anatomy and physiology of the nose
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Searching Images
nasal cavity anatomy turbinates septum
Finding Sources
Reading File
Loading Image
Finding Sources
Searching Images
nasal anatomy external nose cartilage bones labeled diagram
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
I now have comprehensive information from multiple authoritative textbooks. Let me compile a thorough response.
Anatomy and Physiology of the Nose
External Anatomy
The external nose consists of a bony and cartilaginous framework covered by skin of varying thickness:
Bony framework:
- The nasal bones form the upper bridge (nasion/rhinion)
- Laterally, the frontal processes of the maxilla provide support
Cartilaginous framework:
- Upper lateral cartilages (ULC) lie below the nasal bones and form the middle third of the nose
- Lower lateral cartilages (LLC) — also called alar cartilages — form the lower third; each has a medial crus, intermediate crus, and lateral crus
- Fibroareolar tissue occupies the base of the nose
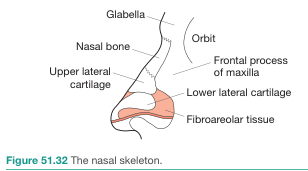
Skin thickness is an important variable: it is thick at the nasion, thin over the rhinion, and thick again over the supratip and tip. — K.J. Lee's Essential Otolaryngology
Nasal Tip Support Mechanisms
Major supports:
- Shape and strength of the lower lateral cartilages
- Attachment of medial crural footplates to the caudal septum
- Attachment of ULC (caudal border) to LLC (cephalic border)
Minor supports:
- Interdomal ligament
- Cartilaginous septal dorsum
- Sesamoid complex extending lateral crura to piriform aperture
- Anterior nasal spine and membranous septum
Internal Anatomy
Nasal Septum
The septum divides the nasal airway into two chambers and is composed of:
- Quadrangular cartilage (anterior)
- Perpendicular plate of the ethmoid (posterior-superior)
- Vomer (posterior-inferior)
Functions include separation of the airway, support of the nasal dorsum, and maintenance of columella shape. Traumatic or developmental deviation can impair olfaction, humidification, filtering of air, and may contribute to chronic sinus disease. — Cummings Otolaryngology
Nasal Cavity
The nasal cavity extends from the nares anteriorly to the choanae posteriorly, communicating with the nasopharynx. Its walls are:
- Floor: hard palate
- Roof: cribriform plate of ethmoid and sphenoid bone
- Medial wall: nasal septum
- Lateral wall: turbinates (conchae)
Turbinates (Conchae)
Three paired bony shelves project from the lateral nasal wall:
- Inferior turbinate — largest; most important for airflow and humidification
- Middle turbinate — landmark for sinus surgery; the ostiomeatal unit lies laterally
- Superior turbinate — smallest; lies near the olfactory cleft
Beneath each turbinate is a meatus (inferior, middle, superior) through which the paranasal sinuses and nasolacrimal duct drain. Turbinate hypertrophy (mucosal or bony) is a common cause of nasal obstruction. — Cummings Otolaryngology
Nasal Valve
The internal nasal valve is the narrowest part of the nasal airway (angle between ULC and septum, ~10–15°). It is the primary site of airflow resistance in the normal nose.
Embryology
Nasal development begins in the 4th week of gestation. Neural crest cells proliferate to form nasal placodes → medial and lateral nasal processes. The medial nasal processes fuse to form the philtrum, columella, and frontonasal process. The nasal pits invaginate, and the nasobuccal membrane ruptures by week 10, allowing nasal–nasopharyngeal communication. The septum develops as a downgrowth from the merged medial nasal and nasofrontal processes. — Cummings Otolaryngology
Blood Supply
The nasal septum receives a dual arterial supply from both the internal and external carotid systems:
| Artery | Territory | Origin |
|---|---|---|
| Sphenopalatine artery | Posteroinferior septum | Internal maxillary artery → external carotid |
| Anterior & posterior ethmoid arteries | Superior septum | Ophthalmic artery → internal carotid |
| Superior labial artery | Anterior septum | Facial artery → external carotid |
| Greater palatine artery | Inferior septum floor | Internal maxillary artery → external carotid |
All these arteries anastomose at the anteroinferior septum in an area called Kiesselbach's plexus (Little's area) — the site of ~95% of anterior nosebleeds. — Pfenninger & Fowler's Procedures for Primary Care
Innervation
- Olfactory nerve (CN I): special sensory; unmyelinated axons from olfactory receptor cells pass through the cribriform plate to the olfactory bulb
- Ophthalmic branch (V1): anterior ethmoidal nerve → external nasal nerve (skin of tip and dorsum)
- Maxillary branch (V2): posterior nasal nerves via sphenopalatine ganglion (mucosa of nasal cavity and septum)
- Autonomic: parasympathetic (via vidian nerve) → vasodilation, mucosal secretion; sympathetic → vasoconstriction
Physiology
Airflow and Resistance
On inspiration, air funnels through the vestibule, accelerates through the narrow nasal valve (up to 16 m/s in cadaver studies), then decelerates ~4-fold as it enters the nasal cavity. This deceleration promotes turbulence that enhances:
- Humidification
- Warming of inspired air
- Particle filtration
- Olfactory contact
The key principle: nasal resistance varies inversely and exponentially with lumen cross-sectional area. Because the nasal valve has the smallest lumen, it is exquisitely sensitive to structural changes. Resistance drops by one-third after topical decongestion, and by two-thirds with full alar retraction. — Cummings Otolaryngology
The Nasal Cycle
First described by Heetderks in 1927: alternating congestion/decongestion of the inferior turbinates occurs in ~80% of people, with a mean cycle of 2.5 hours, controlled by the autonomic nervous system. Total nasal resistance remains constant throughout the cycle. This explains paradoxical nasal obstruction — patients with a fixed septal deviation perceive obstruction on the open (non-deviated) side during its congestion phase. — Cummings Otolaryngology
Autonomic Control of Mucosal Blood Flow
- Parasympathetic: vasodilates sinusoids → congestion and increased secretions
- Sympathetic: provides steady vasoconstrictor tone → decongestion
- Certain medications (e.g., oral contraceptives) alter neural input → mucosal hypertrophy
Mucociliary Clearance
The nasal mucosa is lined by pseudostratified ciliated columnar (respiratory) epithelium with goblet cells. The mucous blanket traps particles; cilia beat toward the nasopharynx, clearing debris and pathogens.
