Allergic fungal rhinosinusitits
Reading File
Finding Sources
Finding Sources
Searching PubMed
"allergic fungal rhinosinusitis" AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive content from multiple authoritative sources. Let me compile the full answer.
Allergic Fungal Rhinosinusitis (AFRS)
Overview
AFRS is a non-invasive, immunologically mediated form of chronic rhinosinusitis (CRS) affecting immunocompetent, atopic individuals. It accounts for 5-10% of all CRS cases requiring surgery and is characterized by an exaggerated IgE-mediated hypersensitivity to ubiquitous airborne fungi. The disease was first reported by Safirstein in 1976, who noted its histopathologic resemblance to allergic bronchopulmonary aspergillosis (ABPA). - K.J. Lee's Essential Otolaryngology, p. 559
Epidemiology
- Most common in young immunocompetent adults (mean age 21-33 years)
- Predilection for warm, humid geographic regions (e.g., the Mississippi basin in the USA, tropical regions)
- Strongly associated with lower socioeconomic status and atopic background
- Comorbid asthma is common; aspirin-sensitive asthma suggests eosinophilic mucin rhinosinusitis (EMRS) rather than classic AFRS
- Scott-Brown's Otorhinolaryngology, Vol 1, p. 260
Pathophysiology
The underlying mechanism is a Type I (IgE-mediated) hypersensitivity reaction to inhaled fungal antigens, with a possible contributory Type III (immune complex) component:
- Inhaled fungal spores (particularly dematiaceous fungi) are encountered by an atopic sinonasal mucosa
- Fungal antigens drive IgE-mediated mast cell and eosinophil activation
- This creates an inflammatory cascade involving IL-25, IL-33, and TSLP (Th2 epithelial cytokines), eosinophil recruitment, and mucus stasis
- Ostial obstruction leads to accumulation of eosinophilic (allergic) mucin containing fungal debris
- The expanding mucin mass causes sinus expansion, bony demineralization, remodeling, and erosion - without mucosal invasion
- Secondary Staphylococcus aureus biofilm may co-exist, with superantigens amplifying the eosinophilic response
