Dysphagia more common in which side of stroke?
Reading File
Searching PubMed
dysphagia stroke laterality hemisphere
Finding Sources
Searching PubMed
dysphagia stroke hemisphere laterality
Reading File
Reading File
Here is a complete, textbook-sourced answer:
Dysphagia After Stroke - Laterality
The Short Answer
Neither side is exclusively "more common" in terms of incidence - dysphagia can follow stroke in either hemisphere. However, right hemisphere strokes tend to produce more severe pharyngeal-phase dysphagia, while left hemisphere strokes more prominently affect the oral stage. The key teaching point is that bilateral hemispheric damage produces the most consistent and severe dysphagia.
What the Textbooks Say
Bradley & Daroff's Neurology in Clinical Practice states directly:
"Strokes involving the right hemisphere tend to produce more impairment of pharyngeal motility, whereas left hemispheric lesions have a greater effect on oral stage function."
This means:
- Right hemisphere stroke - impairs the pharyngeal phase (involuntary, reflexive component of swallowing)
- Left hemisphere stroke - impairs the oral phase (voluntary, preparatory component)
Why This Happens: The Bihemispheric Representation Model
Swallowing has bilateral cortical representation, but the two hemispheres are not equal - one is typically the "swallowing-dominant" hemisphere for each individual (not always the language-dominant side). Key points:
- After unilateral stroke, dysphagia depends on whether the stroke hit the dominant swallowing hemisphere
- Recovery depends on cortical reorganization in the contralesional (unaffected) hemisphere - patients who recover well show greater pharyngeal cortical representation in the unaffected hemisphere (Hamdy et al., confirmed in Adams & Victor)
- Dysphagic patients post-stroke have a smaller pharyngeal representation in the unaffected hemisphere - meaning there is less "reserve" to compensate
Where Dysphagia is Most Severe
| Stroke Location | Dysphagia Features |
|---|---|
| Right hemisphere | Pharyngeal motility impairment; more clinically significant |
| Left hemisphere | Oral stage dysfunction (tongue, bolus preparation) |
| Bilateral hemispheric | Severe, persistent dysphagia (pseudobulbar pattern) |
| Lateral medullary (Wallenberg) | ~50-55% incidence; pharyngeal phase severely affected |
| Subcortical strokes | >85% show delayed pharyngeal initiation; 75% have aspiration |
Important Caveats
- The common belief that dysphagia = brainstem stroke is a myth - it is well documented in cortical and subcortical hemispheric strokes too
- Dysphagia occurs in roughly 50% of all acute strokes in the first few days, on either side
- Subcortical strokes (internal capsule, basal ganglia) carry a higher incidence of dysphagia and aspiration than cortical ones
- Bilateral frontoparietal opercular damage causes Foix-Chavany-Marie syndrome - complete loss of volitional facial/tongue/pharyngeal movement with preserved involuntary movements
Bottom Line for Exams
Right hemisphere stroke = more pharyngeal phase dysphagia (the "clinically relevant" swallowing dysfunction causing aspiration risk). However, the most complete answer is that swallowing has bilateral cortical representation, and the severity depends on which hemisphere is the individual's swallowing-dominant hemisphere.
Sources: Bradley & Daroff's Neurology in Clinical Practice; Adams & Victor's Principles of Neurology, 12th Ed.
Type of respiratory pattern in stroke
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Here is the complete, textbook-based answer with the classic diagram:
Respiratory Patterns in Stroke - Localization Guide