Olfactory Epithelium
The olfactory epithelium is a specialized pseudostratified epithelium located in the superior nasal cavity (olfactory cleft, superior turbinate, roof). It contains three main cell types:
| Cell Type | Structure | Function |
|---|---|---|
| Olfactory receptor cells | Bipolar neurons; apical olfactory vesicle with long nonmotile cilia | Odorant binding and transduction; axons → CN I → olfactory bulb |
| Supporting (sustentacular) cells | Tall columnar, full thickness | Mechanical/metabolic support; secrete odorant-binding proteins |
| Basal cells | Cuboidal, restricted to base | Stem cells; replace receptor cells (~1-month lifespan) |
Olfactory receptor cells are the only neurons in the nervous system that undergo continuous neurogenesis in adult life. Their unmyelinated axons pass through the cribriform plate in small bundles — cribriform plate fractures can sever these fragile axons, causing anosmia. — Histology: A Text and Atlas, Costanzo Physiology
Olfactory Transduction (Signal Cascade)
- Odorant molecules bind to G protein-coupled receptors on olfactory cilia (~1,000 receptor types)
- Receptor activation → Golf protein → adenylyl cyclase activation
- ATP → cAMP increase → opens cation channels (Na⁺, K⁺, Ca²⁺ permeable)
- Depolarization → action potential propagated centrally via CN I to the olfactory bulb
— Costanzo Physiology 7th Edition
Key clinical correlates:
- Septal deviation → turbulent airflow → perceived obstruction even without complete blockade
- Turbinate hypertrophy (mucosal or bony) → persistent obstruction; bilateral mucosal hypertrophy suggests allergic/vasomotor rhinitis
- 50% of inspired air travels along the nasal floor — turbinate and septal floor deviations together significantly affect total flow
- Anterior epistaxis (90%) occurs at Kiesselbach's plexus; posterior epistaxis is rarer but life-threatening and more common after age 40
anatomy and physiology of the pharynx
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Searching Images
pharynx anatomy nasopharynx oropharynx hypopharynx labeled diagram
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Finding Sources
Reading File
Searching Images
pharyngeal constrictor muscles superior middle inferior swallowing
Loading Image
Reading File
I now have comprehensive, well-sourced content from multiple authoritative textbooks. Here is the complete answer:
Anatomy and Physiology of the Pharynx
Overview
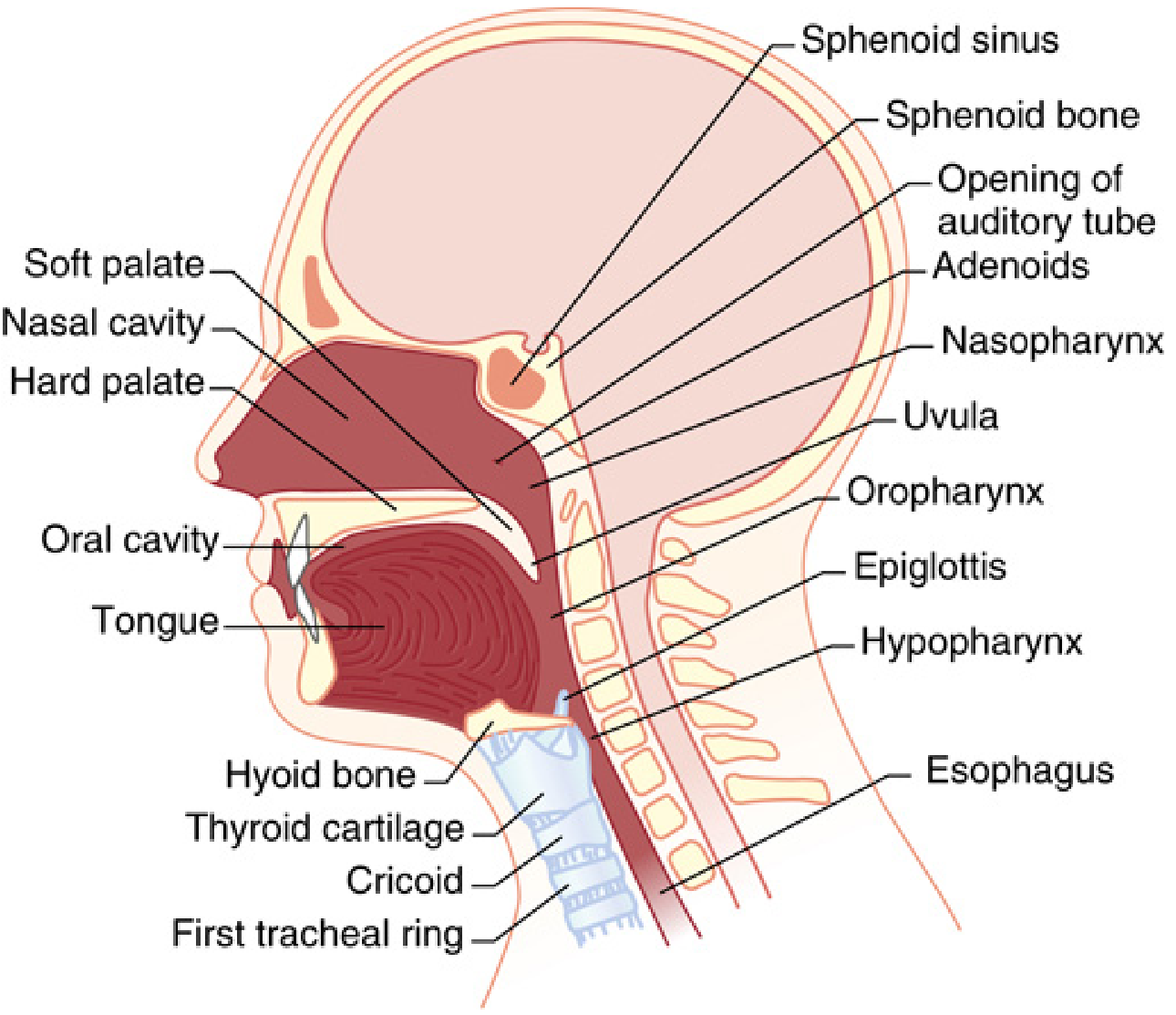
The pharynx is a muscular tube approximately 12–14 cm long that extends from the base of the skull to the level of the inferior border of the cricoid cartilage (C6), where it becomes continuous with the esophagus. It serves as the common pathway for air and food and plays a major role in swallowing, speech, and airway protection.
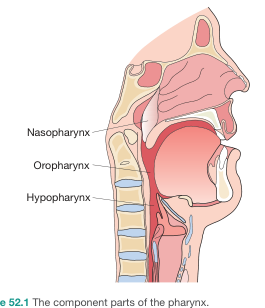
Subdivisions and Boundaries
The pharynx is divided into three regions:
| Region | Superior Boundary | Inferior Boundary |
|---|---|---|
| Nasopharynx | Base of skull | Level of soft palate |
| Oropharynx | Junction of hard and soft palate | Level of hyoid bone (vallecula) |
| Hypopharynx (Laryngopharynx) | Pharyngoepiglottic folds (hyoid level) | Inferior border of cricoid cartilage (C6) |
Nasopharynx
- Subunits: lateral walls (containing the fossa of Rosenmüller and eustachian tube orifice), vault/roof, and posterior wall
- Lined by pseudostratified ciliated columnar (respiratory) epithelium superiorly, transitioning to stratified squamous epithelium inferiorly
- Contains the pharyngeal tonsil (adenoid) on the posterior wall
Oropharynx
- Subunits: soft palate and uvula, base of tongue, palatine arches (tonsillar fossae, palatine tonsils, anterior and posterior pillars), lateral and posterior walls, valleculae, and pharyngoepiglottic/glossoepiglottic folds
- Lined by non-keratinized stratified squamous epithelium
Hypopharynx (Laryngopharynx)
- Subunits:
- Pyriform sinuses (pyriform fossae): paired lateral recesses bordered medially by the aryepiglottic folds and anterolaterally by the thyroid cartilage; the apex is at the level of the cricoid
- Posterior and lateral pharyngeal walls
- Postcricoid region: extends from the arytenoids to the inferior margin of the cricoid, contiguous with the medial walls of the pyriform sinuses
- The narrowest point of the pharyngeal cavity is at the inferior constrictor's attachment to the cricoid
Layers of the Pharyngeal Wall
From inside out:
- Mucosa — stratified squamous epithelium (respiratory in nasopharynx)
- Pharyngobasilar fascia — inner fibrous layer, attaches to the base of skull superiorly
- Muscular layer — constrictors (outer circular) and longitudinal muscles (inner)
- Buccopharyngeal fascia — outer fascia; contains the pharyngeal plexus of nerves and vessels
Muscles
Pharyngeal Constrictor Muscles (Circular)
These muscles narrow the pharyngeal lumen sequentially from top to bottom during swallowing. All three insert into the median pharyngeal raphe posteriorly. All are innervated by CN X (vagus) via the pharyngeal plexus.
