Trans sphenoida approach to
Trans sphenoida approach to Anterior skull base
Reading File
Finding Sources
Finding Sources
Searching PubMed
transsphenoidal approach anterior skull base endoscopic
Finding Sources
Finding Sources
Searching PubMed
endoscopic endonasal anterior skull base
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have enough comprehensive content to provide a thorough answer. Here is the complete overview:
Transsphenoidal Approach to the Anterior Skull Base
The transsphenoidal approach has evolved from a narrow pituitary-only corridor into a family of extended endonasal approaches (EEA) that can reach virtually the entire ventral skull base - from the cribriform plate anteriorly to the foramen magnum posteriorly. For the anterior skull base specifically, the three key sub-approaches are:
- Transcribriform approach
- Transtuberculum-transplanum approach
- Classic transsphenoidal (transsellar/parasellar)
Endoscopic View After Sphenoidectomy
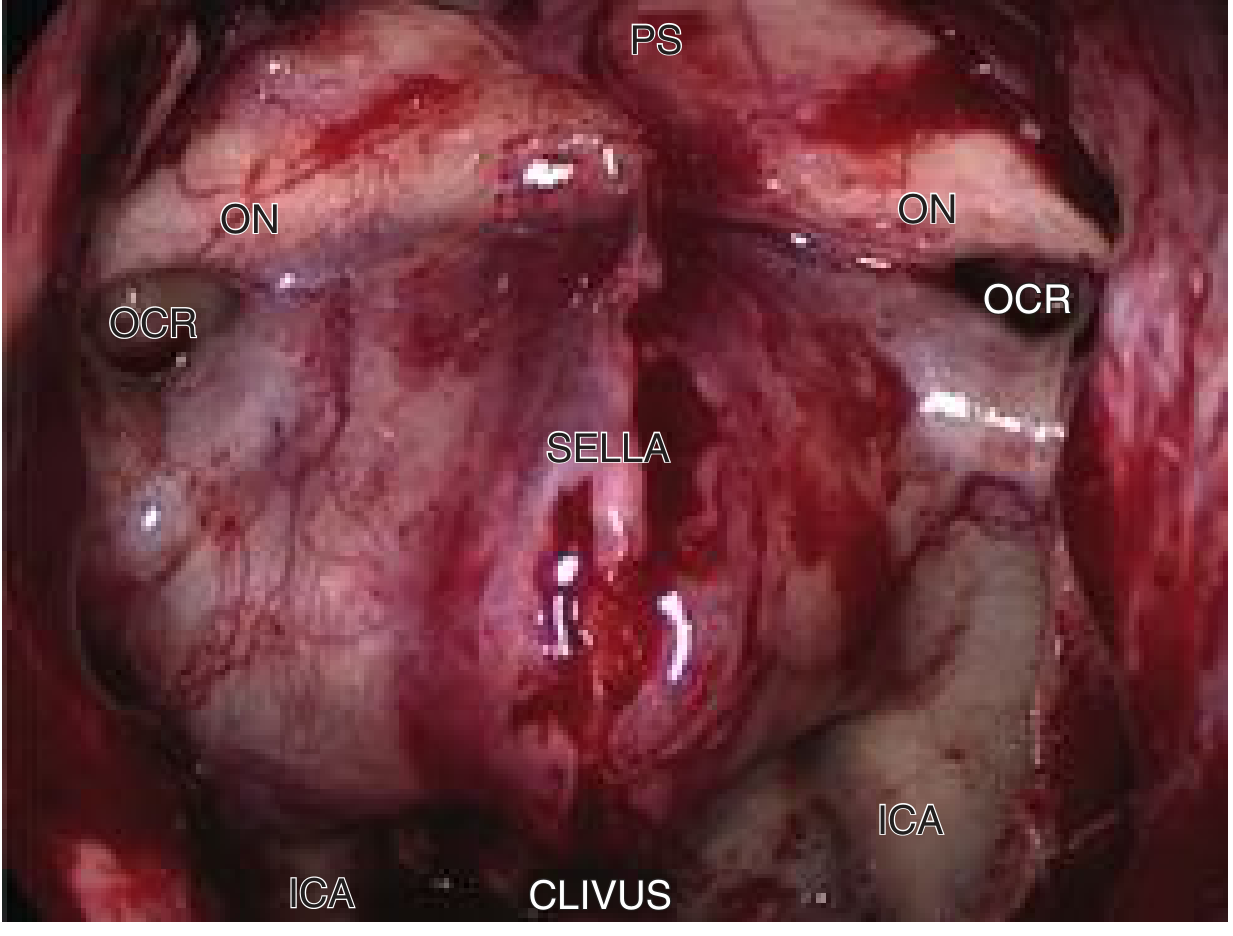
Endoscopic view of the posterior wall of the sphenoid sinus after intersinus septum resection. Identifies bilateral ICAs, optic nerves (ON), optic-carotid recesses (OCR), planum sphenoidale (PS), sella, and clivus - the anatomical landmarks for all transsphenoidal anterior skull base work.
