Portal system anastomosis
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Finding Sources
Reading File
Loading Image
Finding Sources
I now have excellent textbook content and both diagrams. Here is the full answer:
Portal System Anastomoses (Portacaval / Portosystemic Anastomoses)
What Are They?
The hepatic portal system drains blood from the abdominal viscera (gut, spleen, pancreas, gallbladder) to the liver. At several locations, small communicating veins normally connect portal tributaries to systemic (caval) tributaries. Under normal conditions these channels carry minimal flow. When portal pressure rises (as in cirrhosis or portal vein thrombosis), blood is diverted through these collaterals in bulk, causing them to dilate into varices.
Diagram - Portosystemic Anastomoses
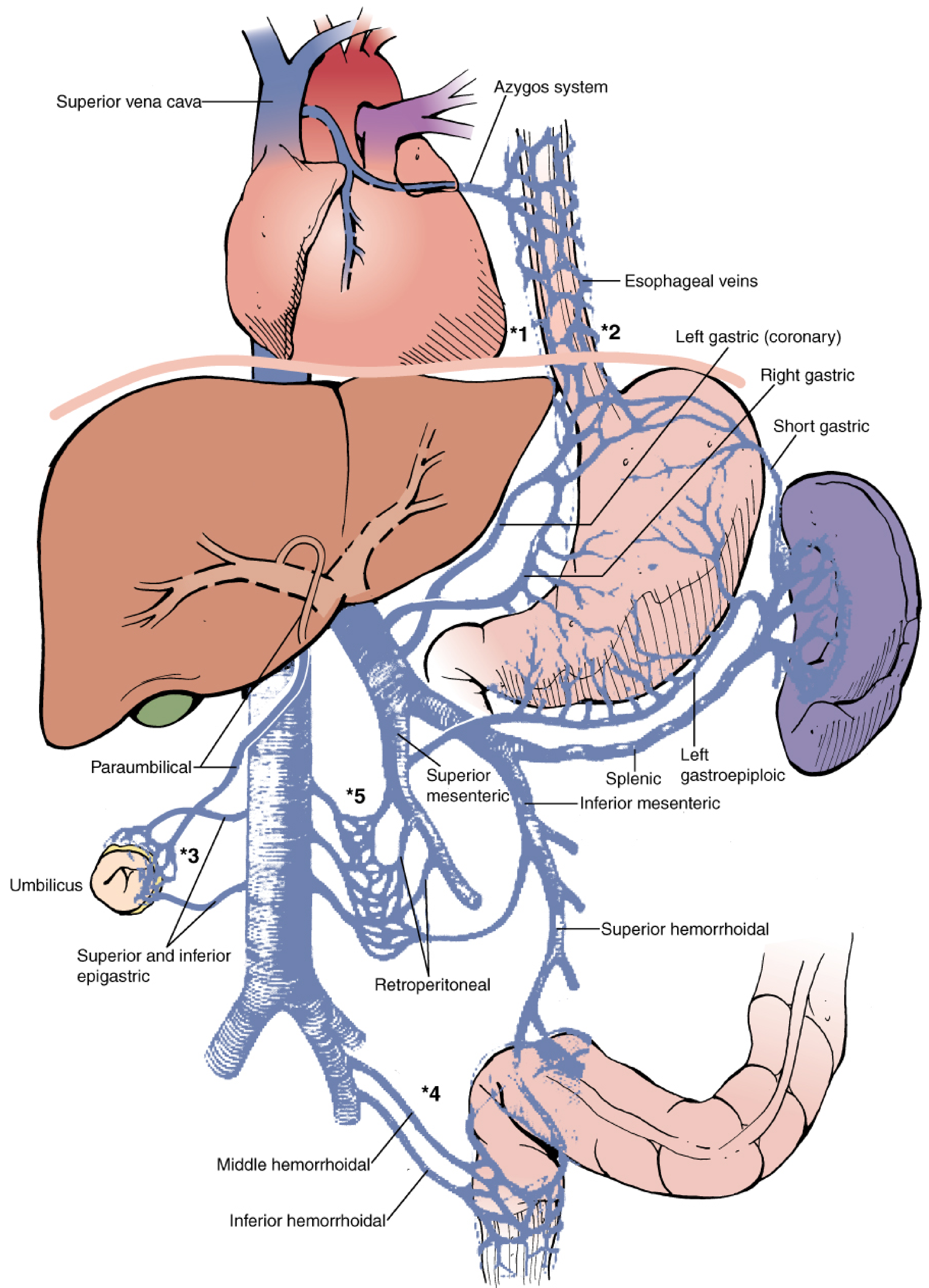
Fischer's Mastery of Surgery - sites of portosystemic collateral formation in portal hypertension
Major Sites of Anastomosis
1. Gastroesophageal Junction (Lower Esophagus / Cardia) - Most Clinically Important
| Portal side | Systemic side |
|---|---|
| Left gastric (coronary) vein + right gastric vein + short gastric veins | Esophageal veins → hemiazygos / azygos system → SVC |
- Clinical consequence: Esophageal and gastric varices
- Most dangerous site - varices are thin-walled, submucosal, susceptible to rupture causing massive upper GI hemorrhage
- Rupture is a medical emergency requiring urgent intervention (variceal banding, sclerotherapy, balloon tamponade, TIPS)
2. Anal Canal / Anorectal Junction
| Portal side | Systemic side |
|---|---|
| Superior rectal vein (branch of inferior mesenteric vein) | Middle and inferior rectal veins → internal iliac vein → IVC |
- Clinical consequence: Anorectal varices (distinct from hemorrhoids, though often confused)
- Less likely to bleed catastrophically than esophageal varices
3. Anterior Abdominal Wall / Umbilicus
| Portal side | Systemic side |
|---|---|
| Para-umbilical veins (accompany the ligamentum teres / round ligament of the liver, remnant of the umbilical vein) connecting to the left branch of the portal vein | Superior and inferior epigastric veins → superficial veins of the abdominal wall |
- Clinical consequence: Caput medusae - dilated, tortuous superficial veins radiating from the umbilicus, visible on the abdominal wall