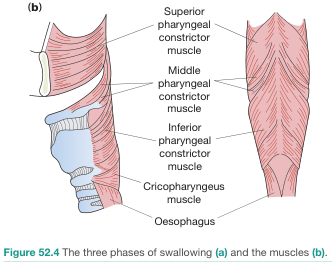
| Muscle | Origin | Key Notes |
|---|---|---|
| Superior constrictor | Pterygomandibular raphe and adjacent mandible and pterygoid hamulus | Forms the lateral and posterior walls of the oropharynx |
| Middle constrictor | Hyoid bone and stylohyoid ligaments | Overlaps the superior constrictor posteriorly |
| Inferior constrictor | Oblique line of thyroid cartilage and lateral surface of cricoid cartilage | Overlaps the middle constrictor posteriorly |
| Cricopharyngeus | Most inferior part of the inferior constrictor | Acts as the upper esophageal sphincter (UES); tonically contracted at rest, relaxes during swallowing |
Clinically Important Gaps in the Pharyngeal Wall
- Killian's dehiscence: triangular gap between the inferior constrictor and cricopharyngeus → site where a Zenker's diverticulum herniates
- Killian–Jamieson space: lateral dehiscence inferior to the cricopharyngeus → passage of branches of the inferior thyroid artery
- Laimer–Hackermann space: between the posterior cricopharyngeus and esophageal musculature
- Oropharyngeal triangle: gap between superior/middle constrictors and posterior border of mylohyoid → allows passage of stylopharyngeus muscle, lingual artery and vein, lingual nerve, CN XII (hypoglossal), CN IX (glossopharyngeal), and lymphatics
Pharyngeal Longitudinal Muscles (Elevators)
These muscles elevate the pharynx and larynx during swallowing:
| Muscle | Origin | Insertion | Action | Innervation |
|---|---|---|---|---|
| Stylopharyngeus | Styloid process of temporal bone | Pharyngeal wall | Elevates pharynx | CN IX (only pharyngeal muscle NOT innervated by CN X) |
| Salpingopharyngeus | Cartilaginous part of pharyngotympanic (Eustachian) tube | Pharyngeal wall | Elevates pharynx | CN X |
| Palatopharyngeus | Upper surface of palatine aponeurosis | Pharyngeal wall (interdigitates with superior constrictor → forms Passavant's ridge) | Elevates pharynx; seals nasopharynx from oropharynx | CN X |
Soft Palate
Function
The soft palate acts as a flutter valve:
- Elevation → closes the pharyngeal isthmus → seals off the nasopharynx (prevents reflux of food into the nasopharynx during swallowing)
- Depression → closes the oropharyngeal isthmus → seals the oral cavity from the oropharynx (allows simultaneous chewing and breathing)
Muscles of the Soft Palate
| Muscle | Action | Innervation |
|---|---|---|
| Levator veli palatini | Raises soft palate to contact posterior pharyngeal wall | CN X (pharyngeal plexus) |
| Tensor veli palatini | Pulls soft palate laterally → rigidity and firmness; opens Eustachian tube | CN V3 (only soft palate muscle NOT innervated via pharyngeal plexus) |
| Palatoglossus (anterior pillar) | Approximates palate to tongue; narrows oropharyngeal opening | CN X |
| Palatopharyngeus (posterior pillar) | Raises larynx and pharynx; closes oropharyngeal aperture | CN X |
| Musculus uvulae | Shortens the uvula | CN X |
Waldeyer's Ring (Lymphoid Tissue)
A ring of lymphoid tissue guarding the entrance to the aerodigestive tract:
- Pharyngeal tonsil (adenoid) — midline posterior nasopharynx
- Palatine tonsils — between palatoglossal and palatopharyngeal arches
- Lingual tonsils — posterior third of tongue
- Tubal (Gerlach) tonsils — at the lip of the fossa of Rosenmüller, posterior to the torus tubarius
- Lateral pharyngeal bands — lymphoid tissue behind the posterior pillars
Immunology: B lymphocytes proliferate in germinal centers; immunoglobulins (IgG, IgA, IgM, IgD), complement, interferon, lysozymes, and cytokines accumulate in tonsillar tissue — first-line immune defense, especially in children. — K.J. Lee's Essential Otolaryngology
Arterial supply to palatine tonsils (five sources): facial artery (main tonsillar branch + ascending palatine), dorsal lingual artery, ascending pharyngeal artery, lesser palatine artery.
Blood Supply
| Region | Artery | Origin |
|---|---|---|
| Upper pharynx | Ascending pharyngeal artery | External carotid |
| Upper pharynx | Ascending palatine + tonsillar branches | Facial artery → external carotid |
| Upper pharynx | Branches of maxillary and lingual arteries | External carotid |
| Lower pharynx | Pharyngeal branches of inferior thyroid artery | Thyrocervical trunk → subclavian artery |
Venous drainage: Pharyngeal venous plexus → pterygoid plexus (infratemporal fossa) → facial and internal jugular veins.
Innervation
Motor
- CN X (vagus) via the pharyngeal plexus → all pharyngeal muscles except stylopharyngeus
- CN IX (glossopharyngeal) → stylopharyngeus (only muscle)
- CN V3 (mandibular) → tensor veli palatini (only soft palate muscle)
The pharyngeal plexus is formed by:
- Pharyngeal branch of CN X (from the inferior vagal ganglion — the dominant motor nerve)
- Branches from the external laryngeal nerve (branch of the superior laryngeal nerve of CN X)
- Pharyngeal branches of CN IX
Sensory
| Region | Nerve |
|---|---|
| Nasopharynx | Pharyngeal branch of CN V2 (maxillary) via palatovaginal canal |
| Oropharynx | CN IX via pharyngeal plexus (afferent limb of gag reflex) |
| Hypopharynx/Laryngopharynx | CN X via internal branch of superior laryngeal nerve |
Lymphatic Drainage
Deep cervical nodes (retropharyngeal, paratracheal, infrathyroid); palatine tonsils drain specifically to the jugulodigastric nodes. — Gray's Anatomy for Students, K.J. Lee's Essential Otolaryngology
Physiology
Swallowing (Deglutition)
Swallowing involves 30+ pairs of muscles, 5 cranial nerves (V, VII, IX, X, XII), and 2 cervical nerve roots (C1–C2). It is coordinated by the swallowing center in the medulla; volitional swallowing also activates the inferior precentral gyrus (lateral motor cortex) bilaterally, as shown by PET and fMRI studies. — Bradley and Daroff's Neurology in Clinical Practice
Three Phases of Swallowing
1. Oral Phase (voluntary)
- Oral preparatory: food taken into mouth, chewed, mixed with saliva; bolus formed by the tongue
- Oral propulsive: tongue propels bolus posteriorly to the pharyngeal inlet in a piston-like action → triggers the involuntary pharyngeal reflex
2. Pharyngeal Phase (reflex, ~1–1.5 seconds)
Initiated by sensory input to the medulla via CN IX and X. The cascade of events:
- Soft palate elevates → closes nasopharynx, preventing nasal regurgitation
- Larynx elevates against the epiglottis (epiglottis deflects posteriorly) → airway protection; glottis closes; respiration inhibited
- UES (cricopharyngeus) relaxes — notably, the UES relaxes just before arrival of the bolus, as laryngeal elevation pulls it open via traction, creating suction that assists bolus entry
- Sequential peristaltic contraction of constrictors (superior → middle → inferior) propels the bolus through the open UES into the esophagus
- Breathing resumes with expiration (not inspiration), reducing aspiration risk
3. Esophageal Phase (reflex + enteric nervous system)
- UES closes once bolus passes
- Primary peristaltic wave (coordinated by the swallowing reflex) travels the length of the esophagus
- If residue remains, secondary peristaltic wave (initiated by enteric nervous system at the site of distension) clears it
- Lower esophageal sphincter (LES) relaxes; bolus enters the stomach
— Costanzo Physiology 7th Edition; Bradley and Daroff's Neurology in Clinical Practice
Speech and Resonance
The pharynx acts as an important resonating cavity for voice. The velopharyngeal sphincter (soft palate + Passavant's ridge formed by palatopharyngeus) gates airflow between the nasopharynx and oropharynx — critical for distinguishing nasal from oral consonants and vowels.