Nasal Access Routes
Regardless of which anterior skull base target is chosen, the initial nasal corridor is established by one of four routes:
| Route | Description | Best Used For |
|---|---|---|
| Direct transnasal | Single nostril; superior turbinate removed if needed | Roof of nasal cavity lesions, some sphenoid sinus lesions |
| Transseptal | Hemitransfixion incision; septum mobilized midline | Sella, pituitary adenomas |
| Transseptal-transnasal (binostril) | Two surgeons, four-handed; septal flap without perforation | Extended approaches |
| Transethmoidal | Adds ethmoidectomy; middle turbinate removed | Ethmoidal lesions, combined ethmoid-sphenoid disease |
In all extended approaches, the first and most critical step is raising a large pedicled nasoseptal flap (Hadad-Bassagasteguy flap) based on the vascular pedicle of the sphenopalatine foramen - this is preserved for skull base reconstruction at closure.
Sphenoidectomy - Common Foundation
All anterior skull base transsphenoidal approaches begin with a wide sphenoidotomy:
- The ostium is probed and opened with a micro-Kerrison punch
- The sphenoidotomy is enlarged inferiorly, avoiding the septal artery crossing the anterior wall
- The anterior wall, rostrum, and all intersinus septa are drilled away with a semicutting/diamond bur
- This exposes the posterior sinus wall with its key landmarks: sella, bilateral ICAs, optic nerves, optic-carotid recesses, planum sphenoidale
1. Transsphenoidal Approach (Transsellar/Parasellar)
Target lesions: Pituitary adenomas, craniopharyngiomas (sellar/suprasellar), Rathke cleft cysts, parasellar tumors
Key steps after sphenoidotomy:
- The sellar floor is thinned with a drill and removed with Kerrison punches
- The dura is incised in a cruciate fashion after bipolar coagulation
- The ICA and cavernous sinus boundaries define the lateral limits
- Tumor removal proceeds with ring curettes and suction
2. Transcribriform Approach
Target lesions: Olfactory groove meningiomas, esthesioneuroblastoma (olfactory neuroblastoma), anterior cranial fossa tumors, CSF rhinorrhea at cribriform plate
Boundaries of bone removal:
- Laterally: lamina papyracea (orbital walls) bilaterally
- Anteriorly: posterior wall of frontal sinus
- Posteriorly: planum sphenoidale
Surgical steps:
- Complete bilateral ethmoidectomy exposing the skull base from the posterior table of the frontal sinus to the planum sphenoidale
- Bilateral drilling of the bone until eggshell thin, then removal with Kerrison punch
- Dural incision initiated with #11 blade after bipolar cauterization, completed with microscissors on both sides of the falx
- The falx is coagulated, transected, and detached from the crista galli
- The sagittal sinus (if encountered) is packed with Surgicel
- Subpial dissection is done carefully - branches of the anterior cerebral artery (frontopolar artery) are at risk
Reconstruction: Large dural defect requires two-layer fascia lata graft (one intradural, one extradural) covered by the nasoseptal flap. If flap is unavailable (malignant involvement), a lateral nasal or pericranial flap is used.
3. Transtuberculum-Transplanum Approach
Target lesions: Planum sphenoidale and tuberculum sellae meningiomas, suprasellar craniopharyngiomas, Rathke pouch cysts, pituitary macro/microadenomas with suprasellar extension, optic nerve gliomas, pre-chiasmal and post-chiasmal lesions
Surgical steps:
- Binostril transseptal-transnasal access
- Wide sphenoidotomy as above
- High-speed drilling of bone overlying the planum sphenoidale until eggshell thin; final layer removed with Kerrison
- The superior intercavernous sinus is cauterized and transected
- Posterior ethmoid arteries are coagulated and divided
- Dura opened carefully after full bony exposure from sellar region to anterior planum, laterally to lamina papyracea
Critical intradural anatomy to identify:
- ICAs in the paraclinoid region
- A1 and A2 segments of anterior cerebral arteries
- Anterior communicating artery (AComA)
- Recurrent artery of Heubner
- Optic nerves and chiasm (superior)
- Pituitary stalk
Dissection in the arachnoid plane is mandatory; excessive coagulation and traction must be avoided.
Key drill safety: Short intervals of drilling with copious irrigation are used to prevent optic nerve thermal injury - the optic canals are immediately lateral.
Complications and Hazards
| Structure at Risk | Consequence of Injury |
|---|---|
| Internal carotid artery (ICA) | Catastrophic hemorrhage |
| Optic nerve/chiasm | Visual loss/blindness |
| Anterior cerebral arteries | Frontal lobe ischemia |
| Pituitary stalk | Diabetes insipidus, hypopituitarism |
| Sagittal/intercavernous sinus | Venous hemorrhage |
| Cribriform plate/dura | CSF leak, meningitis |
| Olfactory nerves | Anosmia (transcribriform approach) |
Reconstruction
Skull base closure follows a layered approach:
- Intradural layer: fascia lata or fat graft
- Extradural layer: fascia lata
- Vascular flap: nasoseptal (Hadad) flap as the final mucosal cover
- Lumbar drain may be placed intraoperatively for high-flow CSF leaks
Recent Evidence
A 2025 systematic review on olfactory groove meningiomas (PMID 40650805) identified key surgical maneuvers in the endoscopic endonasal transcribriform approach that reduce recurrence. A 2024 systematic review (PMID 38430312) found that endoscopic endonasal salvage surgery after transcranial approaches for craniopharyngioma is feasible and effective, supporting the utility of these extended transsphenoidal corridors.
Sources: Cummings Otolaryngology Head and Neck Surgery, pp. 3390-3401 (Chapter 177: Transnasal Surgical Approaches to the Skull Base)
This is a shared conversation. Sign in to Orris to start your own chat.