Tell me everything about pancreatitis
Reading File
Finding Sources
Searching PubMed
pancreatitis management
Searching the Web
pancreatitis 2025 guidelines management acute chronic
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information from multiple authoritative sources. I have enough to write a thorough, well-organized answer. Let me compile it.
Pancreatitis: A Comprehensive Overview
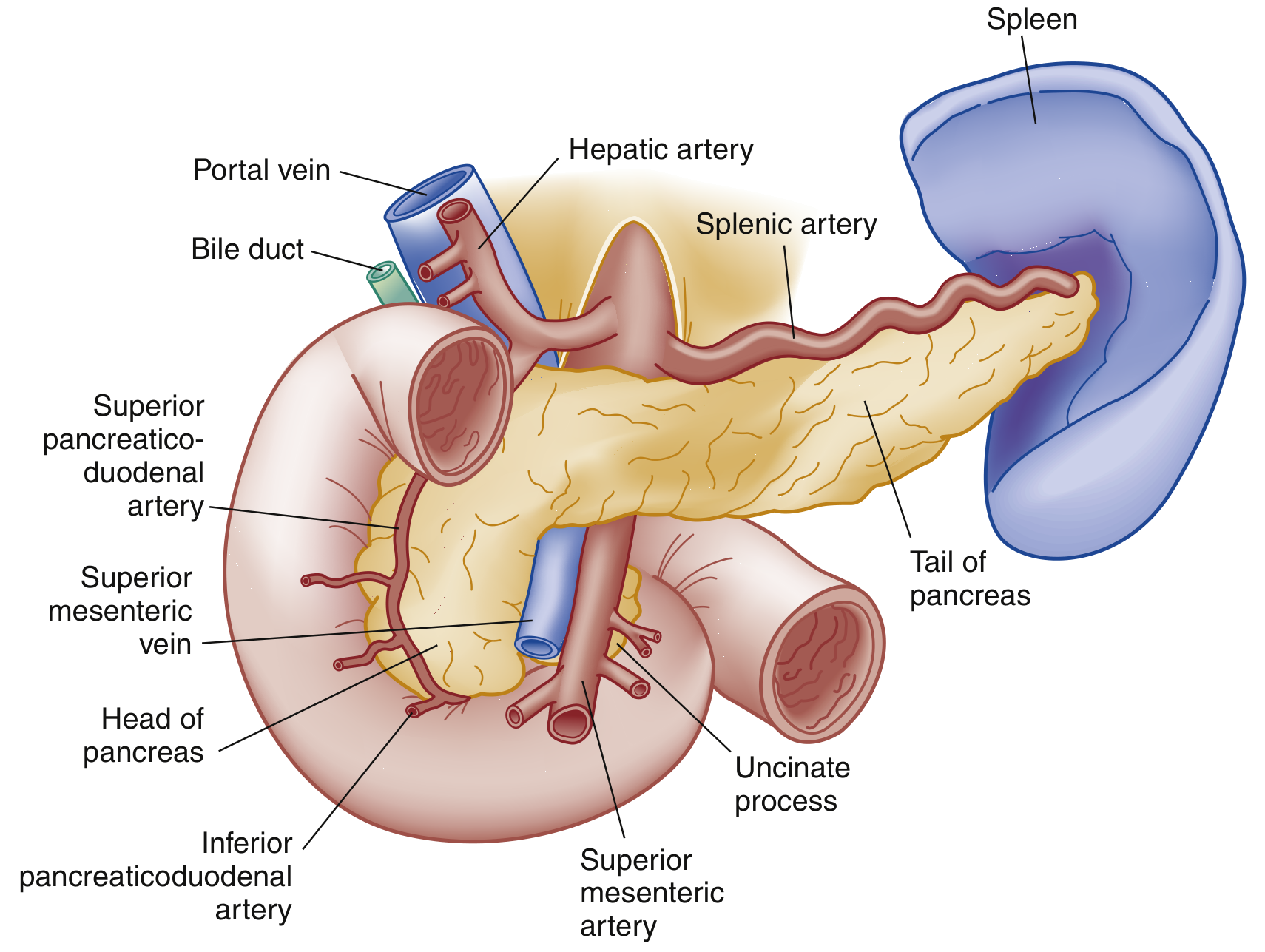
Diagrammatic representation of the pancreas (anterior view) - Rosen's Emergency Medicine
1. Anatomy and Physiology
The pancreas is a retroperitoneal organ with three segments: head, body, and tail. The head sits within the C-loop of the duodenum in the epigastrium. The body traverses posteriorly to the stomach, and the tail abuts the splenic hilum in the left upper quadrant.