Key causative fungi:
-
Dematiaceous (pigmented) species: Bipolaris, Curvularia, Alternaria, Exophiala, Fusarium
-
Aspergillus species (less common, more typical in hot dry climates)
-
K.J. Lee's Essential Otolaryngology, p. 559-560
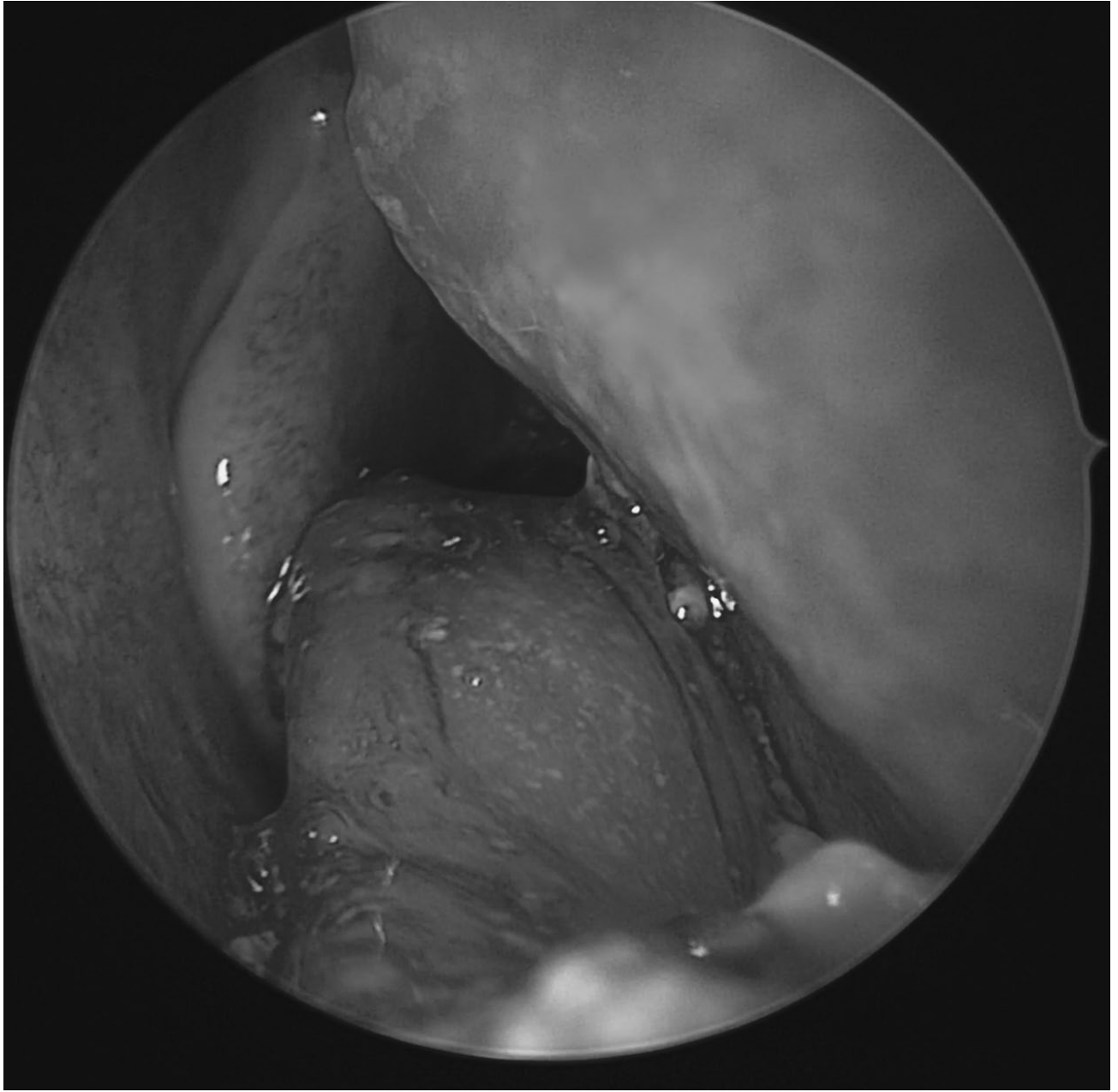
Allergic Mucin (Eosinophilic Mucin)
The hallmark of AFRS is allergic (eosinophilic) mucin (EM), characterized by:
- Gross appearance: Thick, viscous, greenish-brown, "peanut butter" consistency
- Histology:
- Lamellated sheets of eosinophils
- Charcot-Leyden crystals (bipyramidal crystals from eosinophil breakdown)
- Branching, non-invasive fungal hyphae (may be sparse or absent)
- Necrotic inflammatory cell debris
Endoscopic view of characteristic thick eosinophilic mucin in AFRS:
Clinical Presentation
| Feature | Description |
|---|---|
| Onset | Insidious, slow progression over months to years |
| Nasal symptoms | Obstruction, nasal polyps, mucopurulent discharge |
| Systemic atopy | Allergic rhinitis, asthma, eczema |
| Olfaction | Hyposmia or anosmia |
| Advanced disease | Proptosis, diplopia, facial deformity from bony expansion |
| Discharge character | Greenish-brown, thick, tenacious mucus |
In children, proptosis may be the presenting complaint due to orbital expansion by the enlarging mucin mass. - Scott-Brown's Vol 2, p. 462
Diagnostic Criteria: Bent and Kuhn (1994)
All 5 major criteria must be fulfilled for diagnosis. Minor criteria support it:
| Major Criteria | Minor Criteria |
|---|---|
| Type I hypersensitivity to fungi (skin testing or in vitro IgE) | Asthma |
| Nasal polyposis | Unilateral disease |
| Characteristic CT findings | Radiological bone erosion |
| Eosinophilic mucin WITHOUT fungal invasion | Positive fungal cultures |
| Positive fungal stain/smear | Serum eosinophilia |
| Charcot-Leyden crystals |
deShazo's revised criteria (1997): CT-confirmed sinusitis + allergic mucin + fungal hyphae within mucin + absence of invasion + absence of diabetes/immunodeficiency.
