Osteoarthritis
Reading File
Finding Sources
Searching Images
osteoarthritis joint pathology X-ray
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a comprehensive overview of osteoarthritis (OA) based on authoritative textbooks:
Osteoarthritis
Definition
Osteoarthritis is characterized by failed repair of synovial joint tissues after intra-articular stress. The resulting breakdown of cartilage and bone leads to pain, stiffness, and functional disability. Despite the "-itis" suffix, it is primarily a degenerative disorder of articular cartilage, with inflammation acting as a secondary contributor.
— Goldman-Cecil Medicine, p. 2765; Robbins & Kumar Basic Pathology, p. 789
Epidemiology
- Affects >500 million people worldwide; the most common joint disease
- Prevalence increases exponentially after age 50 (~40% of those >70 are affected)
- Incidence rises sharply between ages 50–75; women are disproportionately affected
- Knee OA accounts for ~85% of the global burden; lifetime risk ~40% in men and ~47% in women
- Estimated 25% of U.S. adults will have physician-diagnosed OA by 2040
- The global number affected rose 48% from 1990 to 2019
Classification
| Type | Features |
|---|---|
| Primary (idiopathic) | Appears insidiously with aging; oligoarticular; no identifiable cause |
| Secondary | ~5% of cases; younger patients; underlying cause: prior injury, deformity, diabetes, obesity |
Pathogenesis
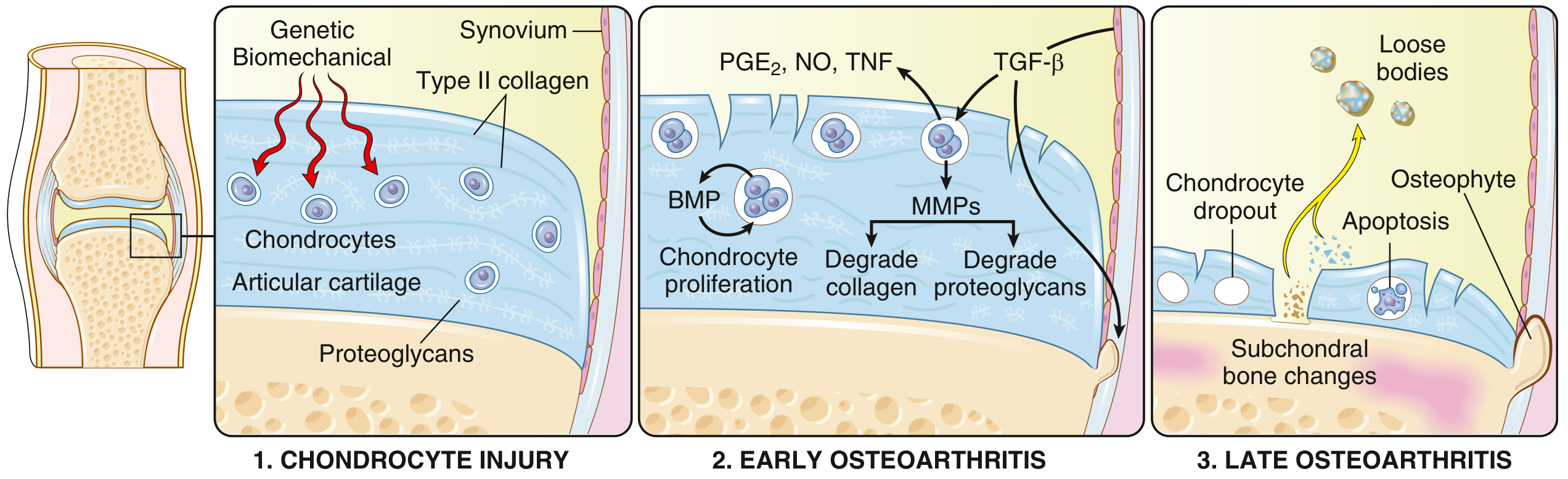
OA stems from an imbalance between repair and destruction of joint tissues driven by mechanical, inflammatory, and metabolic pathways:
-
Chondrocyte injury — Biomechanical stress (obesity, malalignment, occupational risk) or loss of mechanical protection (ligament/meniscal damage) initiates injury, compounded by genetic susceptibility (>100 polymorphic variants identified, >20% heritability)
-
Early OA — Proteoglycan loss causes cartilage swelling and disrupts the type II collagen matrix. Chondrocytes proliferate and secrete matrix metalloproteinases (MMPs) that degrade collagen and proteoglycans. Inflammatory mediators (PGE₂, NO, TNF) are released; TGF-β and BMPs attempt repair but degradation exceeds repair
-
Late OA — Full-thickness cartilage sloughing; loose bodies (joint mice) form from dislodged cartilage and bone fragments; exposed subchondral bone becomes polished (eburnation); subchondral cysts form via a ball-valve mechanism from synovial fluid forced into fracture gaps; osteophytes develop at joint margins via reactivation of endochondral ossification
Synovitis develops secondarily — the synovium becomes hyperplastic and hypertrophic, driven by breakdown products of cartilage and bone.