The pattern of abnormal breathing is one of the most reliable clinical tools for localizing the level of a CNS lesion in stroke. Each pattern corresponds to damage at a specific neuroanatomical level.
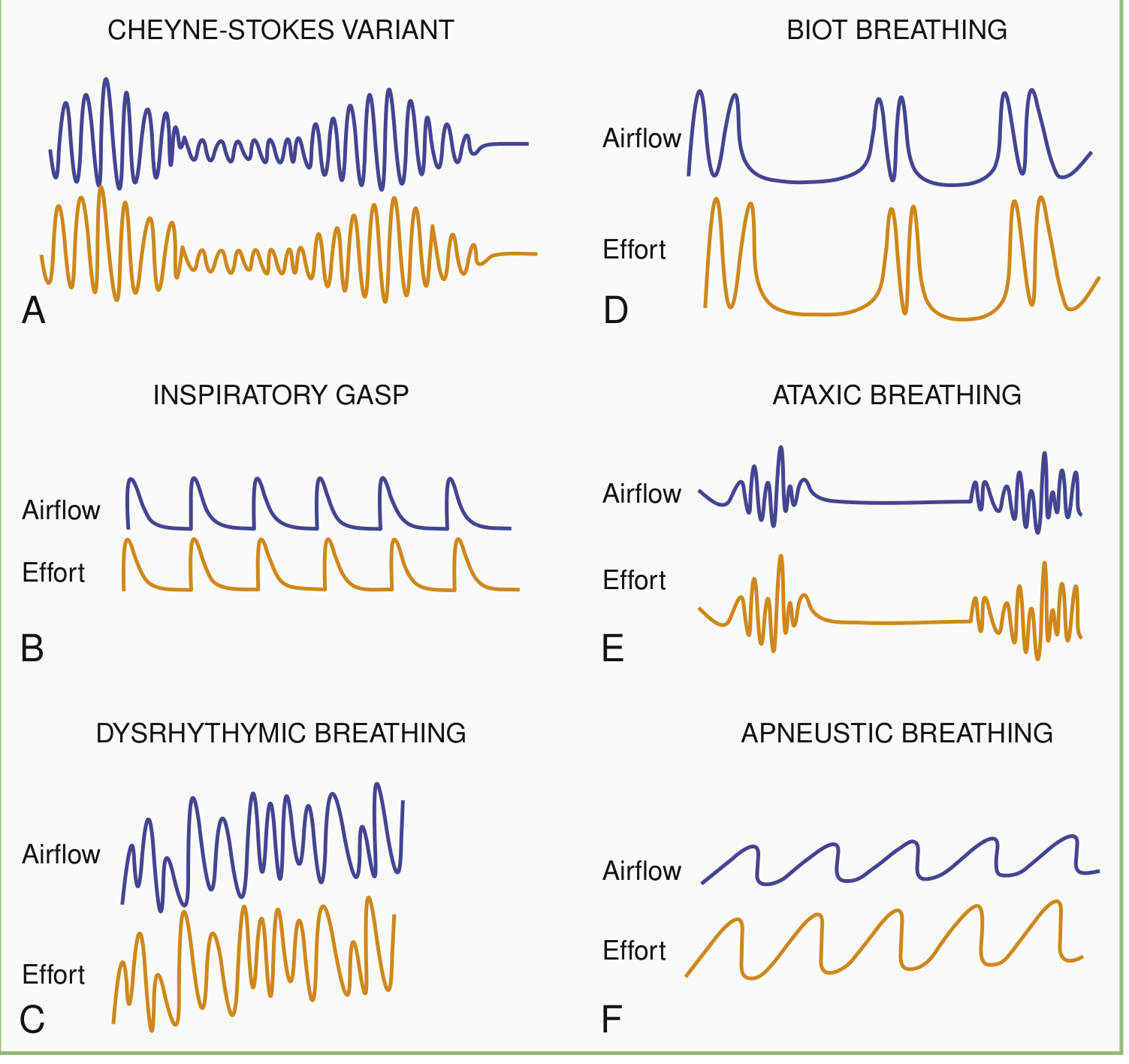
1. Cheyne-Stokes Respiration
Location: Bilateral hemispheric or diencephalic lesions
- Breathing slowly oscillates between hyperventilation and hypoventilation, with periods of apnea
- Classic crescendo-decrescendo pattern cycling roughly every 45-60 seconds
- Caused by bilateral lesions anywhere along the descending pathway from forebrain to upper pons
- Patients are more alert during the waxing phase and less alert during apnea
- A relatively good prognostic sign - implies no permanent brainstem damage
- Also seen in cardiac failure (prolonged circulation time)
- Warning: emergence in a patient with a unilateral mass lesion = early sign of herniation
2. Central Neurogenic Hyperventilation
Location: Central tegmental pontine lesions - just ventral to the aqueduct of Sylvius or 4th ventricle (low midbrain / upper pons)
- Sustained rapid breathing at 40-70 breaths/min
- Rare - must be distinguished from reactive hyperventilation from hypoxia or metabolic acidosis
- Large CNS lesions can cause neurogenic pulmonary edema with secondary hypoxemia that mimics this
3. Apneustic Breathing
Location: Dorsolateral tegmental lesion of the middle/caudal pons
- Prolonged inspiratory gasp with a pause at full inspiration (2-3 second hold)
- Caused by lesions of the medial parabrachial/Kolliker-Fuse area of the rostral pons
- Indicates pontine level damage
4. Cluster (Short-cycle Periodic) Breathing
Location: Lower pontine tegmental / high medullary lesions
- Periodic respirations irregular in frequency and amplitude, with variable pauses between clusters
- Short cycle (faster than Cheyne-Stokes), bursts of 7-10 rapid breaths then apnea, without waxing-waning prodrome
- Also seen with increased ICP and posterior fossa expanding lesions
5. Ataxic (Biot's) Breathing
Location: Dorsomedial reticular formation of the medulla
- Completely irregular in both rate and rhythm - chaotic breathing
- Combination of ataxic respiration + bilateral 6th nerve palsy = warning sign of brainstem compression from posterior fossa expanding lesion
- Pre-terminal pattern - indicates severe lower brainstem damage
- Can progress abruptly to respiratory arrest
Summary Table
| Pattern | Location of Lesion | Key Feature |
|---|---|---|
| Cheyne-Stokes | Bilateral hemispheres / diencephalon | Crescendo-decrescendo + apnea |
| Central neurogenic hyperventilation | Low midbrain / upper pons | 40-70 breaths/min, sustained |
| Apneustic | Mid/caudal pons (dorsolateral) | Inspiratory pause at full inspiration |
| Cluster | Lower pons / upper medulla | Irregular bursts with variable pauses |
| Ataxic (Biot's) | Medulla (dorsomedial) | Completely chaotic - pre-terminal |
Important Points
- Progression from Cheyne-Stokes → central hyperventilation → apneustic → ataxic reflects rostrocaudal deterioration (transtentorial herniation progressing downward) - an ominous sign
- Medullary stroke (e.g., lateral medullary/Wallenberg) can cause respiratory arrest and death due to disruption of the automatic respiratory centers
- Subcortical/locked-in syndrome (midpontine stroke): automatic breathing preserved but voluntary breathing lost (can't voluntarily hyperventilate on command)
- Brainstem infarctions are the most life-threatening in terms of respiratory compromise
Sources: Bradley & Daroff's Neurology in Clinical Practice; Neuroanatomy Through Clinical Cases, 3rd Ed.; Murray & Nadel's Textbook of Respiratory Medicine
This is a shared conversation. Sign in to Orris to start your own chat.