Cubital fossa
Reading File
Finding Sources
Searching the Web
cubital fossa anatomy boundaries contents clinical significance
Reading File
Reading File
Loading Image
Here is a complete overview of the cubital fossa, based on Gray's Anatomy for Students:
Cubital Fossa
Definition
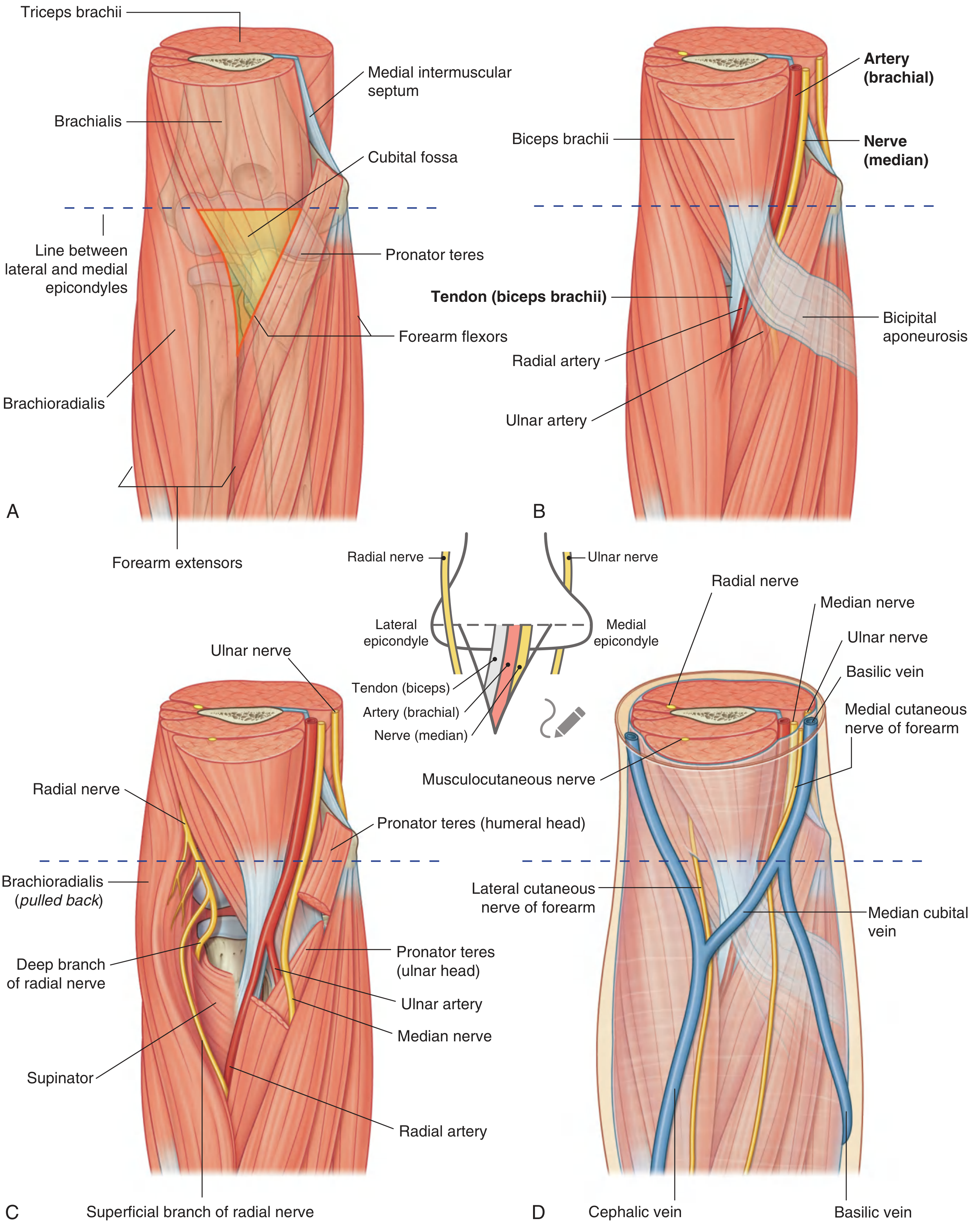
The cubital fossa is a triangular depression on the anterior aspect of the elbow joint, serving as the key area of transition between the arm and forearm. Most major neurovascular structures pass through it as they travel from the arm into the forearm.
