I now have comprehensive content for both topics. Here is a complete, structured answer:
1. ACE Inhibitors
Mechanism of Action
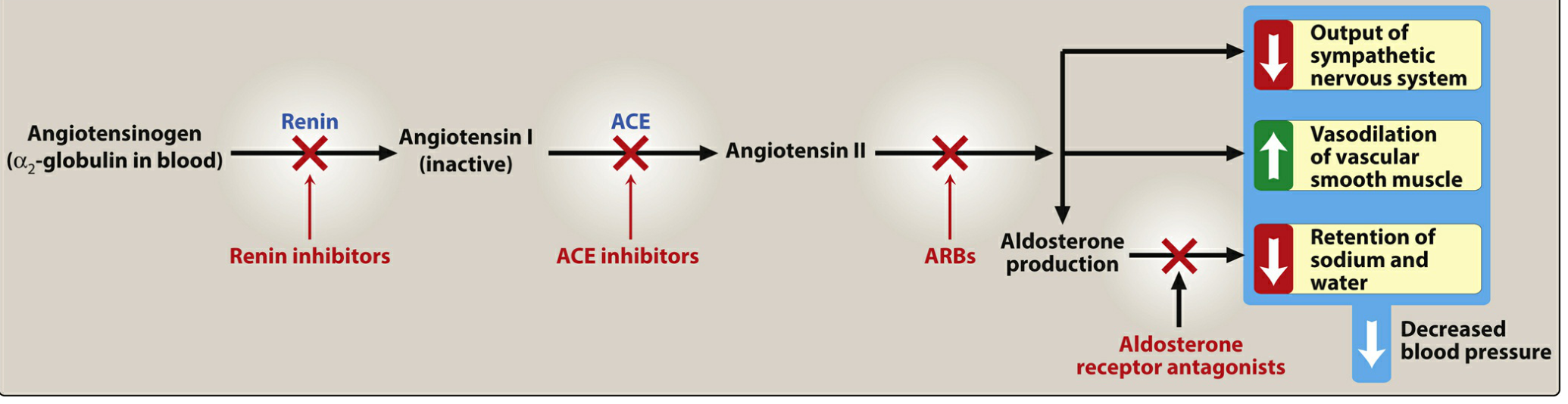
ACE inhibitors (captopril, enalapril, lisinopril, ramipril, fosinopril, quinapril, perindopril, trandolapril, benazepril, moexipril) lower blood pressure by blocking angiotensin-converting enzyme (ACE), which normally:
- Cleaves angiotensin I → angiotensin II (potent vasoconstrictor)
- Degrades bradykinin (a vasodilator that stimulates NO and prostacyclin release)
Net result:
- ↓ Angiotensin II → less vasoconstriction, ↓ aldosterone → ↓ Na⁺/water retention
- ↑ Bradykinin → enhanced vasodilation
- Dilation of both arterioles and veins → ↓ preload and afterload
- Renal: efferent arteriolar vasodilation → ↓ intraglomerular pressure
Figure: Effects of drug classes on the renin–angiotensin–aldosterone system. — Lippincott Pharmacology
Spectrum of Indications
| Indication | Notes |
|---|
| Hypertension | First-line, especially with compelling indications |
| Heart failure (systolic) | Reduce workload, improve remodeling |
| Post-MI | Improve ventricular remodeling and survival |
| Diabetic nephropathy | Slow progression, reduce albuminuria |
| Chronic kidney disease | Renoprotective via ↓ intraglomerular pressure |
| LV hypertrophy | Regression of hypertrophy |
| Coronary artery disease | Risk reduction |
Pharmacokinetics
- All are orally bioavailable (as drug or prodrug)
- Most (except captopril and lisinopril) require hepatic conversion to active metabolite — these two are preferred in severe hepatic impairment
- Most are renally eliminated — except fosinopril (no dose adjustment in renal impairment)
- Enalaprilat is the only IV formulation
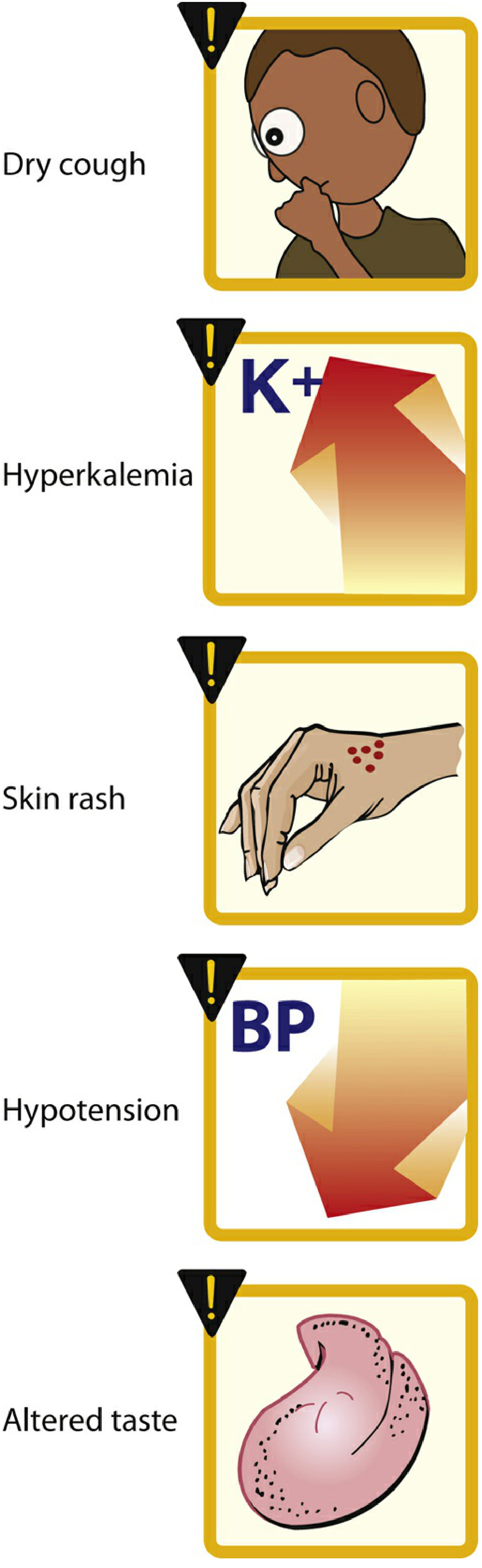
Adverse Effects
Figure: Common adverse effects of ACE inhibitors. — Lippincott Pharmacology