- Pathognomonic sign of portal hypertension
4. Retroperitoneal Connections
| Portal side | Systemic side |
|---|---|
| Superior mesenteric vein branches (veins of Retzius), retroperitoneal portions of the colon and duodenum | Retroperitoneal veins → IVC |
- Less dramatic clinically
- Relevant during surgery - unexpected retroperitoneal bleeding in cirrhotic patients
5. Bare Area of the Liver
| Portal side | Systemic side |
|---|---|
| Small intrahepatic portal tributaries | Diaphragmatic veins (phrenic veins) → IVC |
- Where the liver is in direct contact with the diaphragm (not covered by peritoneum)
- Minor collateral pathway
Summary Table
| Site | Portal Tributary | Systemic Tributary | Varix Formed |
|---|---|---|---|
| Lower esophagus/cardia | Left gastric vein | Azygos/hemiazygos | Esophageal varices |
| Anorectal junction | Superior rectal vein | Middle/inferior rectal veins | Anorectal varices |
| Umbilicus | Para-umbilical veins | Epigastric veins | Caput medusae |
| Retroperitoneum | SMV branches (veins of Retzius) | IVC tributaries | Retroperitoneal collaterals |
| Bare area of liver | Hepatic portal branches | Phrenic/diaphragmatic veins | Minor collaterals |
Clinical Significance of Portal Hypertension
When portal pressure exceeds ~10-12 mmHg (normal ~5-8 mmHg), collateral flow increases significantly. Key consequences:
- Esophageal varices - bleed in ~30% of cirrhotic patients; mortality per bleed ~20%
- Caput medusae - important physical examination finding; blood flows away from the umbilicus (distinguishes it from IVC obstruction, where flow goes upward in both flanks)
- Hepatic encephalopathy - portal blood bypasses the liver, so ammonia and other gut-derived toxins reach the systemic circulation without hepatic detoxification
- Splenomegaly and hypersplenism - back-pressure in the splenic vein
Memory Aid
"SURE" for the 4 main sites:
- Stomach/esophagus (left gastric → azygos)
- Umbilicus (para-umbilical → epigastric = caput medusae)
- Rectum (superior rectal → middle/inferior rectal)
- Retroperitoneum (SMV branches → IVC)
Sources: Gray's Anatomy for Students, pp. 333, 419-420; Fischer's Mastery of Surgery - 8th ed., p. 5301-5303
This is a shared conversation. Sign in to Orris to start your own chat.