Boundaries
| Boundary | Structure |
|---|---|
| Base (superior) | Imaginary line connecting the medial and lateral epicondyles of the humerus |
| Medial border | Pronator teres (from medial epicondyle) |
| Lateral border | Brachioradialis (from lateral supraepicondylar ridge) |
| Apex | Where the two muscles meet distally |
Layers
Roof (superficial to deep)
- Skin
- Superficial fascia
- Deep fascia of forearm
- Bicipital aponeurosis (medially) - covers and protects the brachial artery and median nerve
Floor
- Brachialis muscle (main floor)
- Supinator (lateral part of floor)
Contents (lateral to medial) - Mnemonic: TAN
| Structure | Notes |
|---|---|
| Tendon of biceps brachii | Inserts into the radial tuberosity; the bicipital aponeurosis fans off its medial side |
| Artery (brachial) | Bifurcates into radial and ulnar arteries at the apex; normally bifurcates here but may bifurcate higher in the arm or even in the axilla |
| Nerve (median) | Lies immediately medial to the brachial artery; exits by passing between the ulnar and humeral heads of pronator teres |
The Radial Nerve - NOT strictly inside the fossa
The radial nerve lies just under the lip of brachioradialis, which forms the lateral margin. It divides here into:
- Superficial branch - continues under brachioradialis into the forearm (sensory)
- Deep branch - passes between the two heads of supinator to enter the posterior forearm compartment (motor - becomes posterior interosseous nerve)
The Ulnar Nerve - NOT in the fossa at all
The ulnar nerve passes posterior to the medial epicondyle, completely bypassing the cubital fossa.
Superficial Structures (in the roof)
These lie superficial to the bicipital aponeurosis:
- Median cubital vein - the most important structure in the roof; passes diagonally across the fossa connecting the cephalic and basilic veins
- Lateral cutaneous nerve of forearm (terminal branch of musculocutaneous nerve) - lateral side
- Medial cutaneous nerve of forearm - medial side
- Cephalic vein (lateral) and basilic vein (medial)
Clinical Relevance
1. Venepuncture
The median cubital vein in the roof is the most common site for intravenous cannulation and blood sampling. The bicipital aponeurosis beneath it provides a protective layer separating the vein from the brachial artery and median nerve below.
2. Blood Pressure Measurement
The brachial artery in the cubital fossa is the standard site for auscultating Korotkoff sounds with a stethoscope during BP measurement.
3. Brachial Artery Injury
Supracondylar fractures of the humerus (especially in children) can damage the brachial artery within the fossa, causing ischaemia of the forearm.
4. Median Nerve Compression
The median nerve can be compressed as it exits the fossa between the heads of pronator teres (pronator syndrome), causing pain and weakness.
5. Dialysis Fistula
For haemodialysis, the brachial artery can be surgically anastomosed to the cephalic vein at the elbow (or radial artery to cephalic vein at the wrist), creating an arteriovenous fistula capable of the 250-500 mL/min flow rates needed for dialysis.
6. Biceps Tendon Rupture
A distal biceps tendon rupture presents as a painful snap at the elbow with loss of forearm supination power. The tendon can be felt (or its absence noted) in the cubital fossa.
Summary Mnemonic
"Really Need Beer, Tenderly" (lateral to medial):
- Radial nerve (under brachioradialis, at lateral border)
- Not present - Ulnar nerve is posterior
- Biceps tendon
- Brachial artery
- Nerve (median)
Or simply TAN for the three main contents: Tendon, Artery, Nerve.