| Side Effect | Mechanism | Notes |
|---|
| Dry cough | ↑ Bradykinin + substance P in lungs | Up to 10% of patients; more common in women; resolves on discontinuation |
| Angioedema | ↑ Bradykinin → swelling of lips, mucosa, throat | Rare but life-threatening |
| Hyperkalemia | ↓ Aldosterone → ↓ K⁺ excretion | Monitor K⁺; caution with K⁺-sparing diuretics/supplements |
| ↑ Serum creatinine | Efferent arteriolar dilation | Up to 30% rise acceptable; monitor in renal disease |
| Hypotension | Vasodilation | Especially first-dose effect |
| Skin rash, altered taste | (captopril more common, due to SH group) | |
| Teratogenicity | Fetal renal malformations | Contraindicated in pregnancy |
Contraindications
- Pregnancy (teratogenic — fetal renal dysplasia)
- Bilateral renal artery stenosis (can precipitate acute renal failure)
- History of ACE inhibitor-induced angioedema
- Hyperkalemia
- Concurrent use with ARB + ACE inhibitor (not recommended — similar mechanism, additive toxicity)
- Aliskiren + ACE inhibitor in diabetic patients (contraindicated)
Drug Interactions
| Interaction | Effect |
|---|
| K⁺-sparing diuretics (spironolactone, amiloride) | ↑ Risk of hyperkalemia |
| K⁺ supplements | ↑ Risk of hyperkalemia |
| NSAIDs | Blunt antihypertensive effect; worsen renal function |
| ARBs / aliskiren | Increased adverse effects without additional benefit in hypertension |
| Lithium | ACE inhibitors ↓ lithium excretion → toxicity risk |
| Diuretics | Additive hypotension (especially first dose) |
| Antidiabetic agents | ACE inhibitors may enhance insulin sensitivity → hypoglycemia risk |
2. Drugs for Bradyarrhythmia
Definition & Classification
Bradycardia = HR < 60 bpm; clinically significant when < 50 bpm or causing symptoms (altered mental status, hypotension, chest pain, acute HF, shock).
