Cholelithiasis
Reading File
Finding Sources
Finding Sources
Searching PubMed
cholelithiasis management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have all the information needed for a comprehensive answer. Let me compile this.
Cholelithiasis (Gallstones)
Definition and Epidemiology
Cholelithiasis refers to the presence of calculi (gallstones) within the gallbladder. More than 95% of all biliary tract disease is attributable to gallstones. They affect 10-20% of adults in high-resource countries, with an estimated >20 million persons in the United States having gallstones. More than 700,000 cholecystectomies are performed annually in the US at a cost of approximately $6 billion.
The classic mnemonic for risk is the "four Fs": Female, Fat (obese), Forty, and Fertile. Prevalence is highest in Native Americans (Pima, Hopi, Navajo groups - up to 75%) and in northern Europeans and North/South Americans.
Classification of Gallstones
There are two major types:
1. Cholesterol Stones (90% in Western countries)
- Composition: >50% crystalline cholesterol monohydrate
- Appearance: Pale yellow, round/ovoid, hard, finely granular surface; cross-section shows glistening radiating crystalline palisade. Multiple, faceted stones common.
- Radiology: Mostly radiolucent (10-20% radiopaque due to calcium carbonate)
- Arise exclusively in the gallbladder
2. Pigment Stones (predominant in East Asia/low-resource settings)
- Composition: Calcium salts of unconjugated bilirubin + inorganic calcium salts
- Black stones: Found in sterile gallbladder bile; contain oxidized polymers of calcium bilirubinate, calcium carbonate, calcium phosphate. Small (<1.5 cm), numerous, friable, spiculated; 50-75% radiopaque
- Brown stones: Found in infected bile ducts; contain calcium soaps (palmitate, stearate) + cholesterol; laminated, soft, greasy; radiolucent
Gross pathology images:
Fig. 18.60 - Cholesterol gallstones: multiple faceted yellow-brown stones filling the gallbladder, with thickened fibrotic wall from chronic cholecystitis (Robbins)
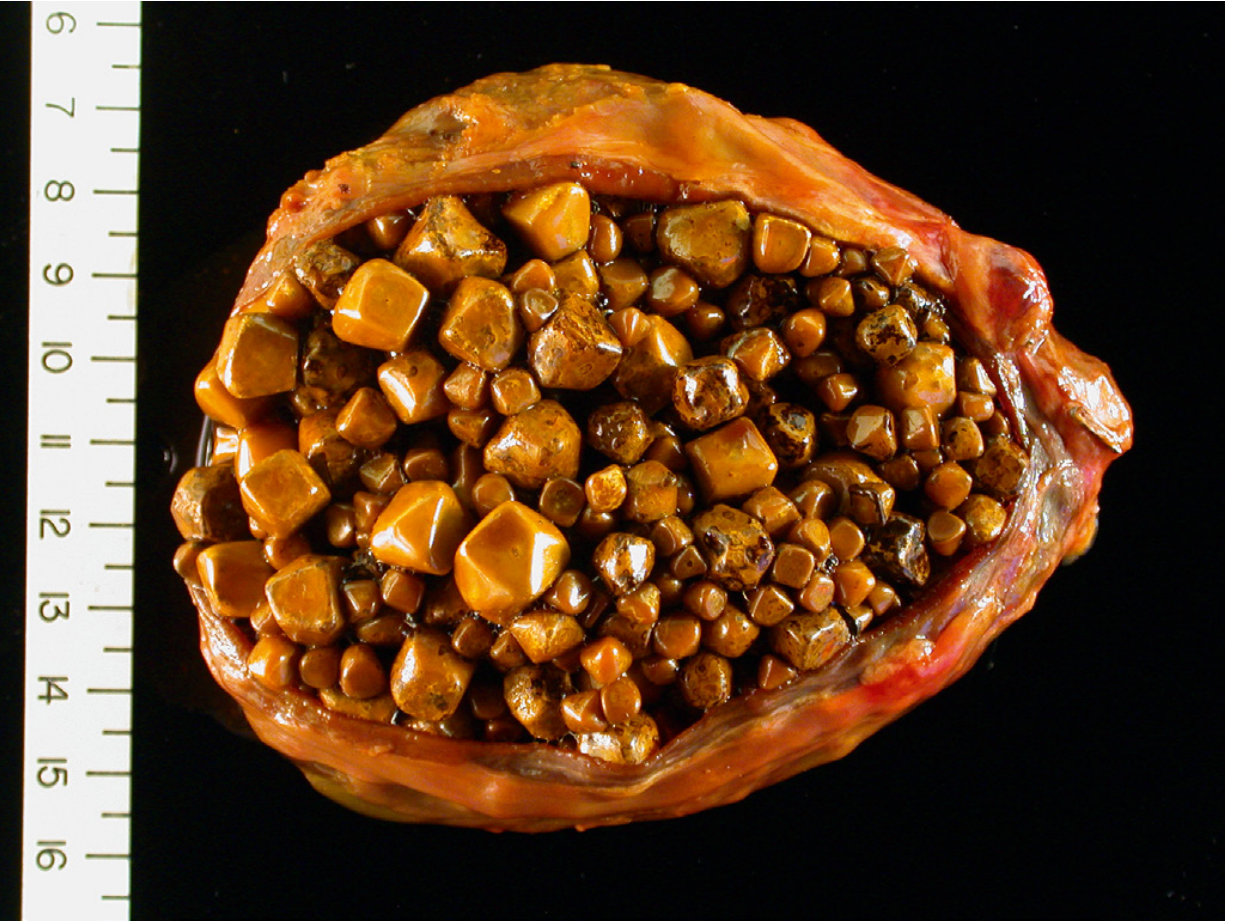
Fig. 18.62 - Pigment gallstones: several small, black, faceted stones in a patient with mechanical mitral valve prosthesis causing chronic intravascular hemolysis (Robbins)

Risk Factors
| Cholesterol Stones | Pigment Stones |
|---|---|
| Female sex, oral contraceptives, pregnancy | Chronic hemolytic anemias (sickle cell, spherocytosis, thalassemia) |
| Obesity, metabolic syndrome | Biliary infections (E. coli, Ascaris, liver flukes) |
| Advancing age | Ileal disease/resection (Crohn's disease), cystic fibrosis |
| Rapid weight loss | Rural > urban populations |
| Gallbladder stasis (TPN, prolonged fasting) | Parasitic infestations (Clonorchis sinensis) |
| Native American / Scandinavian descent | |
| Hyperlipidemia, diabetes mellitus | |
| ABCG8 gene variant (sterol transporter) | |
| Ceftriaxone use, estrogen therapy |
Pathogenesis
Cholesterol Stone Formation (4 key steps)