A large main pancreatic duct (duct of Wirsung) runs from tail to head and joins the common bile duct to form the ampulla of Vater, draining into the duodenum via the sphincter of Oddi.
- Exocrine function: secretion of digestive enzymes (trypsinogen, lipase, amylase, etc.)
- Endocrine function: secretion of insulin, glucagon, and somatostatin from the islets of Langerhans
2. Classification
Pancreatitis is broadly divided into two forms:
| Feature | Acute Pancreatitis | Chronic Pancreatitis |
|---|---|---|
| Parenchymal damage | Reversible | Irreversible |
| Key outcome | Recovery if cause removed | Progressive fibrosis |
| Exocrine function | May recover | Progressively lost |
| Diabetes risk | Low (mild cases) | High |
- Robbins & Kumar Basic Pathology
These two forms exist on a continuum: recurrent acute pancreatitis can progress to chronic pancreatitis.
3. Acute Pancreatitis
Epidemiology
- Annual incidence: ~40 per 100,000 population in the US (~300,000 hospital admissions/year)
- One of the most common GI discharge diagnoses in US hospitals
- Annual cost: $4-6 billion
- Overall mortality: ~5%; up to 30% in severe cases
- Incidence is rising due to the obesity epidemic and increased gallstone prevalence
- Goldman-Cecil Medicine
Etiology
Gallstones (40-70%) and alcohol (25-35%) account for the vast majority of cases.
Full etiologic classification:
| Category | Causes |
|---|---|
| Toxic-Metabolic | Alcohol, drugs, hypertriglyceridemia (>1000 mg/dL), hypercalcemia, uremia, scorpion venom |
| Mechanical-Obstructive | Gallstones, pancreas divisum, annular pancreas, ampullary/pancreatic tumors, post-ERCP, trauma, duodenal diverticulum |
| Infectious | Viral (mumps, coxsackievirus, HIV, CMV, EBV, varicella); Bacterial (TB, Salmonella, Campylobacter, Legionella, Mycoplasma); Parasitic (Ascaris) |
| Vascular | Vasculitis, embolism, hypoperfusion/ischemia, hypercoagulability |
| Genetic | Mutations in PRSS1 (cationic trypsinogen) and SPINK1 (trypsin inhibitor) genes; CFTR mutations |
| Other | Idiopathic (10-20%), hereditary, autoimmune, DKA |
- Rosen's Emergency Medicine; Robbins & Kumar
Key notes on alcohol: More than 5 years of averaging >5-8 drinks/day is usually required. Most people with heavy alcohol intake do NOT develop pancreatitis - cofactors include high-fat diet, smoking, and genetic mutations. - Goldman-Cecil Medicine
Pathogenesis
The key molecular cascade:
- An inciting event (duct obstruction, toxin, alcohol) disrupts normal acinar cell membrane trafficking
- Premature activation of trypsinogen → trypsin within acinar cells (increased intracellular Ca²⁺ is the critical trigger)
- Trypsin activates other digestive proteases (chymotrypsin, elastase, phospholipase A2, lipase)
- Autodigestion of pancreatic parenchyma and peripancreatic fat
- Recruitment of macrophages and neutrophils amplifies local inflammation
- Cytokine release → increased vascular permeability → edema, hemorrhage, and necrosis
- Systemic cytokine spillover → SIRS, sepsis, multiorgan failure
- Translocation of intestinal bacteria → bacteremia and infected necrosis
- Rosen's Emergency Medicine; Goldman-Cecil Medicine
Classification by Type
- Interstitial edematous pancreatitis (80-90%): Inflammation with pancreatic edema; no necrosis visible on CT; usually resolves within 1 week
- Necrotizing pancreatitis (5-10%): Necrosis of pancreatic parenchyma and/or peripancreatic fat visible on CT; necrotic tissue may remain sterile, liquefy, or become infected (infected necrosis carries highest morbidity)
Clinical Features
Symptoms:
- Persistent, moderate-to-severe epigastric or left upper quadrant pain, classically radiating to the back
- Pain may radiate to chest or flanks
- Nausea, vomiting, anorexia (oral intake worsens pain)
- Pain is relieved by leaning forward ("pancreatic position")