Airway Functions
- The pharynx maintains a patent airway at rest via tonic activation of pharyngeal dilator muscles (especially tensor veli palatini and genioglossus)
- Loss of this tonic activity during sleep underlies obstructive sleep apnea
- The gag reflex (afferent: CN IX; efferent: CN X) protects against foreign body aspiration
Key clinical correlates:
- Zenker's diverticulum herniates through Killian's dehiscence (between inferior constrictor and cricopharyngeus) — typically in older adults; presents with dysphagia, regurgitation of undigested food, and halitosis
- Cricopharyngeal dysfunction (failure of UES to relax) → dysphagia; can be treated with dilation or cricopharyngeal myotomy
- Peritonsillar abscess forms in the space between the palatine tonsil and the superior constrictor
- Nasopharyngeal carcinoma classically presents in the fossa of Rosenmüller and causes ipsilateral serous otitis media (from Eustachian tube obstruction), epistaxis, and cervical lymphadenopathy
anatomy and physiology of the ear
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Searching Images
ear anatomy external middle inner ear labeled diagram cross section
Reading File
Loading Image
Finding Sources
Reading File
Reading File
Searching Images
cochlea cross section scala vestibuli tympani media organ of Corti hair cells
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
I now have comprehensive material from multiple authoritative textbooks. Let me compile the full response.
Anatomy and Physiology of the Ear
The ear is divided into three anatomical regions: the external ear, middle ear, and inner ear. It serves two major sensory functions: hearing (auditory transduction) and balance (vestibular transduction). All three regions are housed within the temporal bone.
The Temporal Bone
The temporal bone consists of four embryologically distinct components:
- Squamous part — forms the lateral wall of the middle cranial fossa; contains the zygomatic process
- Petrous part — pyramid-shaped; houses the inner ear; contains the internal auditory canal (IAC) and carotid canal
- Mastoid part — contains air cells communicating with the middle ear via the antrum
- Tympanic part — forms the walls of the bony external auditory canal (EAC) and anterior/floor of the middle ear
The mastoid antrum lies deep to the MacEwen (suprameatal) triangle, posterior to the spine of Henle — an important surgical landmark. — Cummings Otolaryngology
1. External Ear
Auricle (Pinna)
A funnel-shaped fibroelastic cartilaginous structure that collects and directs sound waves. Its surface landmarks include:
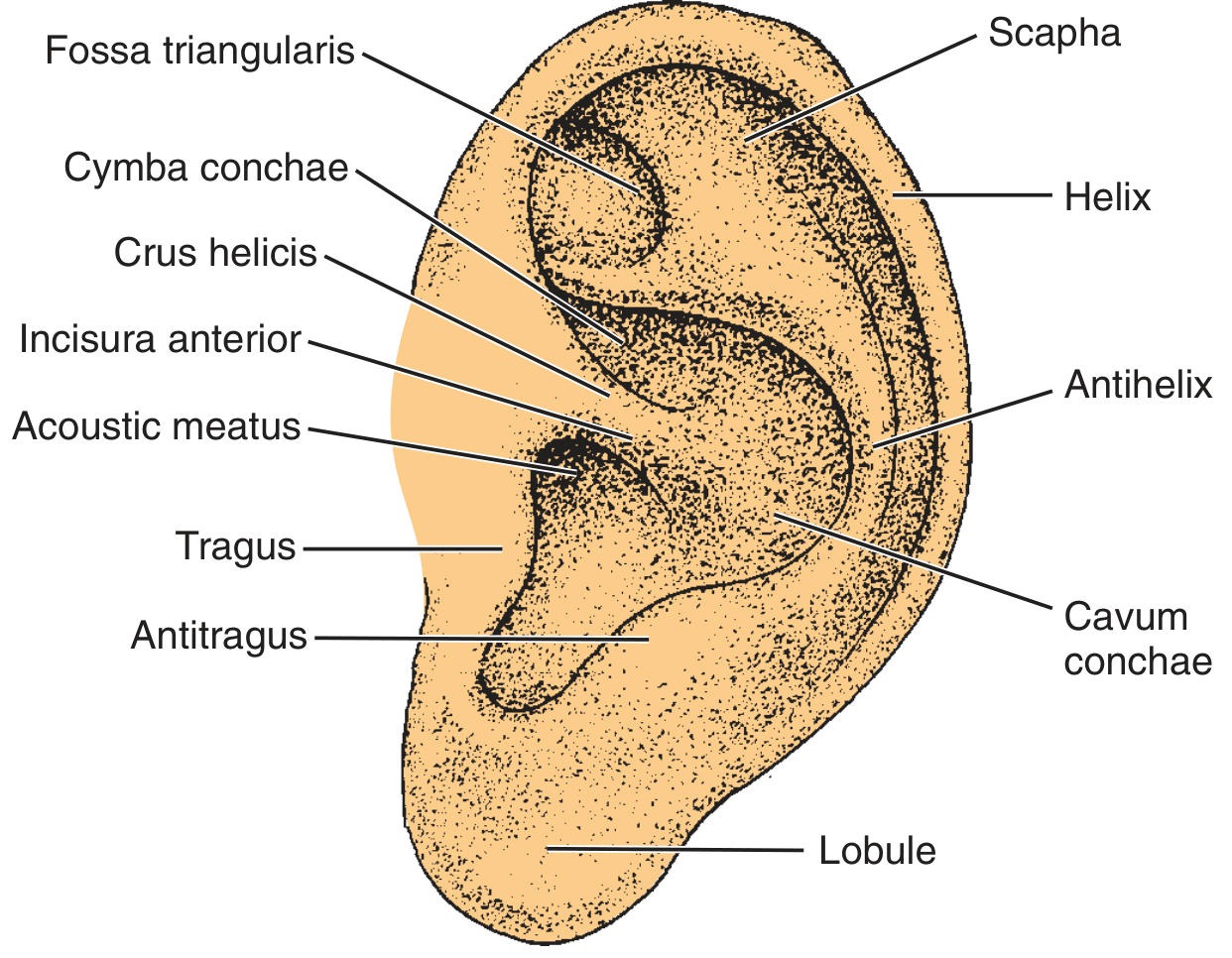
| Structure | Description |
|---|---|
| Helix | Outer curved rim of the auricle |
| Antihelix | Inner curved ridge, parallel to helix |
| Scapha | Groove between helix and antihelix |
| Cymba conchae | Upper part of the concha (bowl) |
| Cavum conchae | Lower part of the concha, leads to meatus |
| Tragus | Cartilaginous projection anterior to the meatus |
| Antitragus | Projection opposite the tragus |
| Fossa triangularis | Depression within the upper antihelix |
| Lobule | Inferior fleshy (non-cartilaginous) portion |
Blood supply: posterior auricular artery and superficial temporal artery (both from external carotid).
External Auditory Canal (EAC)
Approximately 2.5 cm in length; extends from the concha to the tympanic membrane. Comprises:
- Lateral third — cartilaginous (membranous); thick mobile skin; contains ceruminous (apocrine) glands, sebaceous glands, and hair follicles
- Medial two-thirds — bony; thin immobile skin without glands or hair; continuous with the TM epithelium
The bony-cartilaginous junction (isthmus) is the narrowest point — the site where malignant otitis externa presents as granulation tissue (pathognomonic for osteomyelitis). The foramen of Huschke (incomplete ossification of anterior bony canal) and fissures of Santorini (in the cartilaginous canal) are potential routes for spread of EAC malignancy.
