Abg analysis
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
Reading File
Now I have comprehensive content. Here is a complete, structured guide to ABG analysis:
Arterial Blood Gas (ABG) Analysis
Normal Values
| Parameter | Normal Range |
|---|---|
| pH | 7.35 - 7.45 |
| PaCO2 | 35 - 45 mmHg |
| HCO3- | 22 - 26 mEq/L |
| PaO2 | 70 - 100 mmHg (age-dependent) |
| SaO2 | >95% |
| Base Excess | -2 to +2 mEq/L |
Henderson-Hasselbalch equation: pH = 6.1 + log10 ([HCO3-] / 0.003 x PaCO2)
Normal age-adjusted PaO2 (sitting): 104.2 - (0.27 x age in years)
Step-by-Step Interpretation
Step 1 - Determine pH Status
- pH < 7.35 = Acidemia
- pH > 7.45 = Alkalemia
- pH 7.35-7.45 = Normal (but a disorder may still exist - compensated or mixed)
Acidemia and alkalemia describe the blood's pH. Acidosis and alkalosis describe the underlying processes. Multiple acid-base disorders can coexist simultaneously.
Step 2 - Identify the Primary Disorder
| Primary Disorder | pH | PaCO2 | HCO3- |
|---|---|---|---|
| Respiratory Acidosis | ↓ | ↑ (>45) | Normal/↑ |
| Respiratory Alkalosis | ↑ | ↓ (<35) | Normal/↓ |
| Metabolic Acidosis | ↓ | Normal/↓ | ↓ (<22) |
| Metabolic Alkalosis | ↑ | Normal/↑ | ↑ (>26) |
Key rule: If pH < 7.35 and PaCO2 is elevated - primary respiratory acidosis. If pH < 7.35 and HCO3- is low - primary metabolic acidosis.
Step 3 - Assess Compensation
Compensation is never complete. It reduces the pH change but does not return it fully to normal.
| Primary Disorder | Compensatory Response | Formula |
|---|---|---|
| Metabolic acidosis | Hyperventilation (↓ PaCO2) | Expected PaCO2 = 1.5 x [HCO3-] + 8 ± 2 (Winter's formula) |
| Metabolic alkalosis | Hypoventilation (↑ PaCO2) | Expected PaCO2 increase = 0.6 x rise in HCO3- |
| Respiratory acidosis - Acute | Renal HCO3- retention | HCO3- rises by 1 mEq/L per 10 mmHg ↑ PaCO2 |
| Respiratory acidosis - Chronic | Renal HCO3- retention | HCO3- rises by 4 mEq/L per 10 mmHg ↑ PaCO2 |
| Respiratory alkalosis - Acute | Renal HCO3- excretion | HCO3- drops by 2 mEq/L per 10 mmHg ↓ PaCO2 |
| Respiratory alkalosis - Chronic | Renal HCO3- excretion | HCO3- drops by 5 mEq/L per 10 mmHg ↓ PaCO2 |
Metabolic compensation (renal) takes 3-5 days. Respiratory compensation is rapid (hours).
If measured compensation does not match predicted, a second primary disorder is present.
Rule of 15 (quick check for metabolic acidosis): Expected PaCO2 ≈ HCO3- + 15. Also, if HCO3- < 10, expected PaCO2 ≈ 15 mmHg (±2).