Cholesterol is solubilized in bile by forming micelles with bile salts and lecithins. Four conditions lead to stone formation:
- Supersaturation of bile with cholesterol (exceeds solubilizing capacity)
- Gallbladder hypomotility (stasis promotes nucleation)
- Accelerated cholesterol crystal nucleation
- Hypersecretion of mucus - traps nucleated crystals, leading to progressive accretion
Hormonal contribution: Estrogen increases hepatic LDL receptor expression and stimulates HMG-CoA reductase activity → excess biliary cholesterol secretion. This explains the increased risk with OCP use, pregnancy, and female sex.
Genetic contribution: A common variant of ABCG8 (sterol transporter gene) is strongly associated with cholesterol gallstone formation.
Pigment Stone Formation
- Black stones: Disorders with elevated unconjugated bilirubin (hemolytic anemias, ileal dysfunction). About 1% of bilirubin glucuronides are normally deconjugated; with chronically increased conjugated bilirubin secretion, enough deconjugated bilirubin accumulates to precipitate.
- Brown stones: Biliary infection leads to microbial β-glucuronidase release (from E. coli, Ascaris, Clonorchis sinensis) → hydrolysis of bilirubin glucuronides → free unconjugated bilirubin precipitates with calcium.
Clinical Features
Asymptomatic (majority)
- ~70-80% of patients with gallstones are asymptomatic
- The cumulative probability of developing biliary colic is 11.9% at 2 years, 16.5% at 4 years, and 25.8% at 10 years (GREPCO data)
- Cumulative probability of complications at 10 years: only ~3%
- Expectant management is appropriate for asymptomatic gallstones
Symptomatic - Biliary Colic
- Episodic, severe RUQ or epigastric pain (onset NOT consistently related to meals, contrary to popular belief)
- Pain typically lasts 30 minutes to several hours
- Associated nausea and vomiting
- Results from transient obstruction of the cystic duct by a stone
Complications
| Complication | Mechanism |
|---|---|
| Acute cholecystitis | Persistent cystic duct obstruction → inflammation |
| Choledocholithiasis | Stone passage into CBD → obstructive jaundice, cholangitis |
| Ascending cholangitis | CBD obstruction + infection (Charcot's triad: fever, jaundice, RUQ pain) |
| Gallstone pancreatitis | Stone at ampulla of Vater |
| Gallstone ileus | Erosion of large stone through gallbladder into duodenum → small bowel obstruction (Rigler's triad: SBO + pneumobilia + ectopic mineral shadow) |
| Mucocele/empyema | Continued mucus secretion in obstructed gallbladder |
| Gallbladder carcinoma | Chronic irritation (increased risk with large stones >3 cm and porcelain gallbladder) |
Diagnosis
Investigations
- Abdominal ultrasound - first-line investigation; sensitivity and specificity >90%. Findings: echogenic foci with posterior acoustic shadowing that move with gravity. Also shows gallbladder wall thickening, pericholecystic fluid (in cholecystitis), and biliary sludge.