Innervation of EAC:
- Auriculotemporal nerve (CN V3) — anterosuperior wall
- Arnold's nerve (auricular branch of CN X) — posterior wall → explains cough reflex from ear stimulation
- Great auricular nerve (C2, C3)
2. Middle Ear
Tympanic Membrane (TM)
A thin, semi-transparent membrane set obliquely (at ~55° to the EAC floor). Composed of three layers:
- Lateral — stratified squamous epithelium (continuous with EAC skin)
- Middle (fibrous layer) — radial and circular collagen fibers
- Medial — simple squamous/cuboidal epithelium (continuous with middle ear mucosa)
The TM is divided into:
- Pars tensa — the larger, taut inferior portion, supported by the fibrous annulus (Gerlach ring)
- Pars flaccida (Shrapnell's membrane) — the smaller, lax superior portion above the lateral process of the malleus; lacks a fibrous middle layer; retraction here leads to cholesteatoma formation
The handle (manubrium) of the malleus is embedded in the fibrous layer of the TM; the umbo is its most medial point, producing a cone of light seen on otoscopy at the 5 o'clock position (right ear).
Middle Ear Spaces (Tympanic Cavity)
The tympanic cavity is subdivided:
- Epitympanum (attic) — above the TM; contains the head of malleus and body/short process of incus
- Mesotympanum — at the level of the TM; main middle ear space
- Hypotympanum — below the TM; overlies the jugular bulb
- Mastoid antrum — posteriorly, communicates via the aditus ad antrum
Prussak's space lies medial to the pars flaccida and lateral to the malleus head — key site of pars flaccida cholesteatoma formation.
Ossicular Chain
Three bones transmit vibrations from the TM to the cochlea:
| Ossicle | Attachment | Notes |
|---|---|---|
| Malleus ("hammer") | Handle embedded in TM; head in epitympanum | Pulled medially by tensor tympani |
| Incus ("anvil") | Body articulates with malleus head; long process connects to stapes | Most vulnerable — single nutrient vessel in long process; no collateral circulation → susceptible to aseptic necrosis |
| Stapes ("stirrup") | Footplate sits in the oval window | Smallest bone in the body |
The ossicles are suspended by ligaments: anterior and superior malleolar ligaments, posterior incudal ligament, and the annular ligament of the stapes at the oval window.
Muscles of the middle ear:
- Tensor tympani (innervated by CN V3): pulls malleus handle medially → tenses TM
- Stapedius (innervated by CN VII): pulls stapes posteriorly → reduces ossicular mobility
Important Middle Ear Landmarks
- Promontory: bony bulge of the basal turn of the cochlea on the medial wall
- Oval window: niche for stapes footplate, leads to scala vestibuli
- Round window: covered by the secondary tympanic membrane, provides pressure relief for the cochlea (opens into scala tympani)
- Facial nerve canal (fallopian canal): courses along the medial wall just above the oval window — critically vulnerable during middle ear surgery
- Cochleariform process: bony pulley for the tensor tympani tendon; landmark for the tympanic segment of CN VII
Eustachian Tube
Connects the middle ear with the nasopharynx (~35 mm long in adults). Normally closed at rest, opening with swallowing and yawning via contraction of the tensor veli palatini. Functions:
- Equalizes middle ear pressure with atmospheric pressure
- Drains middle ear secretions
- Protects middle ear from nasopharyngeal pathogens and sound
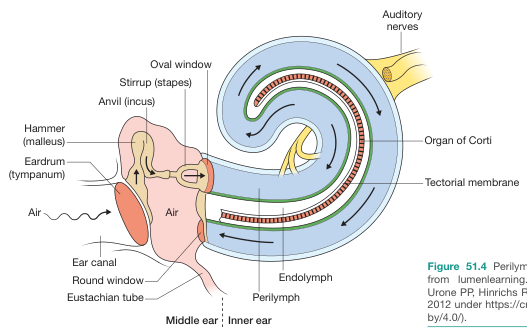
3. Inner Ear
Housed within the petrous temporal bone, the inner ear consists of a bony labyrinth filled with perilymph and a membranous labyrinth within it filled with endolymph.
Fluid composition:
| Fluid | Location | Composition | Similar to |
|---|---|---|---|
| Perilymph | Scala vestibuli, scala tympani | High Na⁺, low K⁺ | Extracellular fluid |
| Endolymph | Scala media, membranous labyrinth | High K⁺, low Na⁺ | Intracellular fluid |
The high K⁺ endolymph creates an endocochlear potential of +80 mV, which drives K⁺ into hair cells during deflection.
Cochlea (Auditory Portion)
A spiral-shaped bony structure making 2.5 turns around a central bony pillar (the modiolus). Contains three fluid-filled scalae (chambers):
| Scala | Fluid | Boundaries |
|---|---|---|
| Scala vestibuli | Perilymph | Above Reissner's membrane; begins at oval window |
| Scala media (cochlear duct) | Endolymph | Between Reissner's membrane (above) and basilar membrane (below) |
| Scala tympani | Perilymph | Below basilar membrane; ends at round window |
Scala vestibuli and scala tympani communicate at the apex via the helicotrema.
The stria vascularis on the lateral wall of the scala media is the highly vascularized epithelium that actively secretes endolymph and maintains the endocochlear potential.
Organ of Corti
The organ of Corti lies on the basilar membrane within the scala media, bathed in endolymph:
- ~3,500 inner hair cells (IHC) — arranged in a single row; receive 90–95% of afferent cochlear nerve fibers; primary sensory detectors
- ~12,000 outer hair cells (OHC) — arranged in 3–4 rows; fewer afferent fibers but many efferent (olivocochlear) fibers; function as active amplifiers ("tuning" the system via electromotility — prestin motor protein)
- Stereocilia project upward from hair cells and are embedded in (OHC) or contact (IHC) the overlying tectorial membrane
- Rods of Corti (pillar cells): triangular support structures; with the reticular lamina and basilar membrane, form a rigid unit
Supporting cells: Deiters' cells, Hensen's cells, Claudius' cells — provide structural and metabolic support.
Physiology of Hearing (Auditory Transduction)
Step 1 — Sound Collection and Transmission
Sound waves enter the EAC → strike the tympanic membrane → ossicles vibrate → stapes footplate pushes into the oval window.
