
| Red degeneration (most common) | Conservative: analgesia, NSAIDs, hydration |
| Pedunculated fibroid torsion | Surgical if unresponsive to conservative Mx |
| Obstructed labour (cervical/lower segment) | Elective caesarean section |
| Myomectomy during pregnancy | Avoided — high haemorrhage risk; only for torsion unresponsive to Mx |
Category F: Perimenopausal / Postmenopausal Fibroids
- Expectant management — fibroids regress after menopause
- Surgical intervention if:
- Rapid post-menopausal growth → exclude leiomyosarcoma
- Persistent/new significant symptoms
- Diagnostic uncertainty
Escalation Ladder (Universal)
ASYMPTOMATIC
→ Observe / Reassure
SYMPTOMATIC
↓
Step 1: Medical symptom control (Tranexamic acid, NSAIDs, OCP, LNG-IUS)
↓
Step 2: Fibroid shrinkage agents (GnRH agonist/antagonist, Mifepristone)
↓
Step 3: Minimally invasive
• Submucosal → Hysteroscopic myomectomy
• Any location → UAE / HIFU / Radiofrequency ablation
↓
Step 4: Surgical myomectomy
• Laparoscopic (preferred) or Open
• Fertility-sparing
↓
Step 5: Hysterectomy (Definitive — no future fertility)
SPECIAL:
• Infertility + submucosal → Hysteroscopic myomectomy first
• Infertility + intramural → Myomectomy; avoid UAE
• Perimenopausal → Bridge with GnRH agonist to menopause
"The definitive treatment for fibroids is hysterectomy, but less invasive options are often preferable." "Myomectomy provides better outcomes than uterine artery embolization" for women seeking fertility. — Goldman-Cecil Medicine; Berek & Novak's Gynecology
Indications, procedure method, precautions and complications of hysterosalpingography
Hysterosalpingography (HSG)
1. INDICATIONS
Uterine Causes
- Infertility (uterine factor)
- Endometrial adhesions (Asherman's syndrome)
- Submucosal polyps
- Pedunculated endometrial leiomyomas (fibroids)
- Uterine anomalies (bicornuate, septate, unicornuate uterus)
- DES (Diethylstilbestrol) exposure — T-shaped uterus
- Recurrent (habitual) miscarriages
- Cervical incompetency (controversial)
- Abnormal uterine bleeding (where saline infusion sonohysterography may be used)
Tubal Causes
- Infertility (tubal factor) — assessment of tubal patency
- Salpingitis isthmica nodosa (honeycombing appearance on HSG)
- Periadnexal adhesive disease
- Tubal cannulation procedures
- Follow-up after ectopic pregnancy (medical or surgical treatment)
Pre/Post-operative Evaluation
- Pre/post tubal reanastomosis, reimplantation, tuboplasty
- Pre/post myomectomy
- Uterine septal resection / metroplasty
- Confirmation of tubal occlusion after Essure/sterilisation procedure
- Localisation of a lost IUD (though ultrasound is preferred)
2. CONTRAINDICATIONS
| Contraindication | Reason |
|---|---|
| Active PID or suspected pelvic infection | Risk of spreading infection; >10% PID rate if hydrosalpinx present |
| Pregnancy | Procedure performed after menses and before ovulation (days 7–12) to avoid |
| Active uterine/vaginal bleeding | Obscures visualisation |
| Iodine/contrast allergy (relative) | Pretreat with glucocorticoids; use non-ionic contrast |
| Known hydrosalpinx | Risk of rupture and severe PID (>10%) |
| Recent intrauterine surgery | Wait for healing |
| Pelvic tenderness on bimanual examination | Contraindication if suspected inflammation |
3. TIMING
- Performed after menses but before ovulation: cycle days 7–12
- Avoids potential early pregnancy
- Takes advantage of thinner proliferative phase endometrium for better visualisation
4. PRE-PROCEDURE PRECAUTIONS
Patient Preparation
- Informed consent — explain procedure, findings, risks, alternatives
- Pregnancy test prior to procedure
- Screen for iodine allergy — pretreat with glucocorticoids if allergic
- Antibiotic prophylaxis:
- Controversial for routine use
- Doxycycline 100 mg twice daily — begin day before, continue 3–5 days post-procedure
- Indicated in high-risk patients (history of PID, hydrosalpinx seen)
- Pre-medication: Ibuprofen or NSAID 30–60 minutes before to reduce cramping
- Intracervical lidocaine can be injected for additional pain relief
- Warm the contrast dye — reduces cramping
Equipment Check
- Contrast medium pre-loaded into cannula
- Bubbles must be expelled — may mimic intrauterine polyps
5. PROCEDURE
Step-by-Step Technique
- Position: Patient in dorsal lithotomy position on high-resolution image-intensifier fluoroscopy table
- Bimanual pelvic examination: Assess degree of uterine flexion/retroflexion; exclude pelvic tenderness
- Insert vaginal speculum
- Cleanse cervix and upper vagina with antiseptic solution