Signs:
- Vitals: fever, tachycardia; hypotension/shock in severe cases
- Abdomen: distension, epigastric tenderness ± guarding; bowel sounds may be absent (ileus)
- Jaundice suggests biliary obstruction
- Cullen sign: periumbilical bluish discoloration (hemoperitoneum) - rare, poor prognosis
- Grey Turner sign: reddish-brown flank discoloration (retroperitoneal bleeding) - rare, poor prognosis
- Murphy sign possible with gallstone pancreatitis
- Basilar crackles/decreased breath sounds if pulmonary complications present
- Rosen's Emergency Medicine
Systemic complications:
| System | Complication |
|---|---|
| Pulmonary | ARDS, pleural effusion (up to 50% of cases, predominately left-sided), atelectasis |
| Cardiovascular | Hypotension, shock (fluid shifts + volume loss) |
| Renal | Acute kidney injury (hypoperfusion + inflammatory mediators) |
| Hematologic | DIC, thrombocytopenia |
| Metabolic | Hyperglycemia (decreased insulin), hypocalcemia (low albumin + Mg²⁺) |
| Vascular | Splenic or portal vein thrombosis |
| GI | Bowel necrosis, gastric outlet obstruction, GI bleeding |
Diagnosis
Diagnostic criteria (2 of 3 required):
- Abdominal pain characteristic of acute pancreatitis
- Serum lipase or amylase >3× the upper limit of normal
- Characteristic findings on abdominal imaging
Laboratory tests:
| Test | Timing | Notes |
|---|---|---|
| Serum lipase | Rises 4-8 hours; elevated up to 14 days | More sensitive and specific than amylase; preferred test |
| Serum amylase | Rises 4-12 hours; normalizes in 3-5 days | Also elevated in salivary gland disease, bowel obstruction, renal failure |
Both amylase and lipase: normal values are amylase 28-100 U/L, lipase 13-60 U/L (>3× ULN for diagnosis). - Robbins & Kumar
Imaging:
- Abdominal ultrasound: First-line to detect gallstones and dilated CBD; pancreas visualization may be limited by gas/habitus
- Contrast-enhanced CT: Most accurate for confirming diagnosis, detecting necrosis (non-enhancing parenchyma = necrotic), and evaluating complications. Best performed ≥3 days after onset. Not routinely needed in mild cases.
- MRI/MRCP: Equivalent to CT for diagnosis; superior for detecting gallstones/microlithiasis; harder to perform in critically ill patients
- EUS: Best for detecting small gallstones, microlithiasis, ampullary lesions, and malignancy when initial workup is unrevealing
- ERCP: Therapeutic (not diagnostic) in acute setting
- Goldman-Cecil Medicine
Severity Assessment
Several scoring systems exist:
- Ranson Criteria (on admission and at 48 hours)
- APACHE II (can be applied at any time; score ≥8 indicates severe disease)
- Bedside Index for Severity in AP (BISAP): BUN >25, altered mental status, SIRS, age >60, pleural effusion
- CT Severity Index (Balthazar score): Based on grade of pancreatic inflammation + % necrosis on CT
Revised Atlanta Classification (2012):
- Mild: No organ failure, no local complications
- Moderately severe: Transient organ failure (<48 hrs) or local complications without persistent organ failure
- Severe: Persistent organ failure (>48 hrs) - single or multi-organ
Treatment of Acute Pancreatitis
1. Fluid Resuscitation:
- Aggressive IV hydration is the cornerstone of early management
- Lactated Ringer's preferred over normal saline (reduces SIRS)
- Goal-directed resuscitation (target urine output, heart rate, MAP)
2. Pain Management:
- Analgesics including opioids as needed for pain control
- NSAIDs and patient-controlled analgesia used in some settings
3. Nutrition (Major paradigm shift):
- Old approach: NPO to "rest" the pancreas - no longer recommended
- Current approach: Early enteral nutrition (EN) is superior to parenteral nutrition (PN)
- In ICU/severe cases: Nasogastric or nasojejunal tube feeding started within 24-36 hours of admission