Step 4 - Calculate the Anion Gap (if metabolic acidosis present)
AG = Na+ - (Cl- + HCO3-)
- Normal: 9-15 mEq/L (threshold of 15 often used)
- Corrected AG (for hypoalbuminemia): Add 2.5 mEq/L for every 1 g/dL drop in albumin below 4 g/dL
Wide (High) AG Acidosis - Mnemonic: MUDPILES
- M - Methanol
- U - Uremia
- D - DKA (Diabetic Ketoacidosis)
- P - Paraldehyde / Propylene glycol / Paracetamol (Acetaminophen)
- I - Iron / Isoniazid
- L - Lactic acidosis
- E - Ethylene glycol
- S - Salicylates
Normal AG (Non-Anion Gap) Acidosis - Mnemonic: HARDUP
- H - Hyperalimentation / Hospital saline
- A - Acid infusion / Addison's disease / Acetazolamide
- R - Renal Tubular Acidosis (RTA)
- D - Diarrhea
- U - Ureterosigmoidostomy
- P - Pancreatic fistula / drainage
Step 5 - Delta Gap (in Wide AG Acidosis)
Used to detect a concurrent metabolic alkalosis or normal-AG acidosis hiding behind a wide-AG acidosis.
Delta Gap = (Measured AG - 15) vs (24 - Measured HCO3-)
- If delta AG > delta HCO3- : Concurrent metabolic alkalosis
- If delta AG < delta HCO3- : Concurrent normal-AG (hyperchloremic) acidosis
- If delta AG ≈ delta HCO3- : Pure wide-AG acidosis
Step 6 - Assess Oxygenation
A-a Gradient = FiO2 x (PB - PH2O) - (PaO2 + PaCO2 / 0.8)
- Simplified normal: P(A-a)O2 = (Age/4) + 4
Mechanisms of hypoxemia:
| Mechanism | A-a Gradient | Example |
|---|---|---|
| V/Q mismatch | Increased | Pneumonia, PE |
| Diffusion impairment | Increased | Interstitial lung disease |
| Right-to-left shunt | Increased | AV malformation |
| Hypoventilation | Normal | Neuromuscular weakness |
| Low FiO2 / altitude | Normal | High altitude |
| Hepatopulmonary syndrome | Increased | Cirrhosis |
Step 7 - Osmolar Gap (if toxic ingestion suspected)