Step 2 — Impedance Matching
Air has far less acoustic impedance than fluid. The TM + ossicular system overcomes this mismatch by:
- Area ratio: TM surface area (~55 mm²) vs. stapes footplate (~3.2 mm²) → ~17-fold force concentration
- Lever action of ossicles: ~1.3-fold mechanical advantage
- Combined effect: ~22-fold increase in force delivered to cochlear fluid
- Without the ossicular system, hearing sensitivity drops 15–20 dB — Guyton and Hall Textbook of Medical Physiology
Step 3 — Basilar Membrane Tonotopy
Stapes movement creates a traveling wave along the basilar membrane:
- Base (near oval window): narrow, stiff → responds to high frequencies (up to 20,000 Hz)
- Apex (helicotrema): wide, flaccid → responds to low frequencies (~20 Hz)
- High frequencies: maximum displacement near base (e.g., 8,000 Hz)
- Low frequencies: maximum displacement near apex (e.g., <200 Hz)
- This place coding (tonotopy) is the principal mechanism of frequency discrimination — Guyton and Hall
Step 4 — Hair Cell Transduction
- Basilar membrane vibration causes the reticular lamina to rock; stereocilia shear against the tectorial membrane
- Deflection toward the kinocilium/longer stereocilia → tip links pull open mechanically gated K⁺ channels → K⁺ flows in from high-K⁺ endolymph → depolarization
- Depolarization opens voltage-gated Ca²⁺ channels → Ca²⁺ influx augments depolarization → release of glutamate from hair cell basal synapses → activates afferent cochlear nerve fibers
- Deflection in the opposite direction → hyperpolarization → decreased firing
- Guyton and Hall Textbook of Medical Physiology
Step 5 — Acoustic Reflex
Loud sounds → reflex contraction of stapedius (latency 40–80 ms) and tensor tympani → ossicular system stiffens → attenuates transmission of low-frequency sounds (<1,000 Hz) by 30–40 dB → protects cochlea from damage
Step 6 — Central Auditory Pathway
Cochlear nerve (CN VIII) → cochlear nuclei (medulla) → superior olivary complex (binaural processing) → inferior colliculus (midbrain) → medial geniculate nucleus (thalamus) → primary auditory cortex (Heschl's gyri, temporal lobe, Brodmann areas 41/42)
Vestibular System (Inner Ear, Balance)
Anatomy
The vestibular apparatus consists of:
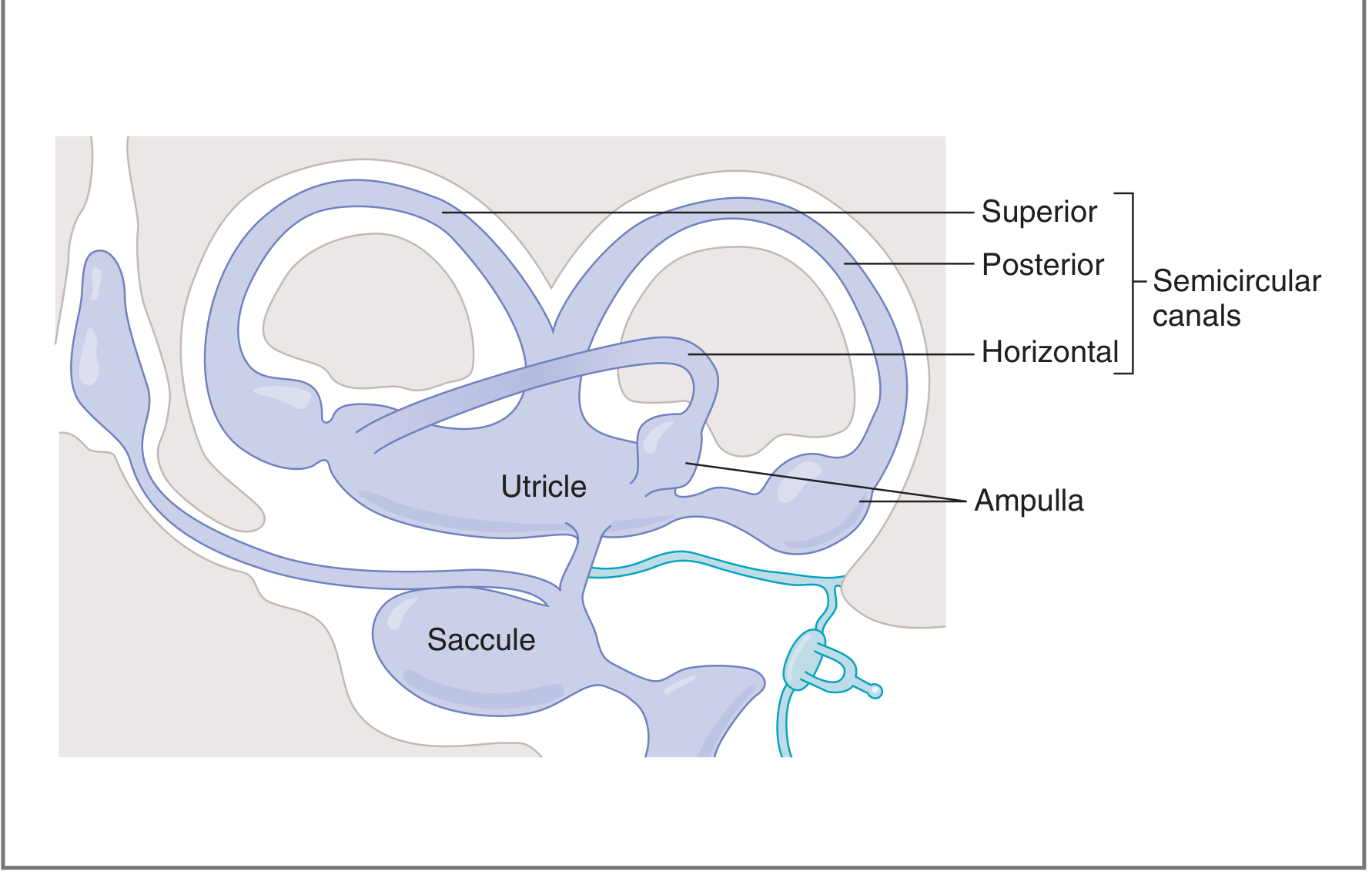
Semicircular canals (3) — detect angular (rotational) acceleration:
- Horizontal (lateral) canal — detects yaw (left–right rotation)
- Superior (anterior) canal — detects pitch (nodding)
- Posterior canal — detects roll (tilting side to side)
- All three are perpendicular to each other → together cover all three axes of rotation
Each canal enlarges at one end into an ampulla containing the crista ampullaris (hair cells covered by the gelatinous cupula). The cupula has the same specific gravity as endolymph.
Otolith organs (2) — detect linear acceleration and gravity:
- Utricle — macula oriented horizontally; detects forward/backward and lateral tilts
- Saccule — macula oriented vertically; detects up/down, pitch, and roll movements
- Both contain a macula: hair cells covered by an otolith membrane embedded with calcium carbonate crystals (otoconia/otoliths)
Vestibular Hair Cells
Unlike cochlear hair cells, vestibular hair cells have a single long kinocilium and multiple stereocilia:
- Bending toward kinocilium → depolarization → increased afferent firing
- Bending away from kinocilium → hyperpolarization → decreased afferent firing
Semicircular canal transduction (e.g., leftward rotation):
- Head rotates left → canals and ampullae rotate left
- Endolymph initially lags behind (inertia) → cupula deflected → hair cells on left canal depolarize, right canal hyperpolarizes
- As rotation continues, endolymph catches up → deflection returns to baseline
- When rotation stops → endolymph continues briefly → reverse deflection → perception of deceleration
Otolith transduction: Head tilt → gravity displaces the heavier otolith mass relative to underlying hair cells → stereocilia bend → differential activation across bilateral otolith organs encodes head position in space. — Costanzo Physiology 7th Edition
Vestibular Pathways
Afferent fibers (CN VIII, vestibular division) → four vestibular nuclei in the medulla (superior, medial, lateral/Deiters', inferior/spinal) →
- Cerebellum (via vestibulo-cerebellar tract) — coordination of gaze and posture
- Spinal cord (via lateral and medial vestibulospinal tracts) — postural reflexes
- Extraocular motor nuclei (via MLF) — vestibulo-ocular reflex (VOR) — stabilizes gaze during head movement
- Thalamus → cortex — conscious perception of motion and spatial orientation
Embryology of the Inner Ear
| Week of Gestation | Event |
|---|---|
| 3 weeks | Otic placode appears; invaginates → otocyst (otic vesicle) |
| 5 weeks | Otocyst divides into pars superior (→ semicircular canals, ampullae) and pars inferior (→ saccule, cochlea); endolymphatic duct is first structure to develop |
| 6 weeks | Cochlear duct grows from saccule |
| 10 weeks | Cochlear duct reaches full 2.5 turns |
| 20 weeks | Cochlea reaches full adult size |
| 21 weeks | Organ of Corti becomes functional |
The outer and middle ear derive from the 1st and 2nd branchial grooves and pouches. — K.J. Lee's Essential Otolaryngology
Key Clinical Correlates
| Condition | Anatomical Basis |
|---|---|
| Conductive hearing loss | Disruption of EAC, TM, or ossicular chain (e.g., otosclerosis fixing the stapes footplate) |
| Sensorineural hearing loss | Damage to cochlear hair cells (noise, ototoxins, aging/presbycusis) or cochlear nerve |
| Cholesteatoma | Keratin cyst arising from retraction of pars flaccida into Prussak's space; erodes ossicles |
| Benign paroxysmal positional vertigo (BPPV) | Displaced otoconia from utricle into posterior semicircular canal → cupulolithiasis/canalolithiasis |
| Acoustic neuroma (vestibular schwannoma) | Tumor of CN VIII in the IAC/CPA angle; presents with unilateral sensorineural hearing loss and tinnitus |
| Malignant otitis externa | Pseudomonas osteomyelitis of temporal bone; granulation tissue at bony-cartilaginous junction is pathognomonic |
| Cochlear implant | Bypasses damaged hair cells; electrodes in scala tympani stimulate spiral ganglion neurons directly |
maxillary sinus
Finding Sources
Finding Sources
Reading File
Reading File
Searching Images
maxillary sinus anatomy walls relations ostiomeatal complex
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Searching Images
maxillary sinus labeled anatomy walls relations teeth orbit
Reading File
Finding Sources
Loading Image
Reading File
Finding Sources
Reading File
Reading File
I now have comprehensive content from multiple authoritative sources. Here is the complete answer.