Types:
- Supraventricular: sinus/junctional bradycardia, AV blocks (1°, 2° Mobitz I/II)
- Ventricular: 3° (complete) AV block with idioventricular escape
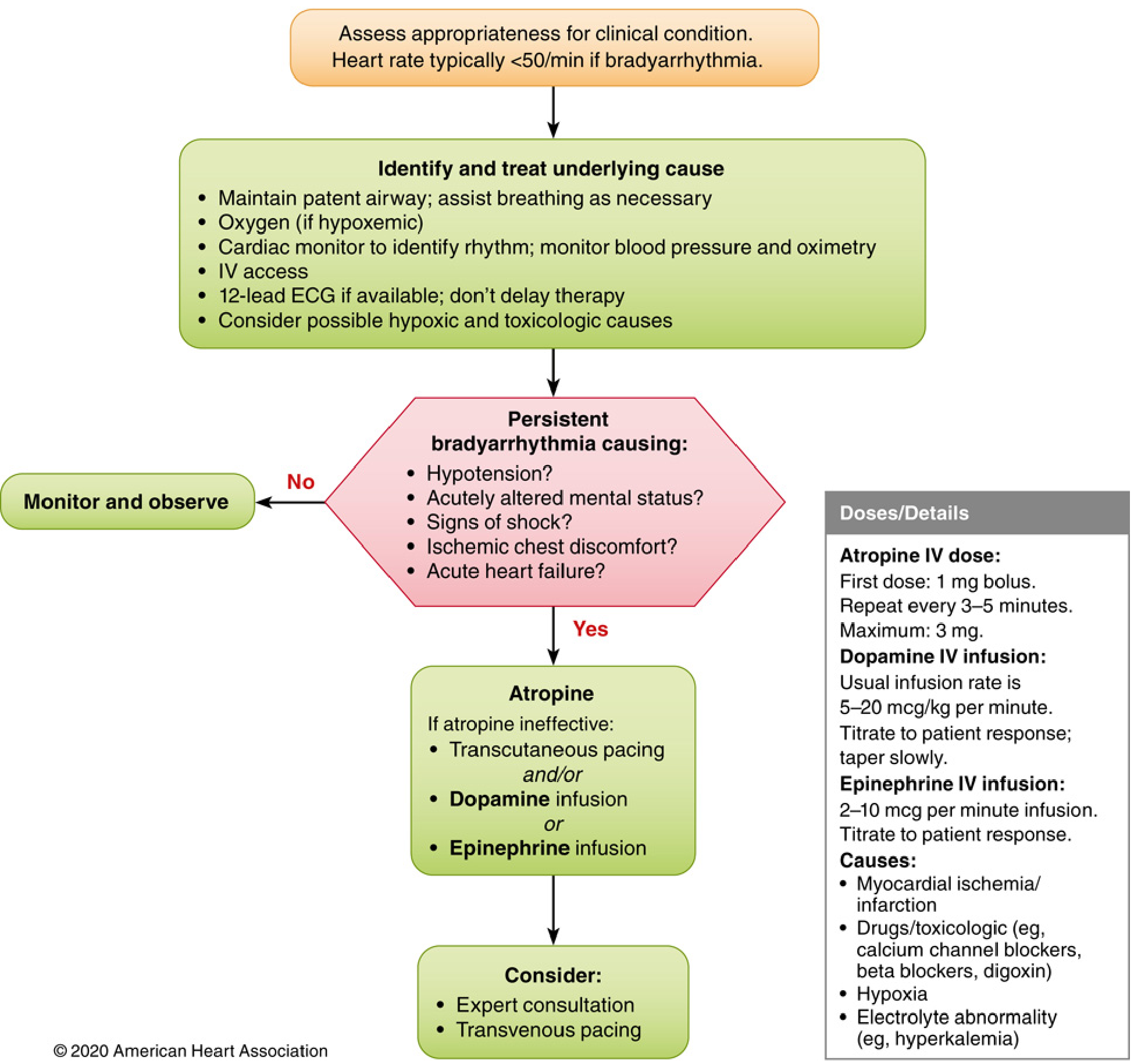
Drugs Used (Step-wise Approach per 2020 AHA Guidelines)
1. Atropine (First-line)
Mechanism: Competitive antagonist of muscarinic (M2) receptors → blocks vagal tone → ↑ SA node automaticity and AV conduction velocity
Spectrum of use:
- Acute symptomatic sinus bradycardia
- 1° AV block (vagally mediated)
- Mobitz type I (Wenckebach) 2° AV block
Dose: 1 mg IV every 3–5 min, max total dose 3 mg
Side Effects: Dry mouth, urinary retention, blurred vision, tachycardia, confusion (anticholinergic effects), paradoxical bradycardia at doses < 0.5 mg
Contraindications / Limitations:
- Not effective in transplanted hearts (denervated — no vagal input)
- Not preferred for Mobitz type II or 3° AV block (block is infranodal, not vagally mediated) — may worsen outcome
- Narrow-angle glaucoma, BPH (relative)
Interactions: Additive anticholinergic effects with other antimuscarinic drugs; antagonized by cholinesterase inhibitors (neostigmine)
2. β-Adrenergic Agonists (Second-line if atropine fails)
Dopamine
Mechanism: Stimulates β1 (and at higher doses α1) receptors → ↑ HR, ↑ contractility, vasoconstriction at high doses (>10 mcg/kg/min)
Dose: Low dose: selective inotropy/chronotropy; high dose: vasoconstriction