Calculated osmolarity = (2 x Na) + (Glucose/18) + (BUN/2.8) + (Ethanol/3.7)
Osmolar gap = Measured osmolality - Calculated osmolarity
- Normal: <10 mOsm/kg
- Gap >10 suggests unmeasured osmoles (methanol, ethylene glycol, isopropanol)
Acid-Base Map
The following map plots pH vs PaCO2 with confidence bands for each pure disorder:
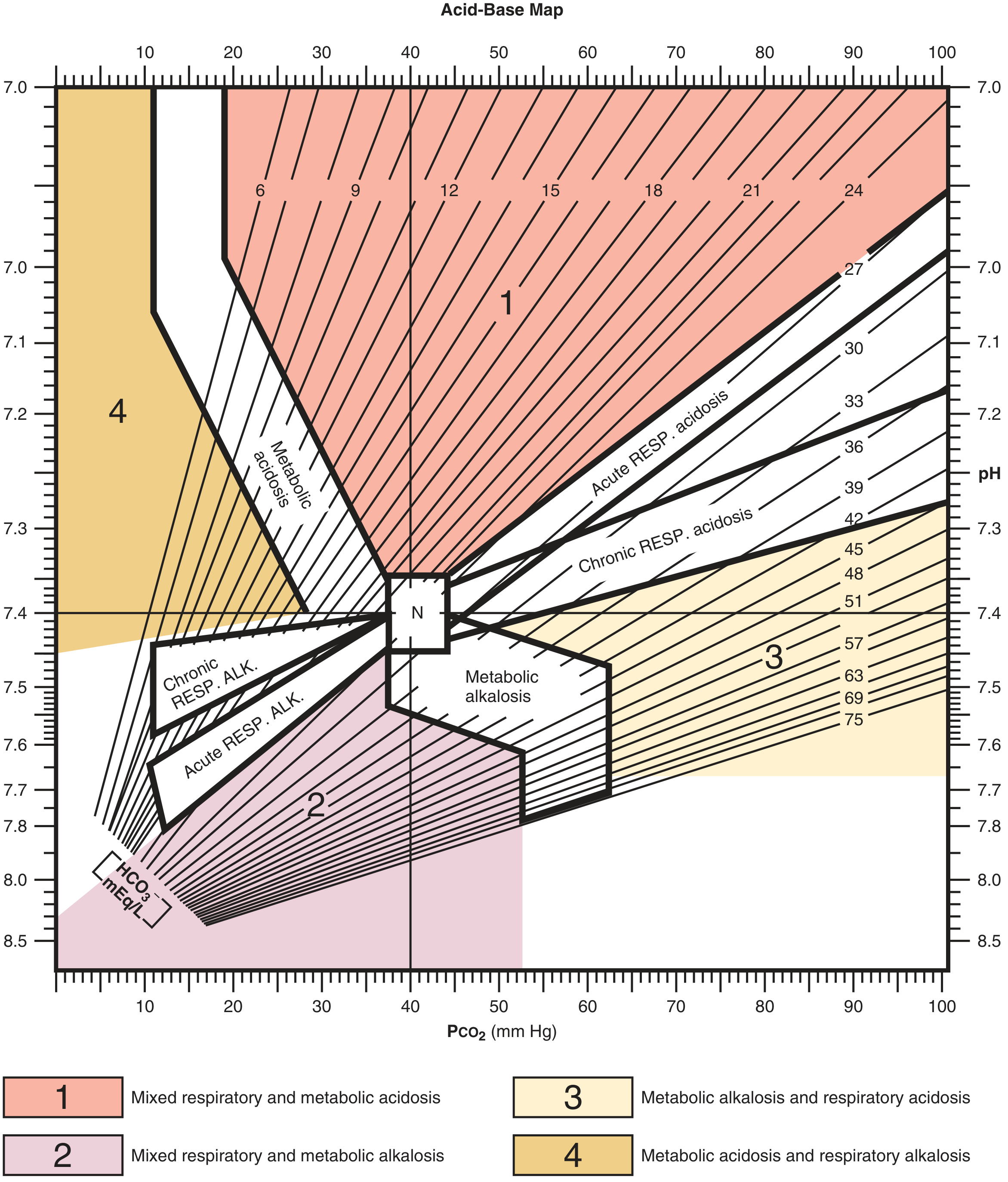
Points falling outside the confidence bands = mixed disorders. The four mixed zones are:
- Mixed respiratory + metabolic acidosis
- Mixed respiratory + metabolic alkalosis
- Metabolic alkalosis + respiratory acidosis
- Metabolic acidosis + respiratory alkalosis
Venous Blood Gas (VBG) vs ABG
- Venous pH is ~0.03 units lower than arterial
- PvCO2 is 3-8 mmHg higher than PaCO2 (less reliable for CO2 comparison)
- VBG is unreliable in hypotensive patients and severe hypercapnia
- A normal PvCO2 can effectively rule out hypercapnia
Worked Examples
Example 1: Metabolic acidosis with respiratory compensation
- pH 7.26, PaCO2 13 mmHg, HCO3- 5 mEq/L
- Step 1: Acidemia (pH < 7.35)
- Step 2: Primary metabolic acidosis (HCO3- low, PaCO2 not elevated)
- Step 3: Winter's formula: Expected PaCO2 = (1.5 x 5) + 8 = 15.5 ± 2. Measured = 13 mmHg - appropriate compensation, no additional respiratory disorder
Example 2: Respiratory alkalosis (sepsis)
- pH 7.49, PaCO2 25 mmHg, HCO3- 22 mEq/L
- Step 1: Alkalemia
- Step 2: Primary respiratory alkalosis (PaCO2 low, HCO3- not elevated)
- Step 3: Expected HCO3- drop = 2 mEq/L per 10 mmHg PaCO2 decrease = 3 mEq/L drop. Actual drop ≈ 2. Consistent with pure respiratory alkalosis - sepsis-driven hyperventilation
Sources: Goldman-Cecil Medicine, p. 1040 | Roberts and Hedges' Clinical Procedures in Emergency Medicine | Rosen's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.