2004 Expert Panel: Histological confirmation of eosinophilic mucin + Type I hypersensitivity to fungi in CRS patients. - Scott-Brown's Vol 1, p. 260
Imaging
CT Scan (modality of choice - non-contrast)
Coronal CT showing bilateral sinus opacification with heterogeneous attenuation (high-density eosinophilic mucin) in AFRS:

Classic "double density sign" on coronal CT - central hyperdensity from eosinophilic mucin surrounded by peripheral mucosal thickening:
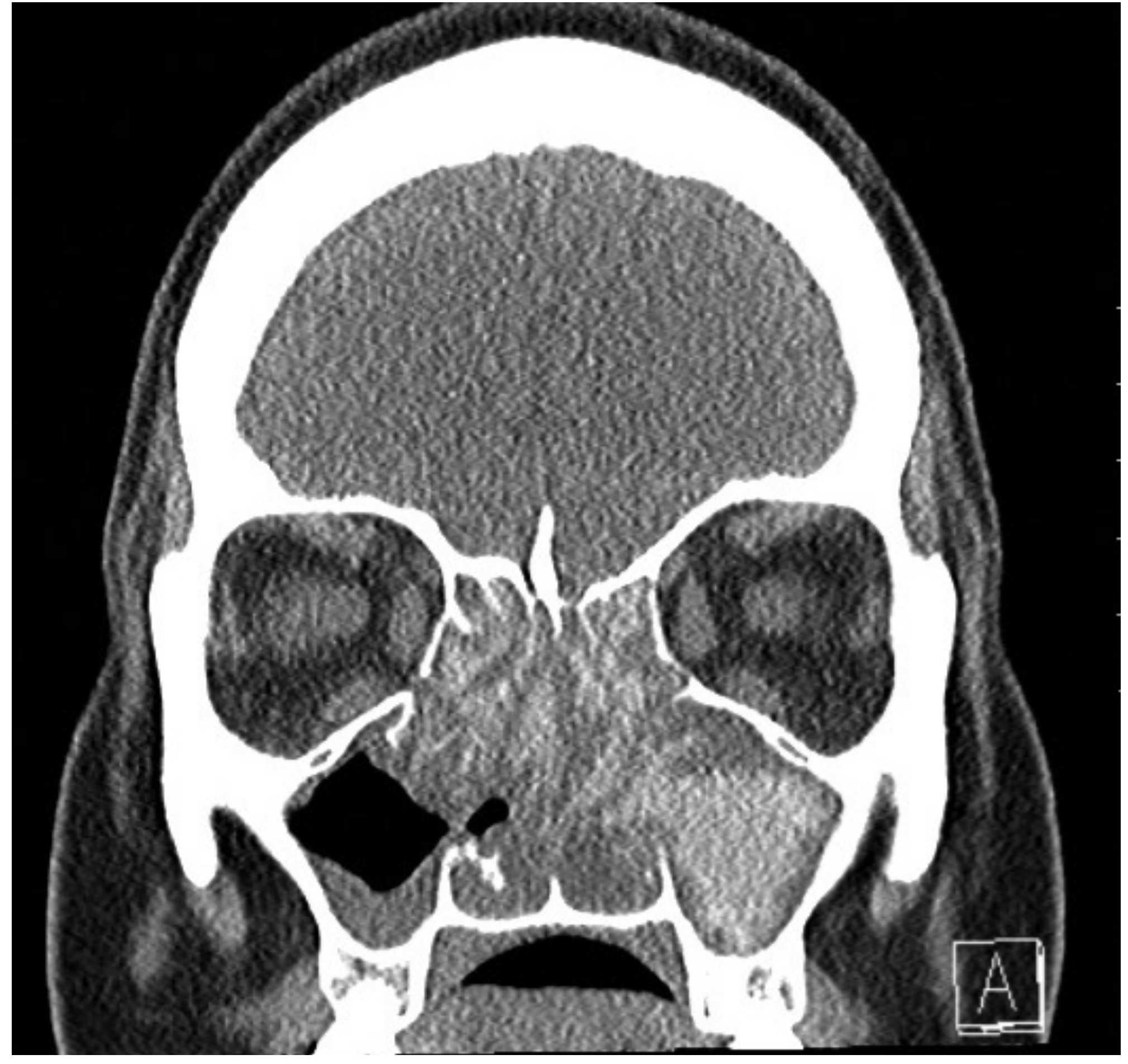
CT findings:
- Ethmoid sinuses most commonly involved
- Heterogeneous, increased attenuation of sinus contents (due to calcium salts, heavy metals, protein concentration in mucin)
- Sinus expansion with bony demineralization, remodeling, or frank erosion
- Can be unilateral or bilateral (unilateral is more classic; bilateral suggests EMRS)
- Erosion of lamina papyracea, skull base possible in advanced disease
MRI
-
T1: isointense to hypointense (high protein, dehydrated mucin)
-
T2: hypointense to signal void (classic finding - helps distinguish from bacterial sinusitis)
-
Peripheral mucosal enhancement with contrast; allergic mucin does NOT enhance
-
K.J. Lee's Essential Otolaryngology, p. 561
Spectrum of Disease / Related Entities
| Condition | Fungus | IgE | Systemic IgE | Notes |
|---|---|---|---|---|
| Classic AFRS | Present | Elevated (specific + total) | Elevated | All Bent & Kuhn criteria met |
| Eosinophilic Mucin Rhinosinusitis (EMRS) | Absent | Elevated (non-specific) | Elevated but less | Bilateral; associated with aspirin-sensitive asthma; IgG1 deficiency |
| Non-allergic Eosinophilic FRS (EFRS) | Present | Absent systemically | Local IgE elevated | No Type I hypersensitivity; MBP-mediated epithelial damage |
Eosinophilic inflammation is the central unifying theme across this spectrum. - K.J. Lee's Essential Otolaryngology, p. 560
Treatment
AFRS is notorious for high recidivism and resistance to conventional therapy. The standard of care combines surgery with prolonged medical management.
