DIC In pregnancy
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Finding Sources
Reading File
Here is a comprehensive overview of Disseminated Intravascular Coagulation (DIC) in Pregnancy, drawn from authoritative medical textbooks:
Disseminated Intravascular Coagulation (DIC) in Pregnancy
Definition
DIC is an acquired coagulopathy caused by systemic, dysregulated activation of coagulation, resulting in widespread microvascular thrombosis, consumption of platelets and clotting factors, secondary fibrinolysis, and paradoxical bleeding. It is a complication of an underlying disease, never a primary diagnosis.
Pathophysiology
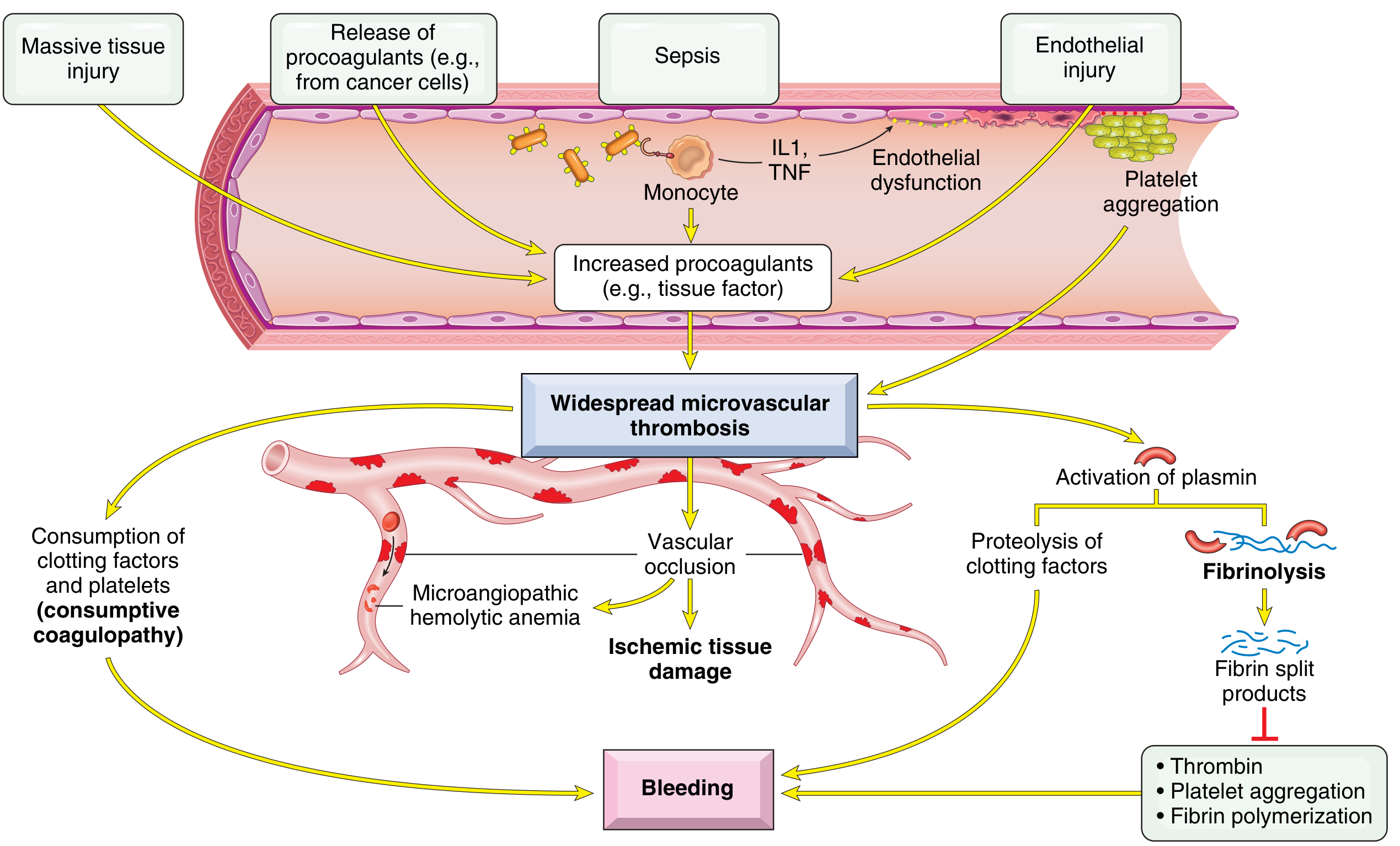
Two main triggers drive DIC:
- Release of tissue factor/procoagulants — Placental tissue, amniotic fluid, and a necrotic/retained fetus are rich sources of thromboplastin (tissue factor), which floods the circulation and triggers the extrinsic coagulation cascade.
- Widespread endothelial injury — As in sepsis, eclampsia, or shock; endothelial damage exposes subendothelial collagen, stimulates tissue factor expression, and downregulates anticoagulants (e.g., thrombomodulin → decreased protein C activation).