Morphology / Pathology
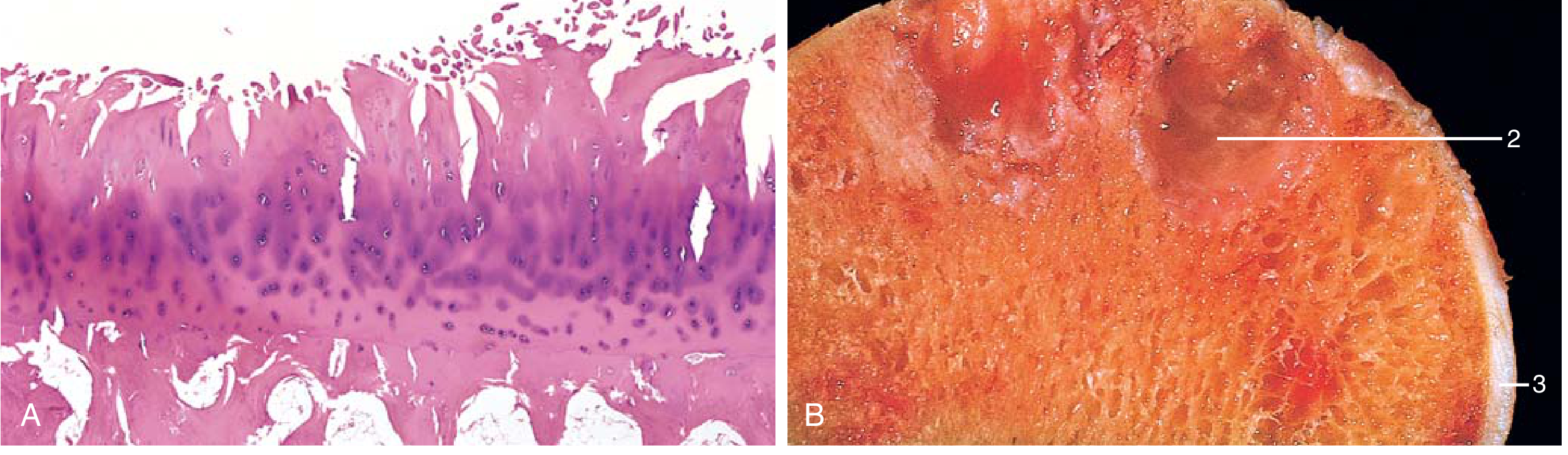
Key morphologic features:
- Cartilage fibrillation and erosion → full-thickness loss in advanced disease
- Bone eburnation — polished ivory appearance of exposed subchondral bone
- Subchondral cysts — fibrous-walled, formed by fluid dissection
- Osteophytes — marginal bony outgrowths capped by fibrocartilage/hyaline cartilage
- Loose bodies (joint mice) — dislodged cartilage/bone fragments in the joint
- Synovium — mildly congested and fibrotic; scattered chronic inflammatory cells (contrast with RA's severe inflammation)
OA vs. Rheumatoid Arthritis — Key Differences
| Feature | Osteoarthritis | Rheumatoid Arthritis |
|---|---|---|
| Primary mechanism | Mechanical injury to cartilage | Autoimmunity |
| Inflammation | Secondary | Primary (T-cell / antibody mediated) |
| Joints involved | Weight-bearing (hips, knees) | Small joints of fingers first, then multiple |
| Pathology | Cartilage degeneration, bone spurs, subchondral cysts; minimal inflammation | Inflammatory pannus, severe synovitis, ankylosis |
| Serum antibodies | None | ACPA, rheumatoid factor |
| Systemic involvement | No | Yes (lungs, heart, other organs) |
| Joint fusion | Does not occur | Can occur (ankylosis) |
Joints Commonly Affected
Hips, knees, lower lumbar and cervical vertebrae, proximal and distal interphalangeal joints (fingers), first carpometacarpal joints, first tarsometatarsal joints.