1. Surgery - Endoscopic Sinus Surgery (ESS)
ESS is the cornerstone of treatment:
- Goals: Complete removal of allergic mucin and fungal debris, polypectomy, meticulous ethmoidectomy, wide ostioplasty
- Thorough debridement is essential - residual mucin perpetuates the inflammatory response and drives revision surgery
- Caution: Significant bony erosion means dura and periorbita may be adherent to mucosa and easily violated
- Micro-debriders should be used with extreme care near areas of orbital or skull base dehiscence
- Balloon sinusotomy is controversial in severe AFRS/polyposis disease; use is more appropriate for mild-moderate disease
2. Corticosteroids
Post-operative steroids are recommended (Grade B evidence):
Systemic:
- Prednisone ~0.5 mg/kg/day for 2-3 weeks, perioperative, then tapered over several days to weeks
- Reduces post-operative mucosal disease and inflammatory markers
- Risk: significant side effects with high-dose prolonged use; disease may recur on cessation
Topical:
- Intranasal steroid sprays or budesonide irrigations - used concomitantly and long-term
- Tapered after stabilization of mucosal health
3. Immunotherapy (IT)
Level C evidence supports IT with fungal allergens (dematiaceous species):
- Decreases polyp recurrence, nasal crusting, systemic corticosteroid use
- Reduces revision surgery rates (11.1% with IT vs. 33% without IT in one study - Bassichis et al.)
- Concern about theoretical Type III (immune complex) reaction from fungal-specific IgG has not been substantiated - no such reactions reported to date
- IT may begin post-operatively once surgical sites have healed
4. Antifungals
- Sparse evidence; Cochrane reviews of both topical and oral antifungals show no benefit in CRS
- Oral or topical antifungals are NOT recommended as routine therapy in AFRS
- K.J. Lee's Essential Otolaryngology, p. 562
5. Biologics (Emerging - 2025 Evidence)
A recent 2025 systematic review and meta-analysis (PMID 40552669) demonstrates short-term efficacy of biologics in recalcitrant AFRS. Omalizumab (anti-IgE) has shown promise in AFRS refractory to surgery and conventional medical therapy, consistent with the central IgE-mediated pathophysiology. - Scott-Brown's Vol 1, p. 261
6. Antibiotics
- Culture-directed antibiotics for frank mucopurulence
- AFRS exacerbations are often heralded by secondary acute bacterial sinus infections
- Some clinicians use empirical anti-staphylococcal agents or mupirocin irrigation post-operatively (given the S. aureus biofilm association)
7. Leukotriene Modulators
- No established evidence to support montelukast in AFRS (only one case report of benefit)
Post-operative Surveillance
Prolonged endoscopic follow-up is mandatory given the high recidivism rate. Serial endoscopy allows:
-
Early detection of disease recurrence
-
Surveillance for new bone erosion
-
Guided topical medication delivery into widely patent sinuses
-
Timely initiation of revision surgery if needed
-
Cummings Otolaryngology, Head and Neck Surgery, p. 892
Key Differentials
| Feature | AFRS | Fungal Ball | Invasive FRS |
|---|---|---|---|
| Immunity | Immunocompetent, atopic | Immunocompetent | Immunocompromised |
| Invasion | None | None | Yes - vascular/tissue |
| IgE | Elevated | Normal | Normal |
| Eosinophilic mucin | Yes | No | No |
| Treatment | ESS + steroids + IT | ESS only | ESS + systemic antifungals + treat underlying cause |
| Prognosis | Recurrent; not lethal | Excellent | Grave |
Recent Evidence Update
- A 2025 meta-analysis (PMID 40552669) confirms short-term biologic efficacy (particularly omalizumab and dupilumab) in recalcitrant AFRS.
- A 2026 systematic review (PMID 42061107) characterizes AFRS fungal species distribution in the Eastern Mediterranean, where Aspergillus and dematiaceous fungi both feature prominently.
- A 2025 meta-analysis on post-operative oral corticosteroids (PMID 40270102) reinforces the benefit of perioperative steroid use in CRS/AFRS following ESS.
Sources:
- K.J. Lee's Essential Otolaryngology, 12th Ed., pp. 559-562
- Cummings Otolaryngology Head and Neck Surgery, 7th Ed., pp. 876, 892
- Scott-Brown's Otorhinolaryngology, Vol 1, pp. 259-261
- Harrison's Principles of Internal Medicine, 22E (2025), p. 300
This is a shared conversation. Sign in to Orris to start your own chat.