- Labs: Usually normal in uncomplicated cholelithiasis. In cholecystitis: leukocytosis ± bandemia. In choledocholithiasis: elevated ALP, bilirubin, transaminases; elevated amylase/lipase if pancreatitis.
- CT scan: Less sensitive for cholesterol stones (radiolucent) but detects complications; good for pigment/calcified stones
- MRCP (Magnetic Resonance Cholangiopancreatography): Gold standard for CBD stones (choledocholithiasis)
- HIDA scan (hepatobiliary scintigraphy): Useful when USS equivocal; non-filling of gallbladder suggests acute cholecystitis
- ERCP: Diagnostic and therapeutic for choledocholithiasis
Management
Asymptomatic Cholelithiasis
- Observation/expectant management is the standard recommendation
- Prophylactic cholecystectomy is generally not indicated, except in:
- Patients undergoing bariatric surgery (especially malabsorptive procedures or RYGB with symptomatic disease)
- High-risk populations (Native Americans, where gallbladder cancer risk is elevated)
- Porcelain gallbladder with mucosal irregularities
- Large stones >3 cm (cancer risk)
- Ursodiol (ursodeoxycholic acid) 300 mg BID is used for 6 months after bariatric surgery to prevent gallstone formation from rapid weight loss; reduces incidence from ~30% to ~4%
Symptomatic Cholelithiasis - Definitive Treatment
- Laparoscopic cholecystectomy is the gold standard
- Benefits: shorter hospital stay, faster recovery, reduced morbidity vs. open
- Performed electively for biliary colic; urgently/emergently for acute cholecystitis/complications
Choledocholithiasis
- ERCP with sphincterotomy and stone extraction, followed by laparoscopic cholecystectomy
Special Populations
Pregnancy:
- Surgical intervention is the primary treatment for symptomatic gallstones in pregnancy
- Laparoscopic cholecystectomy during pregnancy is preferred over open (lower fetal, maternal, and surgical complication rates)
- Best performed in the 1st or 2nd trimester (not the 3rd trimester when the uterus impairs access)
- Gallstone pancreatitis in pregnancy carries: maternal mortality 15%, fetal mortality 60% - justifies aggressive surgical management
- Recurrence of symptoms if left untreated: 92% (1st trimester), 64% (2nd trimester), 44% (3rd trimester)
Gallstone Ileus (Special Complication)
A large gallstone erodes through the gallbladder wall into the duodenum (cholecystenteric fistula) and impacts in the small bowel, classically ~60 cm proximal to the ileocaecal valve. Occurs predominantly in the elderly.
Rigler's Triad (on plain X-ray/CT):
- Small bowel obstruction
- Pneumobilia (air in biliary tree)
- Ectopic calcified stone shadow
Presence of 2 of 3 signs is considered pathognomonic (seen in 40-50% of cases). Management: milk the stone proximally and perform enterolithotomy; do not explore the gallbladder fistula at the initial operation.
Recent Evidence Note
A 2024 global epidemiology meta-analysis (Wang et al., PMID 38382725) provides updated prevalence data on gallstones in the 21st century. Additionally, recent meta-analyses (2025) on GLP-1 receptor agonists (e.g., semaglutide, tirzepatide) note an increased risk of gallstone formation as a gastrointestinal adverse effect (PMIDs 40189856, 40499738) - relevant to the growing use of these agents in obesity management.
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 811-812 | Sabiston Textbook of Surgery | Sleisenger and Fordtran's Gastrointestinal and Liver Disease | Textbook of Family Medicine 9e, p. 1131 | Maingot's Abdominal Operations | Bailey and Love's Short Practice of Surgery 28th Edition
This is a shared conversation. Sign in to Orris to start your own chat.