- Heberden nodes — osteophytes at distal interphalangeal joints; more common in women
- Bouchard nodes — osteophytes at proximal interphalangeal joints
Clinical Features
Symptoms:
- Pain — mechanical in nature, worsens with activity, worse at end of day; at rest in advanced disease
- Morning stiffness — localized, typically <30 minutes (contrast with RA: >1 hour)
- Crepitus — palpable and audible on joint movement
- Limitation of range of motion — progressive
- Functional limitation — difficulty with stairs/rising from chair (knee), putting on shoes (hip), opening jars (hand)
- Catching or locking (especially knee) — risk of falls
Signs:
- Joint line tenderness on palpation
- Bony swelling (osteophytes) and soft tissue swelling (effusion)
- Crepitus (prominent under patella)
- Joint deformity (varus alignment in knee), instability
- Muscle atrophy and weakness
- Hip OA: early restriction of internal rotation with end-range pain
Spinal OA: osteophytes impinge on foramina → cervical/lumbar radiculopathy, muscle spasms, neurologic deficits
Diagnosis
Diagnosis is clinical, based on:
- Symptoms: pain, brief morning stiffness (<30 min), functional limitation
- Signs: crepitus, restricted/painful movement, tenderness, bony enlargement
Plain radiographs are not required but useful for atypical presentations. Radiographic hallmarks:
- Joint space narrowing
- Subchondral sclerosis
- Osteophyte formation
- Subchondral cysts
Laboratory tests are not required to diagnose OA. If coexistent inflammatory disease is suspected (RA, gout, CPPD), check RF, ESR/CRP, synovial fluid analysis.
Synovial fluid in OA: noninflammatory, <2000 leucocytes/μL; basic calcium phosphate crystals often present.
"Red flags" suggesting alternative diagnosis: prolonged morning stiffness, recent trauma, swollen hot joint, rapid symptom worsening.
Management
Core (First-Line) — Nonpharmacologic
Active, nonpharmacologic interventions are the mainstay and should be tried first:
| Intervention | Details |
|---|---|
| Education & self-management | Disease process, realistic expectations, shared decision-making |
| Weight loss | Strongly recommended if BMI ≥25; target 5–10% reduction (more = greater benefit for pain and function) |
| Exercise / physical activity | Aerobic (walking, cycling, swimming), strengthening (quadriceps), neuromuscular/balance, tai chi, yoga, water-based |
| Physiotherapy | Manual therapy, exercise prescription, gait assessment |
Pharmacologic
- Topical NSAIDs — preferred first-line over systemic (better safety profile)
- Oral NSAIDs — first-line if oral analgesia required; lowest dose, shortest duration
- Intra-articular corticosteroids — short-term relief; physical therapy superior for long-term function
- Low-dose oral prednisolone (10 mg/day × 6 weeks) — safe and efficacious short-term for hand OA
- Glucosamine / chondroitin — evidence does not support routine use
- Viscosupplementation (hyaluronic acid injections) — modest evidence, not routinely recommended
- Platelet-rich plasma (PRP) — evidence from RCTs does not show benefit over placebo
- Opioids — similar short-term efficacy to NSAIDs and exercise; use cautiously
Surgical
- Joint replacement — indicated for severe, refractory disease
- There are no disease-modifying treatments that halt or reverse OA progression
Sources: Robbins & Kumar Basic Pathology, pp. 789–791 | Goldman-Cecil Medicine, pp. 2765–2771
This is a shared conversation. Sign in to Orris to start your own chat.