Epinephrine
Mechanism: α1 + β1 + β2 agonist → ↑ HR, ↑ contractility, vasoconstriction + vasodilation
Isoproterenol
Mechanism: Pure β1 + β2 agonist → ↑ HR, ↑ contractility + vasodilation (no α effect)
Dose: 2–10 mcg/min IV infusion, titrated to HR/rhythm response
Side Effects (β-agonists): Tachycardia, palpitations, hypertension (dopamine/epi), arrhythmias, myocardial ischemia, anxiety
Interactions: MAO inhibitors → markedly potentiate catecholamine effects (hypertensive crisis); β-blockers antagonize effects
3. Transcutaneous/Transvenous Pacing (Non-pharmacological)
- Used when pharmacotherapy fails or for Mobitz II / 3° AV block
- TCP is painful — sedation required in awake patients
- Definitive: transvenous pacing
Summary Table
| Drug | Mechanism | Indication | Key Contraindication |
|---|
| Atropine | Antimuscarinic (↓ vagal tone) | Sinus/junctional bradycardia, Mobitz I | Heart transplant, Mobitz II, 3° AV block |
| Dopamine | β1 > α1 agonist | Atropine-refractory bradycardia | Pheochromocytoma |
| Epinephrine | β1 + β2 + α1 agonist | Atropine-refractory, cardiac arrest | Relative: hypertension, arrhythmias |
| Isoproterenol | β1 + β2 agonist | Torsades, β-blocker OD, denervated heart | Coronary ischemia, tachycardia |
Figure: 2020 AHA Adult Bradycardia Algorithm. — Miller's Anesthesia
Sources: Lippincott Illustrated Reviews: Pharmacology; Miller's Anesthesia 10e; Braunwald's Heart Disease