Source: Gray's Anatomy for Students, p. 889-891
Causes fort early claditaion in 16 years old
Reading File
Finding Sources
Finding Sources
Searching the Web
causes claudication young person teenager 16 years old differential diagnosis
Finding Sources
Finding Sources
Reading Web Page
https://achaiki-iatriki.gr?p=243
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
I now have enough information to give a thorough answer. Here is the complete breakdown:
Causes of Early Claudication in a 16-Year-Old
Claudication is leg pain (cramping, aching, fatigue) brought on by walking/exercise and relieved by rest. In older patients it almost always means atherosclerotic peripheral arterial disease (PAD). In a 16-year-old, atherosclerosis is virtually never the cause - the differential is completely different.
Why Claudication at Age 16 is Always Pathological
Claudication at this age should never be dismissed. It demands urgent investigation, as every cause listed below is a distinct, diagnosable condition requiring specific treatment.
Causes (Roughly by Frequency in Young Patients)
1. Popliteal Artery Entrapment Syndrome (PAES) - Most Common
The most common cause of claudication in young patients, especially athletic males.
- Mechanism: Abnormal anatomical relationship between the popliteal artery and surrounding musculotendinous structures (usually the medial head of gastrocnemius). Repetitive compression causes progressive arterial wall injury, thrombosis, or embolism.
- Types: Anatomic (structural anomaly) vs. Functional (muscle hypertrophy compresses a normally-placed artery)
- Who gets it: Young athletic men predominantly; bilateral in ~30% of cases; most common in the third decade but well-reported in teenagers
- Symptoms: Calf pain on exertion, cold feet after exercise, paraesthesias; can progress to rest pain and tissue necrosis if undiagnosed
- Key sign: Diminished foot pulses on active plantar flexion against resistance
- Diagnosis: Doppler + ankle-brachial index with provocative maneuvers; CT or MR arteriography confirms anatomy
- Treatment: Surgery (resection/translocation of compressing structure); full recovery if caught early
(Goldman-Cecil Medicine; Harrison's Principles of Internal Medicine 22E)
2. Takayasu Arteritis
A large-vessel granulomatous vasculitis predominantly affecting young women, often of Asian origin.
- Who gets it: Women <40 years, cases reported as young as 5 months
- Mechanism: Inflammatory stenosis/occlusion of the aorta and its major branches
- Symptoms: Limb claudication, peripheral pulse discrepancies, headache, constitutional symptoms (fever, weight loss, fatigue in early "systemic" phase)
- Key signs: Unequal blood pressures in the arms, absent pulses ("pulseless disease"), bruits over carotid/subclavian arteries
- Diagnosis: Imaging (CTA, MRA) showing vessel wall thickening and stenosis; elevated ESR/CRP
- Treatment: Corticosteroids, immunosuppressants; surgical/endovascular revascularization for critical stenosis
(Fuster and Hurst's The Heart, 15th Ed; Bradley and Daroff's Neurology)
3. Cystic Adventitial Disease (CAD)
- A mucinous cyst forms within the adventitial layer of the arterial wall, narrowing the lumen - usually the popliteal artery
- Who gets it: Classically middle-aged men, but can occur in young people
- Characteristic feature: Pain lasts up to 20 minutes after stopping exercise (unlike PAD where pain resolves quickly); Ishikawa's sign - foot pulses disappear with knee flexion (distinguishes CAD from PAES where pulses disappear with plantar flexion/muscle contraction)
- Cause is unknown; may be developmental or post-traumatic
- Treatment: Cyst aspiration or surgical excision
(Goldman-Cecil Medicine)
4. Thromboangiitis Obliterans (Buerger Disease)
- Inflammatory non-atherosclerotic occlusive disease of medium and small arteries of hands and feet
- Who gets it: Young men aged 20-40, strongly associated with heavy tobacco smoking (including smokeless tobacco)
- At age 16 this is possible in a heavy smoker
- Symptoms: Claudication of foot/leg/hand, progressing to ischemic ulcers, peripheral cyanosis, gangrene, migratory superficial thrombophlebitis