The cascade:
- Thrombin is generated in excess, overwhelming its inhibitors (antithrombin III, protein C, TFPI)
- Fibrin is deposited in small vessels → microangiopathic hemolytic anemia + organ ischemia
- Plasminogen activators are secondarily released → fibrinolysis → fibrin degradation products (FDPs/D-dimers)
- FDPs inhibit platelet aggregation, inhibit thrombin, and impair fibrin polymerization → bleeding tendency
- Net result: consumptive coagulopathy — depletion of platelets, fibrinogen, factors V, VIII, and XIII
Acute DIC (as in obstetric emergencies) is dominated by hemorrhage; chronic DIC tends to manifest with thrombosis. — Robbins & Kumar Basic Pathology
Obstetric Causes of DIC
| Cause | Mechanism |
|---|---|
| Abruptio placentae | Most common obstetric trigger; release of placental thromboplastin |
| Amniotic fluid embolism | Amniotic fluid (rich in fetal tissue factor) enters maternal circulation |
| Retained dead fetus | Gradual release of thromboplastic material from necrotic fetal tissue |
| Septic abortion | Endotoxin-mediated endothelial injury and tissue factor expression |
| Eclampsia / severe preeclampsia | Widespread endothelial dysfunction; HELLP syndrome (hemolysis, elevated liver enzymes, low platelets) is a related thrombotic microangiopathy |
| Acute fatty liver of pregnancy (AFLP) | Medical emergency complicated by DIC; affects ~1 in 10,000 pregnancies, 30% fatality; occurs in 3rd trimester with nausea, vomiting, and liver failure |
Clinical Features
- Bleeding: Diffuse petechiae, ecchymoses, oozing from IV/surgical sites, hematuria, GI bleeding, postpartum hemorrhage
- Thrombosis: Microinfarcts in kidneys (cortical necrosis), brain, adrenals (Waterhouse-Friderichsen), heart
- Organ failure: Acute renal failure, dyspnea, cyanosis, convulsions, coma
- Sheehan syndrome: DIC may contribute to postpartum pituitary necrosis via microinfarction of the anterior pituitary
Laboratory Diagnosis
| Test | Finding | Pathophysiology |
|---|---|---|
| Peripheral smear | Schistocytes, low platelets | RBC fragmentation on fibrin strands |
| Platelet count | Low (usually <100,000/mm³) | Consumed in clotting |
| PT | Prolonged | Factors II, VII consumed |
| PTT | Prolonged | Factors II, V, VIII consumed |
| Thrombin time | Prolonged | Low fibrinogen + in vivo fibrinolysis |
| Fibrinogen | Low | Consumed; note: it's an acute-phase reactant so may appear falsely normal early |
| D-dimer / FDPs | Elevated | Secondary fibrinolysis |
| Serum creatinine / UA | Abnormal | Renal microvascular involvement |
— ROSEN's Emergency Medicine
Differential diagnosis: Severe liver disease (jaundice + splenomegaly) and primary fibrinolysis (rare; preserves platelets, factor V, factor VIII in low-normal range) must be distinguished from DIC.
Management
Principle: Treat the underlying cause FIRST
Most obstetric DIC resolves with delivery of the fetus and placenta or with treatment of the precipitating condition (e.g., antibiotics for septic abortion, delivery in AFLP/eclampsia). Many episodes are self-limited once the trigger is removed.
Specific Interventions
| Situation | Treatment |
|---|---|
| Active bleeding | Platelets, Fresh Frozen Plasma (FFP), Cryoprecipitate (for fibrinogen repletion) |
| Monitoring | Fibrinogen levels, platelet count, FDPs — normalization of PT/PTT occurs later and is less useful acutely |
| Fibrin deposition / thrombosis predominant | Consider heparin (e.g., retained dead fetus before delivery, purpura fulminans) |
| Abruptio placentae, severe liver disease, trauma | Heparin is generally NOT helpful |
Antithrombin III, recombinant factor VIIa, and activated protein C have been evaluated but none has demonstrated improved outcomes in DIC. — ROSEN's Emergency Medicine
Goals of Emergency Care
- Early recognition and close monitoring
- Identify and treat the precipitating condition
- Identify life-threatening complications
- Reserve blood products and anticoagulation for specific indications — not routine
Key Summary
- DIC in pregnancy is most often triggered by abruptio placentae, amniotic fluid embolism, retained dead fetus, septic abortion, or eclampsia
- The pathophysiology involves excess thrombin generation → microvascular thrombosis → consumptive coagulopathy → hemorrhage
- Lab hallmarks: ↓ platelets, ↑ PT/PTT, ↓ fibrinogen, ↑ D-dimer, schistocytes
- Management pivots on delivering/removing the obstetric trigger + supportive blood product replacement
- Complications include bilateral renal cortical necrosis, Waterhouse-Friderichsen syndrome, and Sheehan syndrome
Sources: Robbins & Kumar Basic Pathology; ROSEN's Emergency Medicine; Quick Compendium of Clinical Pathology 5th ed.
This is a shared conversation. Sign in to Orris to start your own chat.