- In mild cases (minimal SIRS, managed on ward): Offer oral diet as tolerated; start EN only if oral diet fails after 4 days
- Meta-analyses show EN vs PN: 2-fold reduction in infectious complications, 2.5-fold reduction in mortality
- EN significantly reduces infected peripancreatic necrosis (OR 0.28), single organ failure (OR 0.25), and multi-organ failure (OR 0.41) vs PN
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease
4. Role of ERCP:
- Indicated within 24-72 hours in gallstone pancreatitis with concurrent cholangitis or biliary obstruction
- Not routinely recommended in mild biliary pancreatitis without obstruction
5. Antibiotics:
- NOT routinely indicated for acute pancreatitis
- Reserved for proven infected necrosis (confirmed by FNA or clinical signs)
- Imipenem/meropenem or fluoroquinolones used when infected necrosis confirmed
6. Management of Infected Necrosis ("Step-Up Approach"):
- Percutaneous drainage → endoscopic transluminal necrosectomy (via EUS) → video-assisted retroperitoneal debridement (VARD) → open surgery
- Surgical necrosectomy is a last resort
7. Cholecystectomy:
- For gallstone pancreatitis: early cholecystectomy during the index admission (in mild disease) is now recommended to prevent recurrence per 2025 ACG and IAP guidelines - per the IAP 2025 Revised Guidelines
4. Chronic Pancreatitis
Definition and Key Features
Chronic pancreatitis involves irreversible destruction of exocrine pancreatic parenchyma with replacement by fibrous tissue. Unlike acute pancreatitis, inflammation and damage continue even after the causative agent is removed.
Key consequences:
- Exocrine insufficiency → malabsorption, steatorrhea
- Endocrine insufficiency → pancreatogenic (type 3c) diabetes
- Chronic abdominal pain
- Weight loss
Causes
Same broad categories as acute pancreatitis but chronic exposure:
- Alcohol (most common in adults; >10 years of heavy use typical)
- Idiopathic (tropical pancreatitis in South/Southeast Asia)
- Genetic: PRSS1, SPINK1, CFTR mutations (hereditary pancreatitis)
- Autoimmune pancreatitis (AIP): IgG4-related (Type 1) or not (Type 2)
- Obstruction: Tumors, strictures, pancreas divisum
- Recurrent acute pancreatitis of any cause
Clinical Features
- Chronic, recurrent epigastric pain (classically postprandial, radiating to back)
- Steatorrhea - fatty, bulky, foul-smelling stools (occurs when >90% of exocrine function is lost)
- Weight loss from malabsorption, reduced food intake (pain with eating), and hypermetabolism
- Diabetes mellitus (endocrine failure in advanced disease)
- Jaundice if common bile duct stricture develops
Diagnosis
- Labs: Low fecal elastase-1 (exocrine insufficiency); elevated glucose/HbA1c; possible elevated bilirubin
- Imaging:
- CT/X-ray: Pancreatic calcifications (pathognomonic in alcohol-related CP)
- MRCP: Duct irregularity, strictures, dilation ("chain of lakes" appearance)
- EUS: Most sensitive for early changes (parenchymal and ductal changes)
- ERCP: Diagnostic + therapeutic for duct strictures/stones
- Secretin stimulation test: Gold standard for exocrine function (rarely used)
Treatment of Chronic Pancreatitis
1. Pain management:
- Analgesic ladder (paracetamol → NSAIDs → opioids)
- Pregabalin/tricyclics for neuropathic pain
- Pancreatic enzyme replacement therapy (PERT) may reduce pain by feedback inhibition
- Antioxidants (selenium, ascorbic acid, β-carotene, α-tocopherol, methionine): some RCT evidence of pain benefit (32% pain-free vs 13% placebo in one trial), but conflicting evidence exists
- Cessation of alcohol and smoking is mandatory
2. Exocrine insufficiency (Pancreatic Enzyme Replacement Therapy - PERT):
- Lipase-containing enzyme supplements taken with every meal
- Fat-soluble vitamin supplementation (A, D, E, K)
- Low-fat diet