- Treatment: Absolute cessation of all tobacco is the only effective intervention
(Rosen's Emergency Medicine; Andrews' Diseases of the Skin)
5. Fibromuscular Dysplasia (FMD)
- Non-inflammatory, non-atherosclerotic disease causing segmental arterial stenosis
- Who gets it: Predominantly young women
- Affects renal arteries (causing hypertension) and carotid/vertebral arteries most often, but can affect iliac/femoral arteries causing claudication
- Imaging: "String of beads" appearance on arteriography
- Treatment: Percutaneous transluminal angioplasty (preferred over surgery)
(Goldman-Cecil Medicine)
6. Coarctation of the Aorta (if undiagnosed)
- Congenital narrowing of the aorta (usually just distal to left subclavian artery)
- Symptoms: Leg fatigue/claudication on exertion, hypertension in upper limbs, weak/absent femoral pulses, headaches, nosebleeds
- Often diagnosed in childhood but mild cases can escape detection until adolescence
- Key signs: Radio-femoral delay, blood pressure differential (arms > legs), rib notching on CXR
- Treatment: Surgical repair or endovascular stenting
7. Chronic Exertional Compartment Syndrome
- Increased intracompartmental pressure during exercise impairs perfusion
- Who gets it: Young athletes (runners)
- Symptoms: Aching/tightness in the leg (usually anterior compartment) that starts at a consistent point during exercise and resolves within 20-30 min of rest - mimics vascular claudication
- Pulses are normal
- Diagnosis: Compartment pressure measurement before and after exercise
- Treatment: Fasciotomy
8. Other Rarer Causes
| Cause | Note |
|---|---|
| Cannabis arteritis | One of the most frequent causes of PAD in adults <40; cannabis-induced arterial inflammation; increasingly relevant in adolescents |
| Antiphospholipid syndrome | Hypercoagulable state causing arterial/venous thrombosis in young people; associated with SLE |
| Homocystinuria | Inborn error of methionine metabolism; premature atherosclerosis and thrombosis in childhood |
| Familial hypercholesterolaemia (homozygous) | Severe premature atherosclerosis starting in childhood |
| Iliac artery endofibrosis | Repetitive trauma to external iliac artery in competitive cyclists/runners; rare |
| Arterial embolism | From cardiac source (e.g. patent foramen ovale, congenital heart disease) |
| Tumour compression | Extravascular mass compressing a major artery |
Approach to a 16-Year-Old with Claudication
History: Exercise type, sport, tobacco/cannabis use, family history, systemic symptoms (fever, weight loss, rashes), cardiac history
Examination: Bilateral blood pressures (arms and legs), all peripheral pulses, radio-femoral delay, auscultation for bruits, skin changes
First-line investigations:
- Ankle-brachial index (ABI) at rest + after exercise
- Doppler ultrasound with provocative maneuvers
- CXR (rib notching)
- Echocardiogram
- ESR, CRP, ANA, antiphospholipid antibodies, lipid profile, homocysteine
Imaging: CTA or MRA of aorta and lower limb vessels
The key takeaway: PAES is the single most likely diagnosis in a fit 16-year-old with exertional leg pain, but Takayasu arteritis, coarctation of the aorta, and other structural/inflammatory causes must always be excluded with appropriate imaging.
Does girl with thyroid problem can have leg weakness and and pain in legs and body pain?
Finding Sources
Searching the Web
hypothyroidism leg weakness muscle pain body aches myopathy symptoms
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Yes, absolutely. A girl with a thyroid problem - particularly hypothyroidism (underactive thyroid) - can definitely have leg weakness, leg pain, and widespread body pain. This is a very well-recognized and common feature of thyroid disease.
Thyroid Problems and Muscle/Body Pain
How Common Is It?
More than 75% of hypothyroid patients have neuromuscular symptoms. This is not rare - it is one of the main features of thyroid disease that often goes unrecognized.
(Rheumatology, 2-Volume Set, Elsevier 2022)
Hypothyroidism (Underactive Thyroid) - the Main Culprit
What Happens to the Muscles?