Maxillary Sinus
Overview
The maxillary sinuses (antra of Highmore) are the largest of the four paranasal sinuses and completely fill the bodies of the maxillae. They are pyramidal in shape with the apex directed laterally (toward the zygomatic process) and the base formed by the medial wall (the lateral nasal wall).
Dimensions
In adults:
- Volume: approximately 15 mL (range 9.5–20 mL)
- Height: ~33 mm; Width: ~23 mm; Depth (AP): ~34 mm
- The largest of all the paranasal sinuses (maxillary > frontal > sphenoid > ethmoid)
Embryology and Development
The maxillary sinus is the second paranasal sinus to develop (after the ethmoid) and is present — albeit very small — at birth.
- Develops as an evagination from the lateral nasal wall (infundibulum/middle meatus region)
- In early childhood: the floor of the sinus lies above the nasal floor due to the presence of unerupted dentition, and the roof slopes downward medial to lateral because the orbit is disproportionately large relative to the midface
- As dentition erupts and the midface grows, the floor descends to and then below the level of the nasal floor
- Reaches near-adult size by puberty; continues slight growth into adult life
- Only the ethmoid and maxillary sinuses are present at birth — K.J. Lee's Essential Otolaryngology
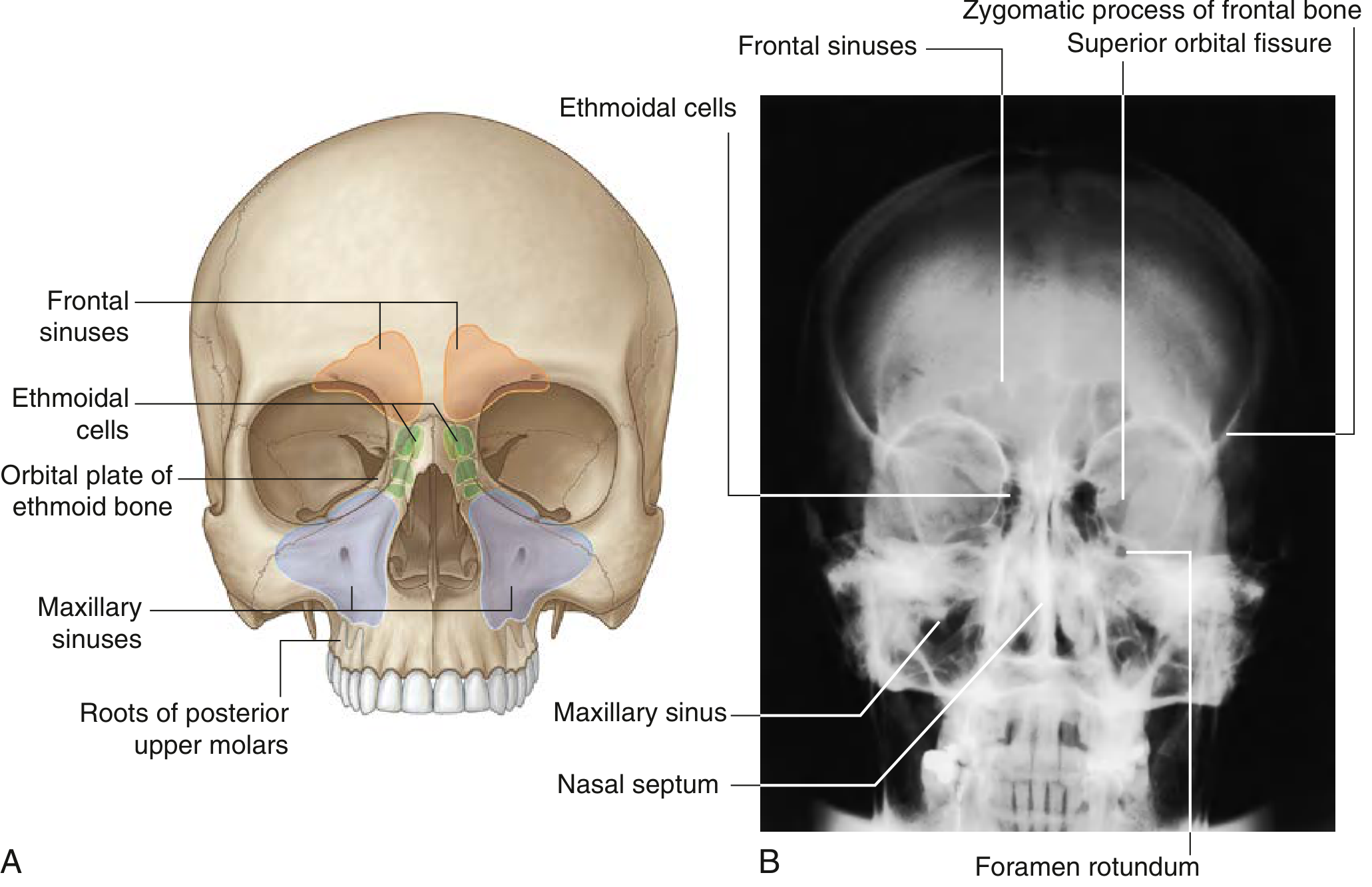
Walls (Boundaries)
The maxillary sinus has six walls:
| Wall | Boundary | Key Relations |
|---|---|---|
| Roof (superior) | Orbital floor | Contains the infraorbital canal with the infraorbital nerve (CN V2), artery, and vein; canal may be dehiscent (~14%) → at risk in surgery |
| Floor (inferior) | Alveolar and palatine processes of the maxilla | Roots of upper premolars and molars may project into the sinus floor; after tooth loss, floor thins further |
| Medial wall (base) | Lateral nasal wall | Contains the natural ostium (medial high on the wall); completed by parts of the inferior concha and palatine bone overlying the maxillary hiatus |
| Anterior wall | Facial (anterior) surface of maxilla | Overlies the canine fossa; contains the infraorbital foramen (infraorbital nerve exits here), anterior superior alveolar canal |
| Posterior wall | Pterygopalatine fossa (PPF) and infratemporal fossa (ITF) | Contains the posterior superior alveolar nerve and vessels; the PPF lies immediately behind, containing the pterygopalatine ganglion and internal maxillary artery |
| Lateral wall (apex) | Zygoma / zygomatic process | Thin; forms the posteromedial infratemporal fossa wall |
Endoscopic landmarks:
- Roof of maxillary sinus ≈ height of sphenoid sinus floor
- Posterior wall of maxillary sinus ≈ depth of sphenoid rostrum
- Medial maxillary wall normally lies in line with a vertical line drawn tangential to the lamina papyracea
— K.J. Lee's Essential Otolaryngology; Cummings Otolaryngology
The Maxillary Ostium and Ostiomeatal Complex
Natural Ostium
The natural ostium of the maxillary sinus:
- Located in the posterior one-third of the ethmoid infundibulum
- Opens high on the medial wall, near the roof of the sinus (not at the floor — an inherently disadvantageous position for gravity drainage)
- Opens at a 45° angle into the floor of the infundibulum
- Diameter: 2.4–4.8 mm (may be enlarged by accessory ostia)
Accessory ostia (fontanelles) are common anatomic variants representing membranous areas in the medial wall not covered by bone; failure to connect natural and accessory ostia during surgery can result in mucus recirculation.