3. Endocrine insufficiency:
- Pancreatogenic diabetes (type 3c) management: insulin is typically needed
- Caution with oral hypoglycemics due to altered glucagon response and malnutrition risk
4. Nutritional support:
- Jejunal tube feeding to improve weight and reduce pain
- Reduces GI side effects and narcotic use
5. Endoscopic therapy:
- ESWL (extracorporeal shock wave lithotripsy) + ERCP for pancreatic duct stones
- Endoscopic stenting for duct strictures
- Drainage of symptomatic pseudocysts
6. Surgery:
- Indicated for pain refractory to medical/endoscopic therapy, or complications (CBD obstruction, duodenal stenosis, suspected malignancy)
- Operations: Frey procedure, Beger procedure (head resection with duct drainage), Puestow (lateral pancreaticojejunostomy), distal pancreatectomy, or total pancreatectomy with islet autotransplantation (TPIAT)
- Sleisenger and Fordtran's GI and Liver Disease
5. Local Complications of Pancreatitis
| Complication | Description | Timing |
|---|---|---|
| Acute peripancreatic fluid collection | Homogeneous fluid in/around pancreas, no wall | <4 weeks, acute phase |
| Pancreatic pseudocyst | Encapsulated fluid collection with well-defined wall; no solid material | >4 weeks |
| Acute necrotic collection | Heterogeneous collection with both fluid and necrotic tissue | <4 weeks |
| Walled-off necrosis (WON) | Mature encapsulated necrosis with thick wall | >4 weeks |
| Infected necrosis | Necrotic tissue with bacterial infection; gas on CT | Any time after necrosis |
| Splenic/portal vein thrombosis | Inflammatory compression of vessels | Late |
| Pancreatic fistula | Communication of pancreatic duct to peritoneum or pleura | Late |
| Pancreatic ascites / pleural effusion | High amylase in ascitic/pleural fluid | Late |
6. Pancreatitis and Malignancy Risk
- Chronic pancreatitis is a risk factor for pancreatic adenocarcinoma (10-20x elevated lifetime risk)
- Hereditary pancreatitis (PRSS1 mutations) carries up to 40% lifetime risk of pancreatic cancer
- Any patient with chronic pancreatitis, especially over age 40, should be monitored for malignancy with periodic imaging
7. Key Scoring Systems Summary
Ranson Criteria (original, for alcohol-related pancreatitis):
At admission: Age >55, WBC >16,000, glucose >200 mg/dL, LDH >350 IU/L, AST >250 IU/L
At 48 hours: Hematocrit drop >10%, BUN rise >5 mg/dL, Ca²⁺ <8 mg/dL, PaO₂ <60 mmHg, base deficit >4, fluid sequestration >6L
Score ≥3: Severe pancreatitis
BISAP Score:
- BUN >25 mg/dL
- Impaired mental status
- SIRS (≥2 of 4 criteria)
- Age >60
- Pleural effusion on imaging
Score ≥3: High risk of organ failure and mortality
8. 2025 Guideline Updates
Per the IAP/APA 2025 Revised Guidelines on Acute Pancreatitis, key updated recommendations include:
- Pain control optimization (non-opioid preferred where possible)
- Goal-directed fluid therapy (avoiding over-resuscitation with normal saline)
- Early enteral nutrition strongly recommended
- Step-up approach (percutaneous → endoscopic → surgical) for infected necrosis
- Early cholecystectomy for mild biliary pancreatitis during index admission
- Strategies for prevention of recurrence (including early ERCP sphincterotomy when cholecystectomy is not feasible)
The ACG 2025 guidelines also caution against overdiagnosis - elevated lipase/amylase >3× ULN without compatible symptoms (e.g., in gastroenteritis) should NOT be labeled as acute pancreatitis.
Sources:
- Robbins & Kumar Basic Pathology, pp. 646-650
- Goldman-Cecil Medicine (International Edition), Chapter 130
- Rosen's Emergency Medicine, Chapter 77
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease
- IAP Revised Guidelines on Acute Pancreatitis 2025
- ACG Acute Pancreatitis Guideline 2025
This is a shared conversation. Sign in to Orris to start your own chat.