When thyroid hormone levels are low, the muscles cannot work properly. Thyroid hormone controls energy production, muscle fiber type, and metabolism in muscle cells. Without it:
- Muscles switch from fast to slow fibers
- Energy (glycogen) production in muscles is impaired
- Muscles accumulate abnormal substances (glycosaminoglycans)
- Muscle enzymes (CPK/CK) leak into the blood
Symptoms in the Legs and Body
| Symptom | Details |
|---|---|
| Proximal leg weakness | Difficulty climbing stairs, getting up from a chair, squatting. The thighs and hips are affected most. |
| Muscle pain (myalgia) | Aching, diffuse pain in the legs and throughout the body |
| Muscle stiffness | Especially after rest, worse in the mornings |
| Muscle cramps | Painful sudden cramps, often in the calves |
| Fatigue | Heavy, tired feeling in limbs even at rest |
| Slow reflexes | Ankle jerks and knee jerks are sluggish ("hung-up" reflex) |
| Myoedema | A visible mound/ripple in the muscle after light tapping - a sign specific to hypothyroidism |
(Firestein & Kelley's Textbook of Rheumatology; Goldman-Cecil Medicine)
In Severe Cases
- Rhabdomyolysis - actual breakdown of muscle tissue (very high CK, dark urine - a medical emergency)
- Hoffmann Syndrome - hypothyroidism with muscle stiffness, severe cramps, and muscle enlargement (pseudohypertrophy) - looks like the muscles are big but they are actually weak
Hyperthyroidism (Overactive Thyroid) - Also Causes Weakness
Even an overactive thyroid can cause:
- Proximal muscle weakness with muscle wasting (especially shoulders)
- Brisk (over-active) reflexes
- Occasionally distal weakness too
- Thyrotoxic Periodic Paralysis - episodes of sudden, rapid weakness/paralysis of the legs, worse proximally - can mimic a stroke
Other Thyroid-Related Causes of Leg/Body Pain
| Condition | How it causes pain |
|---|---|
| Carpal tunnel syndrome | Hypothyroidism causes glycosaminoglycan deposits in the wrist, compressing the median nerve - causes hand/arm pain and tingling |
| Joint pain (arthralgia) | Hypothyroidism can cause swelling and pain in joints |
| Fibromyalgia-like picture | Widespread body aching, fatigue, and sleep disturbance, often misdiagnosed as fibromyalgia before thyroid disease is found |
| Hashimoto's thyroiditis | The autoimmune inflammation itself (even before TSH becomes abnormal) can cause muscle and joint pains |
The Good News
Most or all of these symptoms completely resolve once thyroid hormone replacement is started and levels are normalized. The muscle abnormalities on biopsy and the elevated CK return to normal with treatment.
(Rheumatology, 2-Volume Set; Firestein & Kelley's Textbook of Rheumatology)
Practical Bottom Line
If a girl has:
- Leg weakness (especially difficulty climbing stairs or getting up)
- Leg/body pain, aching, cramps
- Along with any of: tiredness, weight gain, cold intolerance, dry skin, hair loss, constipation, heavy periods, slow thinking, puffy face
...then thyroid function tests (TSH + free T4) should be done. It is a simple blood test and can explain all of these symptoms together.
Taxim tab
Finding Sources
Searching the Web
Taxim cefixime tablet uses dose indications side effects
Finding Sources
Reading File
Finding Sources
Reading File
Here is a complete profile of Taxim (Cefixime):
Taxim Tablet - Cefixime
What Is It?
Taxim (also marketed as Taxim-O in India) is the brand name for Cefixime - an oral third-generation cephalosporin antibiotic. It works by binding to penicillin-binding proteins (PBPs) on bacterial cell walls, inhibiting cell wall synthesis and killing bacteria.
- Drug class: Third-generation cephalosporin (beta-lactam antibiotic)
- Available strengths: 100 mg, 200 mg, 400 mg tablets; also oral suspension
Mechanism of Action
Cefixime inhibits bacterial cell wall synthesis by irreversibly binding to transpeptidase enzymes (PBPs), preventing cross-linking of peptidoglycan chains. This leads to cell wall weakness and bacterial lysis (death). It is bactericidal.