Ostiomeatal Complex (OMC)
The OMC is the critical functional unit for maxillary sinus drainage. It is bounded:
- Laterally: lamina papyracea (medial orbital wall)
- Medially: middle turbinate
Key structures within:
| Structure | Description |
|---|---|
| Uncinate process | Sickle-shaped bony projection from the lateral nasal wall; anterior free margin parallels the ethmoid bulla posteriorly; its superior attachment determines whether the frontal sinus drains into the infundibulum or medial to it |
| Hiatus semilunaris | A 2-dimensional crescentic cleft between the posterior free edge of the uncinate and the anterior face of the ethmoid bulla; the nasal cavity communicates with the infundibulum through this gap |
| Ethmoidal infundibulum | A 3-dimensional funnel-shaped space between the uncinate process and the lamina papyracea; the maxillary ostium opens into its floor |
| Ethmoid bulla (bulla ethmoidalis) | The largest, most constant anterior ethmoid air cell; forms the posterior boundary of the hiatus semilunaris |
Obstruction of the OMC (by inflammation, anatomic variants, or polyps) impairs drainage and ventilation of the maxillary sinus → the pathophysiologic basis of chronic rhinosinusitis. — Cummings Otolaryngology
Mucosal Lining and Histology
The maxillary sinus is lined by pseudostratified ciliated columnar (respiratory) epithelium with interspersed goblet cells — identical to nasal respiratory mucosa but thinner (~0.3 mm vs. 5 mm in the nose).
- Cilia beat in a coordinated spiral pattern directed toward the natural ostium regardless of where material deposits in the sinus (including the floor)
- Mucociliary transport rate in the sinus: ~6 mm/min
- Mucous blanket: two layers — a sol (periciliary) layer and a gel (mucous) layer
- Mucociliary clearance is the primary defense mechanism; impairment (e.g., from viral URI, ciliary dyskinesia, cystic fibrosis) predisposes to sinusitis
Blood Supply
Arterial supply (all ultimately from the external carotid via the maxillary artery):
- Infraorbital artery (from maxillary artery, 2nd part) → roof and anterior wall
- Posterior superior alveolar artery (from maxillary artery) → posterior wall and floor
- Greater palatine artery (from pterygopalatine part of maxillary artery) → floor
- Anterior superior alveolar branch of the infraorbital artery → anterior wall/floor
Venous drainage:
- Into the pterygoid plexus (via veins accompanying the arteries) → internal jugular vein
- Small communications with the facial vein anteriorly
Innervation
All sinus innervation is from the maxillary nerve (CN V2):
| Branch | Territory |
|---|---|
| Infraorbital nerve (anterior, middle, posterior superior alveolar branches) | Roof, floor, anterior and posterior walls |
| Posterior superior alveolar nerve | Posterior wall, floor, related molar roots |
| Middle superior alveolar nerve | Lateral wall, premolar roots |
| Anterior superior alveolar nerve | Anterior wall, canine and incisor roots |
Parasympathetic secretomotor fibers travel via the vidian nerve (nerve of the pterygoid canal) → pterygopalatine ganglion → postganglionic fibers distributed with branches of CN V2 to the sinus mucosa (→ vasodilation and glandular secretion).
Sympathetic fibers (vasoconstriction) join via the deep petrosal nerve → also travel via the vidian nerve.
Lymphatic Drainage
- Anterior: facial lymphatics → submandibular nodes
- Posterior: retropharyngeal and deep cervical nodes
Important Anatomic Relations and Clinical Significance
Relation to Teeth
The roots of the upper posterior teeth are intimately related to the sinus floor — most commonly in order of proximity:
- First molar (most commonly projects into the sinus)
- Second molar
- Second premolar
- Third molar
The average distance between the root apex and the sinus floor is only 1–2 mm; in many cases the roots project directly into the sinus with only mucosa intervening. This explains:
- Odontogenic sinusitis (dental infection seeding the sinus directly)
- Oroantral fistula after tooth extraction
- Referred dental pain in maxillary sinusitis
Relation to the Orbit
The thin roof (orbital floor) means:
- Orbital complications of maxillary sinusitis (orbital cellulitis, subperiosteal abscess)
- Orbital floor fractures ("blowout fractures") → herniation of orbital contents into the sinus
- The infraorbital nerve runs in a canal in the roof and may be dehiscent (14%) → facial numbness in surgery or trauma
Relation to the Pterygopalatine Fossa
The thin posterior wall separates the sinus from the PPF, which contains:
- Pterygopalatine ganglion
- Internal maxillary artery
- CN V2 (as it enters from foramen rotundum)
- Vidian nerve
This makes the PPF accessible via a transantral approach (Caldwell-Luc operation).
Anatomic Variants Relevant to Maxillary Sinus
| Variant | Significance |
|---|---|
| Haller cell (infraorbital ethmoid cell) | Most common anatomic variant; ethmoid cell pneumatizing along the inferomedial orbit; can narrow the ethmoidal infundibulum and obstruct maxillary sinus drainage |
| Accessory maxillary ostium | Can lead to mucus recirculation if not united with the natural ostium |
| Hypoplastic/atelectatic maxillary sinus | Medial wall displaced laterally; can be mistaken for OMC disease on CT; associated with silent sinus syndrome |
| Infraorbital canal dehiscence (~14%) | Infraorbital nerve at risk during endoscopic maxillary surgery |
| Large maxillary sinus | Extensive pneumatization increases proximity of molar roots to sinus floor |
Physiology and Functions
The precise physiologic role of the paranasal sinuses remains debated. Proposed functions include:
- Humidification and warming of inspired air — contribution is minimal given the small ostium
- Lightening of the skull — reduction of cranial weight without sacrificing structural strength
- Resonance of the voice (though this effect is minimal)
- Immune defense — the mucous blanket traps and the mucociliary escalator clears bacteria and particles toward the ostium and into the nasal cavity
- Thermal insulation of orbital contents and brain from facial temperature changes
- Crumple zones — absorb mechanical shock from trauma to the facial skeleton
Key Clinical Correlates
| Condition | Basis |
|---|---|
| Acute maxillary sinusitis | OMC obstruction (usually post-viral) → impaired mucociliary clearance → bacterial superinfection; pain over the cheek worsened by bending forward; purulent nasal discharge |
| Chronic rhinosinusitis (CRS) | Persistent OMC obstruction; CT shows mucosal thickening, infundibular obstruction; treated medically (nasal steroids, saline irrigation) then surgically with FESS |
| Odontogenic sinusitis | ~10–40% of maxillary sinusitis cases; unilateral; caused by periapical abscess, periodontal disease, or implant/extraction complication |
| Oroantral fistula | Communication between oral cavity and sinus after tooth extraction; presents with food/fluid entering the nose |
| Antrochoanal polyp | Large solitary polyp arising from the maxillary sinus mucosa, expanding through the ostium into the nasal cavity and then through the choana into the nasopharynx; commonest in young males |
| Orbital blowout fracture | Trauma transmits force through orbital floor → fractures into the sinus; enophthalmos, diplopia on upgaze (inferior rectus entrapment), infraorbital nerve numbness |
| Caldwell-Luc operation | Historical transantral approach via sublabial incision; access to maxillary sinus, PPF, and infratemporal fossa; largely replaced by FESS |
| Silent sinus syndrome | Chronic OMC obstruction → negative intrasinus pressure → gradual sinus atelectasis and orbital floor depression → enophthalmos and facial asymmetry |
| Mucous recirculation | If an accessory ostium is not connected to the natural ostium during FESS, mucus can exit the natural ostium, re-enter via the accessory ostium, and recirculate indefinitely |
This is a shared conversation. Sign in to Orris to start your own chat.