- Grasp anterior lip of cervix with tenaculum (slowly, to minimise pain) — if required by cannula type
- Insert and seat the cannula through the cervix past the internal os:
- Various catheter types available: Mencini double balloon, HUI, pediatric Foley, Thurmond-Rosch, H/S Elliptosphere — each seated differently (balloon inflation, spring platform, suction cup)
- Remove speculum (non-radiopaque plastic speculum may be left in)
- Position patient recumbent for fluoroscopy
- Inject contrast dye slowly:
- 1–3 mL initially — reveals intrauterine detail (spot film taken); larger volumes may obscure small polyps or adhesions
- Continue until tubes start to fill — spot film at this stage shows tubal detail before dye obscures it
- Continue until bilateral intra-abdominal spill is confirmed — confirms bilateral tubal patency
- A delayed film may show peritubal adhesion detail
- Rolling patient side to side can help visualise lesions (but increases radiation exposure)
- If one tube not visualised: relax pressure on syringe and wait 1–2 minutes to relieve tubal spasm before re-attempting
- Remove instruments
- Observe patient for 30 minutes post-procedure — watch for allergic reaction and heavy bleeding
Selective Tubal Cannulation (Specialist Technique)
- Used for unilateral/bilateral non-visualisation, salpingitis isthmica nodosa, or proximal tubal blockage
- Coaxial catheter system threaded under radiological guidance to the tubal ostium
- Guidewire advanced into tube, contrast confirms placement
- Therapeutic — can open proximal tubal blockage
6. CONTRAST MEDIA
| Type | Features |
|---|---|
| Water-soluble ionic (Salpix, Sinografin, Conray 60) | Most commonly used; less expensive |
| Water-soluble non-ionic (Hypaque-60) | Used when ionic dye risk is concern |
| Oil-based (Lipiodal/Ethiodol) | Higher live birth rates (38% vs 28%) — therapeutic effect by flushing inspissated mucus; risk of oil embolism if intravasation |
A large RCT (1,119 women) found significantly higher live birth rates with oil-based contrast (38% vs 28%; RR 1.38) compared to water-based. — Berek & Novak's Gynecology
7. NORMAL HSG APPEARANCE
- Smooth triangular endometrial cavity
- Narrow smooth isthmic portion of tube
- Progressively enlarging, increasingly convoluted ampullary tube with internal mucosal folds
- Free peritoneal spill bilaterally — dye dispersed between bowel loops
8. DIAGNOSTIC ACCURACY
- Compared to laparoscopy (gold standard):
- Sensitivity: 65% for tubal patency
- Specificity: 83% for tubal patency
- False positive rate (suggesting occlusion) and false negative rate may be as high as 25% each
- Selective cannulation reduces false positives from proximal tubal spasm
9. COMPLICATIONS
| Complication | Details |
|---|---|
| Pelvic Inflammatory Disease (PID) | 0.3–3.1% overall; >10% if hydrosalpinx present — most significant complication |
| Vasovagal reaction | Bradycardia, hypotension during procedure |
| Vascular intravasation of contrast | Dye enters bloodstream — discontinue immediately; oil-based dye → risk of pulmonary oil embolism |
| Uterine/tubal perforation | Rare; discontinue procedure immediately |
| Rupture of hydrosalpinx | Can occur during procedure |
| Cervical laceration / tenaculum site bleeding | Rare; may require suturing |
| Allergic reaction to contrast dye | Pretreat if iodine allergy known |
| Haemorrhage | Rare |
| Granuloma formation | Late, rare complication; associated with oil-based dye |
| Severe pain | Usually transient cramping; NSAIDs pre-medicate |
| Radiation exposure | Minimal (50–500 mrem); comparable to 1–2 CT scans |
10. THERAPEUTIC VALUE
- HSG itself may improve fertility — by flushing inspissated mucus and debris from tubes
- Oil-based contrast has significantly higher live birth rates than water-based (therapeutic flushing effect)
- Selective cannulation can therapeutically open proximal tubal blockages
HSG vs Sonohysterography (SIS) — Key Comparison
| Feature | HSG | SIS |
|---|---|---|
| Radiation | Yes | No |
| Tubal patency | ✅ Gold standard for tubes | Limited (air-saline used as substitute) |
| Uterine cavity detail | Good | Superior (myometrium also visualised) |
| Differentiates uterine anomalies | Limited | Superior (especially with 3D) |
| Submucosal fibroids | Detects | Better characterisation |
| Therapeutic effect | Yes (oil-based contrast) | No |
| Anaesthesia required | No | No |
Regarding hormone replacement therapy after hysterectomy and bilateral salpingo oophorectomy and other indicators for HRT