It is resistant to many narrow-spectrum beta-lactamases, giving it activity against organisms that break down older penicillins.
Antibacterial Spectrum
Active Against (Sensitive):
| Category | Organisms |
|---|---|
| Gram-positive | Streptococcus pyogenes (Group A strep), Streptococcus pneumoniae (penicillin-sensitive) |
| Gram-negative | Haemophilus influenzae, Moraxella catarrhalis, E. coli, Proteus mirabilis, Klebsiella, Neisseria gonorrhoeae |
NOT Active Against:
- Staphylococcus aureus (MRSA and MSSA - poor activity)
- Pseudomonas aeruginosa
- Anaerobes (e.g., Bacteroides fragilis)
- Enterococcus
- ESBL-producing organisms (resistance)
(Goodman & Gilman's Pharmacological Basis of Therapeutics)
Uses / Indications
| Infection | Notes |
|---|---|
| Urinary tract infections (UTI) | E. coli, Proteus mirabilis - first-choice oral option |
| Pharyngitis / tonsillitis | Due to Streptococcus pyogenes |
| Acute otitis media | H. influenzae, S. pyogenes |
| Acute bronchitis / LRTI | Mild-moderate community-acquired |
| Typhoid fever | Widely used in India for enteric fever (fluoroquinolone-resistant cases) |
| Gonorrhea (uncomplicated) | Single high dose (800 mg) - though ceftriaxone is now preferred due to rising resistance |
| Sinusitis | Acute bacterial sinusitis |
Dosing
| Patient | Standard Dose |
|---|---|
| Adults | 200-400 mg once daily or 200 mg twice daily |
| Children | 8 mg/kg/day in 1-2 divided doses |
| Gonorrhea | 800 mg single dose |
| Typhoid | 15-20 mg/kg/day for 7-14 days |
- Duration: Typically 5-14 days depending on infection
- Can be taken with or without food (food may reduce GI upset)
- Renal adjustment required - dose reduction needed if creatinine clearance < 60 mL/min
Pharmacokinetics
| Parameter | Value |
|---|---|
| Bioavailability | ~40-50% (oral) |
| Half-life (t½) | 3-4 hours |
| Elimination | Both renal (urine) and biliary (bile/feces) |
| Protein binding | ~65% |
(Goodman & Gilman's Pharmacological Basis of Therapeutics)
Side Effects
Common:
- Diarrhea (most common - up to 15% of patients)
- Nausea, vomiting
- Abdominal pain / indigestion
- Headache, dizziness
Less Common:
- Skin rash
- Elevated liver enzymes (transaminases)
- Superinfection with Candida (oral thrush, vaginal candidiasis)
Serious (Rare):
- C. difficile-associated diarrhea / colitis (pseudomembranous colitis) - watery/bloody diarrhea with any antibiotic
- Allergic reaction - rash, urticaria, anaphylaxis (especially if allergic to penicillin - ~1-2% cross-reactivity)
- Stevens-Johnson syndrome (very rare)
Contraindications & Cautions
| Contraindicated | Known allergy to cephalosporins |
| Use with caution | Penicillin allergy (cross-reactivity ~1-2%), renal impairment, history of GI disease |
| Pregnancy | Category B - generally considered safe when needed |
| Breastfeeding | Small amounts in breast milk; use with caution |
Important Drug Interactions
| Drug | Interaction |
|---|---|
| Warfarin | May increase anticoagulant effect - monitor INR |
| Antacids / H2 blockers | May reduce absorption slightly |
| Probenecid | Increases cefixime blood levels (blocks renal secretion) |
Key Points to Remember
- Oral 3rd-gen cephalosporin - convenient once/twice daily dosing
- Good for UTIs, respiratory infections, typhoid (India), ENT infections
- Does NOT cover Staph - do not use for skin/soft tissue infections or hospital-acquired infections
- Complete the full course even if feeling better - stopping early causes resistance and relapse
- Tell your doctor if you have penicillin allergy before taking
- If severe diarrhea develops, stop and seek medical advice (could be C. difficile)
This is a shared conversation. Sign in to Orris to start your own chat.